52-year-old man who stumbled and fell to the ground. Lateral radiograph of the left knee. There is marked soft tissue swelling over the patella (arrowhead). There is a proximally distracted avulsion fracture fragment (arrow) from the superior pole of the patella, and the normal quadriceps tendon is not seen. The patella is positioned inferior to its normal position (patella baja). The patella is a sesamoid bone beneath the quadriceps tendon; these findings represent a complete tear of the quadriceps tendon superior to the patella (accounting for the soft tissue swelling) with proximal retraction and avulsion of a small fragment of the superior pole.
Case 11–2
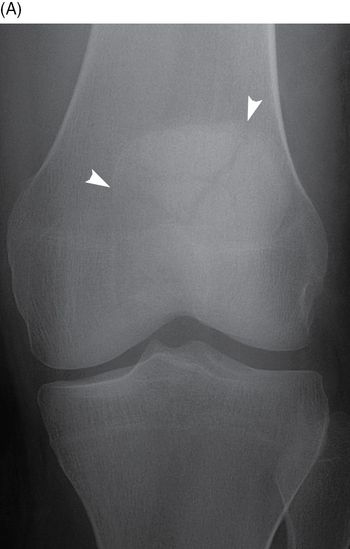
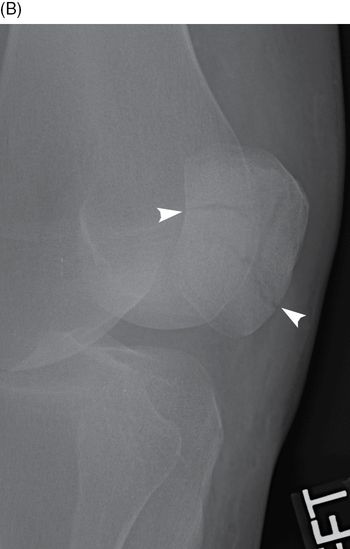
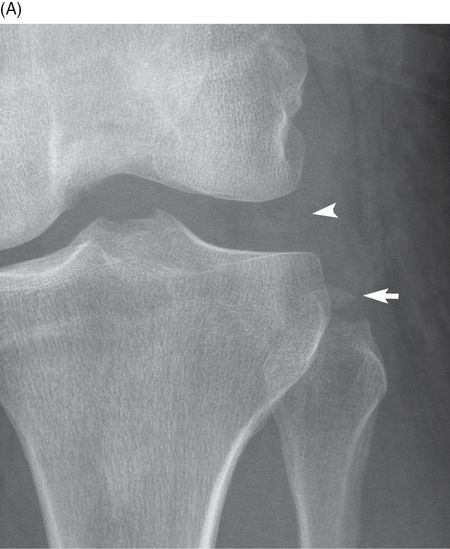
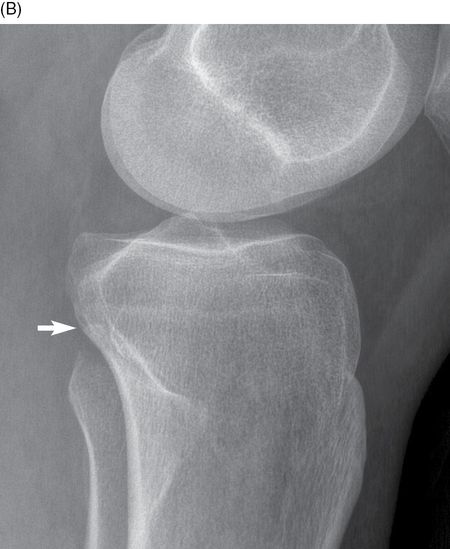
Transverse patella fracture


31-year-old man who injured his knee while snowboarding. AP (A) and cross-table lateral (B) radiographs of the left knee. There is a transverse fracture of the patella with gross distraction of the fragments. There is severe soft tissue swelling and a fat-fluid level anterior to the patella. This fracture pattern is associated with complete disruption of the quadriceps tendon as it passes over the anterior aspect of the patella. The quadriceps muscles retract the superior pole fragment while the infrapatellar tendon keeps the lower pole in place. Surgical repair is necessary to restore function to the quadriceps mechanism [1].
Case 11–3
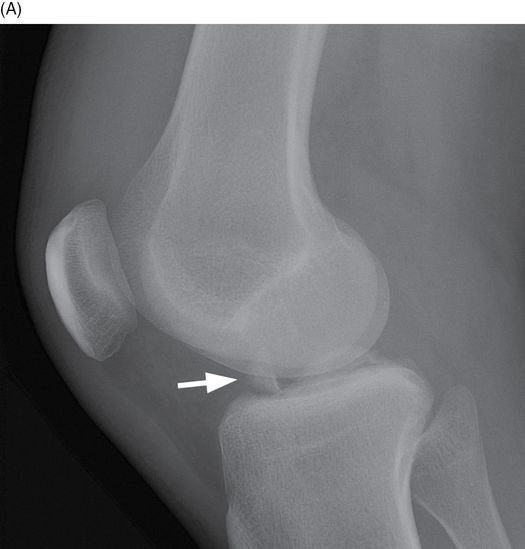
Patella avulsion fracture
19-year-old man who was struck by a car as a pedestrian. Lateral radiograph of the right knee. There is a mildly displaced avulsion fracture of the inferior pole of the patella. Soft tissue swelling is present superficially (arrowhead), but the extensor mechanism appears to be in continuity and the patella is normally positioned. If there is an associated with injury to the extensor tendon, it is not complete. There is also a minimally displaced fracture of the anterior margin of the lateral tibial plateau.
Case 11–4
Infrapatellar tendon rupture


25-year-old woman who was in a motor vehicle crash. Lateral (A) and AP (B) radiographs of the right knee. There is a laceration of the infrapatellar soft tissues (arrow), with gas in the Hoffa fat pad. The infrapatellar tendon has been transected and is not seen in its usual location. The patella is positioned superior to its normal position (patella alta). Other injuries are present, including fractures of the median eminence of the tibia (arrowhead).
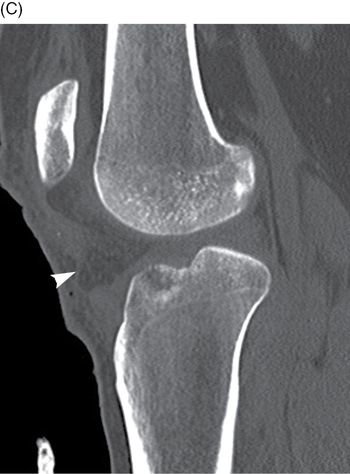


Sagittal CT of the right knee through the median eminence of the tibia, lateral (C) to medial (E). The infrapatellar tendon has been transected (arrowhead). There is a small amount of gas in the soft tissues inferior to the patella. There are comminuted fractures of the median eminence of the tibia. These fractures represent avulsions of the attachments of the cruciate ligaments.
Case 11–5
Stellate patella fracture
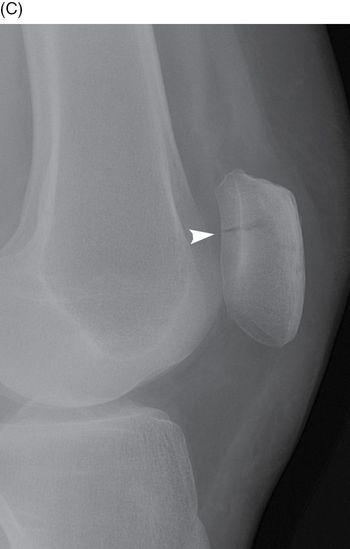
Adult who fell on knee. AP (A), oblique (B), and lateral (C) radiographs of the left knee. There is a stellate fracture (arrowheads) of the patella with minimal displacement. There is a joint effusion and overlying soft tissue swelling. This fracture pattern is the result of direct trauma to the patella; the quadriceps mechanism remains intact.
Case 11–6
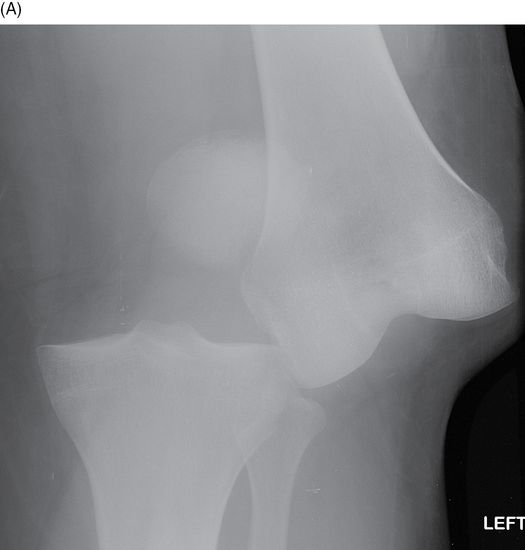
Lateral patella dislocation
37-year-old man whose patella popped out when he knelt down. AP radiograph of the left knee. The patella (arrowhead) is dislocated to a position just lateral to the femur. The articulation between the femur and tibia is normal. No fracture is seen. Most patellar dislocations occur with non-contact, low-energy flexion-valgus stress. The patella dislocates laterally and may be associated with a variety of soft tissue injuries, especially the medial patellofemoral ligament [2]. MRI may be appropriate to evaluate for concomitant osteochondral injury.
Case 11–7
Posterior knee dislocation


Adult in a high-speed motor vehicle crash. AP (A) and lateral (B) radiographs of the left knee. There is posterior dislocation of the knee. No definite fractures are evident. Severe ligamentous injuries accompany knee dislocations, typically including tears of the anterior and posterior cruciate ligaments [3]. Vascular injuries may also be associated with knee dislocation; a recent meta-analysis found a prevalence of 18% among all acute traumatic knee dislocation patients, with multi-ligament injuries and posterior dislocations as additional risk factors for vascular injuries [4].
Case 11–8
Anterior knee dislocation


44-year-old woman who tripped on the stairs and fell. AP (A) and lateral (B) radiographs of the left knee. There is anterior dislocation of the knee. No fractures are evident. Subsequent evaluation showed no vascular injuries but tears of anterior and posterior cruciate ligaments and medial and lateral collateral ligaments.
Case 11–9
Lateral knee dislocation


51-year-old man in a sky-diving mishap, losing lift 10 feet above the ground and landing awkwardly. AP (A) and lateral (B) radiographs of the left knee. There is lateral dislocation of the tibia relative to the femur, with the lateral tibial articular surface uncovered and the medial tibial articular surface aligned with the intercondylar notch of the femur. The patella has dislocated laterally with the tibia. The femur and tibia remain aligned in the coronal plane, as shown on the lateral view.
Case 11–10
Medial knee dislocation

30-year-old man involved in a motorcycle collision. AP (A) and lateral (B) radiographs of the left knee. There is medial dislocation of the tibia relative to the femur. The patella is medially dislocated from the trochlea, but remains aligned with the tibia. Subsequent MRI showed the expected severe multi-ligament injuries.
Case 11–11
Anterior tibial spine fracture

Young adult with a sports injury. Lateral (A) and AP (B) radiographs of the right knee. There is an avulsion fracture of the anterior tibial spine, a component of the median eminence of the tibia, which is indicative of avulsion by the anterior cruciate ligament [5]. There is knee joint effusion.
Case 11–12
Combined ACL-PCL avulsion fractures


59-year-old woman in a motorcycle crash. Lateral (A) and AP (B) radiographs of the right knee. There is an avulsion fracture of the anterior tibial spine, indicative of avulsion by the anterior cruciate ligament (short arrow). There is an avulsion fracture of the posterior margin of the tibia (long arrow) suggestive of avulsion by the posterior cruciate ligament. There is extensive soft tissue swelling. There is knee joint effusion.


Sagittal CT of the right knee through the median eminence, lateral (C) and medial (D). There is an avulsion fracture of the anterior tibial spine (short arrow). The anterior cruciate ligament (large arrow) is intact and attached to the fragment. There is an avulsion fracture of the posterior margin of the tibia (long arrow). The posterior cruciate ligament (arrowheads) is intact and attached to the fragment. There is extensive soft tissue swelling (*). There is knee joint effusion. In this case, the likely mechanism of injury was hyperextension.
Case 11–13
Segond fracture

Young adult with a sports injury. AP radiograph of the left knee. There is a small avulsion fragment at the lateral margin of the proximal tibia (arrow). This fracture corresponds to an avulsion of the lateral collateral ligament complex or lateral joint capsule, and is highly associated with tears of the anterior cruciate ligament [5]. A joint effusion is also present. MRI should be obtained to document the ACL tear and to identify additional injuries.
Case 11–14
Fibular styloid avulsion fracture (arcuate sign)
48-year-old woman who was struck by a car as a pedestrian. AP (A) and lateral (B) radiographs of the left knee. There is lateral joint space widening of the knee, indicative of ligamentous injury on the lateral side. There is an avulsion fracture of the styloid process of the head of the fibula, corresponding to an avulsion of the arcuate ligament. The arcuate ligament includes the fibular attachment of the lateral collateral ligament. When a pedestrian is struck in the knee by a car, the car has typically approached from the side and the knee may be forced into valgus or varus, depending on whether the impact is from the lateral or medial side of the knee, respectively.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


