
30-year-old man injured in motor vehicle crash. AP (A) and lateral (B) radiographs of the left ankle. There are bimalleolar ankle fractures. There is a talar neck fracture (arrow) with a small amount of comminution. The fracture enters the posterior facet of the subtalar joint. Talar neck fractures may be described using the Hawkins classification: Type I is a non-displaced fracture; Type II is associated with subtalar subluxation or dislocation; Type III is associated with subtalar and ankle dislocation.
Case 13–2
Talar extrusion


46-year-old man in 30-foot fall. Lateral (A) and AP (B) radiographs of the right ankle. The talus (T) is extruded in the medial direction from the ankle. This injury represents simultaneous medial dislocation of the ankle and lateral subtalar dislocation of the foot.


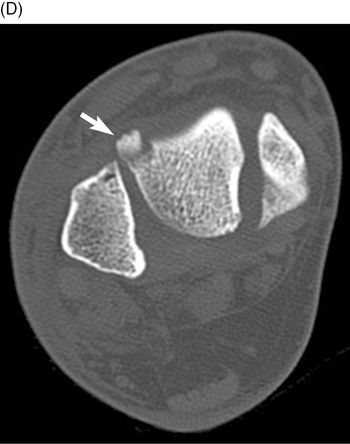
Coronal (C) and axial (D) CT images of the right hindfoot. There is moderate internal rotation and medial displacement of talus (T). The anterior medial aspect of the talus extrudes through an open wound in the soft tissues and skin (arrow). Accordingly, there is large amount of air within the ankle joint. There are multiple small bone fragments about the injury site, and an osteochondral fracture donor site on the lateral aspect of the head of the talus (arrow). Open talar fractures with extrusion of the talar body or even the entire talus are typically the result of high-energy trauma and are frequently associated with markedly displaced fractures, severe soft-tissue injury, contamination, and disruption of the talar blood supply [1–4].
Case 13–3
Talar extrusion


61-year-old woman in motor vehicle crash. AP (A) and lateral (B) radiographs of the right ankle. There has been complete medial extrusion of the talus, simultaneous medial dislocation of the ankle, and lateral subtalar dislocation of the foot. Talar extrusion is a rare injury. The talus can be extruded anteromedially, as in this case, or anterolaterally [5].
Case 13–4
Talar dome osteochondral fracture

24-year-old man in high-speed motor vehicle crash. Mortise radiograph of the right ankle. There is a mildly displaced fracture of the lateral corner of the talar dome (arrow). The lateral or medial corner of the dome of the talus may be compressed against the ankle mortise during the traumatic event [4]. These fractures may require CT or MR for visualization.


Multiplanar CT of the right ankle in coronal (B), sagittal (C), and axial (D) planes. The anterolateral corner of the talar dome is fractured with a small displaced fragment. The fragment includes the articular cartilage overlying the subchondral bone.
Case 13–5
Lateral process of talus fracture


Man injured in 20-foot fall. AP (A) and lateral (B) radiographs of the right ankle. There is a comminuted lateral process of talus fracture (arrow). There is diffuse soft tissue swelling.


Axial (C) and sagittal (D) CT of the ankle. There is a comminuted fracture of the lateral process of the talus (arrows), extending into the anterior medial aspect of the posterior facet. The lateral process of the body of the talus is a broad-based wedge-shaped prominence that articulates dorsolaterally with the fibula and inferomedially with the calcaneus, thereby forming the lateral part of the subtalar joint. Fracture of the lateral process is seen frequently in snowboarders [6]. Before the development of this sport, these fractures were rare and generally associated with motor vehicle accidents, falls from a height, or simple inversion injuries [7]. With the increasing popularity of snowboarding, fractures of the lateral process of the talus occur more frequently and account for 2.3% of snowboarding injuries.
Case 13–6

Case 13–7
Talus avulsion fractures

57-year-old woman with twisting injury to foot in motor vehicle crash. Lateral radiograph of the right ankle. There is a subtle dorsal avulsion fracture of talar neck (arrow).



Axial (B-C) and coronal (D) CT of the right ankle. There is a mildly comminuted fracture involving the medial margin of the talus with minimal displacement (large arrows). There is a minimally displaced fracture of the medial aspect of the navicular (arrowhead) and a small accessory navicular. There is a talar medial process avulsion fractures (long small arrow) and an avulsion fracture at the tip of the lateral malleolus (short small arrow).
Case 13–8
Medial subtalar dislocation


28-year-old woman sustained a twisting injury while playing basketball. AP (A) and lateral (B) radiographs of the right ankle. There has been gross medial dislocation of the foot from the talus. There are simultaneous dislocations of the talocalcaneal and talonavicular joints, an injury referred to as subtalar or peritalar dislocation. Following reduction, CT showed a few small avulsion fractures. Most subtalar dislocations are medial and may occur with low energy inversion or twisting, as in this case [8].
Case 13–9
Lateral subtalar dislocation


36-year-old woman injured in motor vehicle crash. Lateral (A) and AP (B) radiographs of the right ankle. The lateral view shows full overlap of the talus and the calcaneus. The AP view confirms that the talus and calcaneus are side-by-side rather than over-and-under, with the foot dislocated laterally. No more than 25% of subtalar dislocations are lateral [8]. The displaced bone fragment lateral to the distal fibula (arrow) is an avulsion fracture of the peroneal tendon sheath. The peroneal tendons were dislocated from their normal location along the posterior aspect of the distal fibula when the foot dislocated laterally, taking with them their sheath and its bony attachment.


Axial (C) and coronal (D) CT of the right ankle. CT scan following reduction shows comminuted fractures of the talus at the lateral aspect of the posterior facet of the subtalar joint (arrowheads). CT should be obtained following reduction to identify fractures that might be radiographically occult [9]. The patient subsequently had open reduction and internal fixation of her fractures.
Case 13–10
Intra-articular calcaneal compression fracture, centrolateral depression type
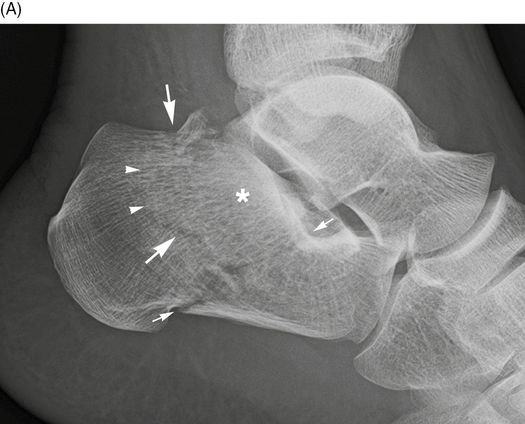

38-year-old man who fell from a height of 6 feet, landing on his feet. Lateral (A) and axial (B) radiographs of the left calcaneus. There is a comminuted calcaneal fracture with the primary fracture line extending through the posterior subtalar facet to the plantar surface (small arrows) and a secondary fracture line exiting vertically just posterior to the posterior subtalar facet (large arrows). The major posterior facet fragment (asterisk) is impacted into the calcaneal tuberosity resulting in a zone of sclerosis where the trabecular bone has been crushed together (arrowheads). Calcaneal fractures may be divided into those that involve the posterior facet of the subtalar joint (intra-articular) and those that do not (extra-articular). Accordingly, extra-articular calcaneal fractures may involve articular surfaces that are not the posterior subtalar facet.


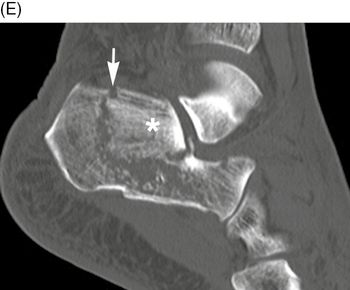
Sagittal CT of the left calcaneus, medial (C) to lateral (E). The primary fracture line (small arrows) begins at the angle of Gissane (also called critical angle) and extends to the plantar surface at the calcaneal tuberosity. A secondary fracture line extends posterior to the posterior subtalar facet (large arrows). There are two major posterior subtalar facet fragments (asterisks). Depression of the posterior facet fragments into the body of the calcaneus has crushed the trabecular bone (arrowheads).
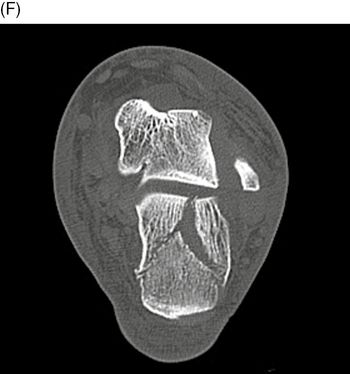
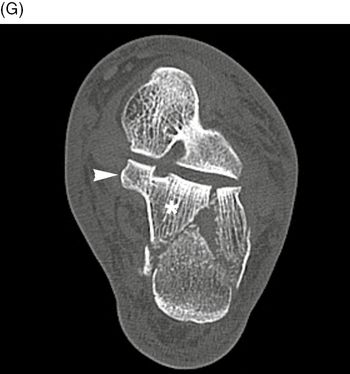
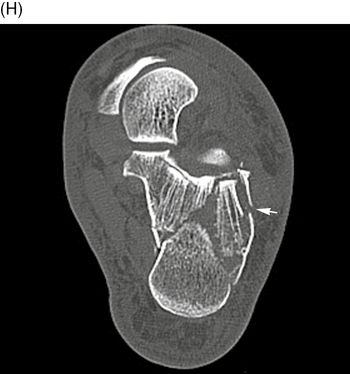
Axial CT of the left calcaneus, superior (F) to inferior (H). Comminuted fractures separate the posterior subtalar facet of the calcaneus into a medial fragment (asterisk) that includes the sustentaculum tali (arrowhead) and a lateral fragment. There is further comminution of the lateral fragment (small arrow). In the classification of Essex-Lopresti for intra-articular fractures [10–11], compression of the talus into the calcaneus splits the calcaneus through the posterior facet into an anteromedial fragment that includes the sustentaculum and a posterior tuberosity fragment. A secondary fracture may appear posterior to the facet (centrolateral compression type) or may appear in the posterior tuberosity (tongue type). This case is an example of a centrolateral compression type intra-articular calcaneal fracture.
Case 13–11
Intra-articular calcaneal compression fracture, tongue type


47-year-old man who fell from an 8-foot height. Lateral (A) and axial (B) radiographs of the left calcaneus. There is an impacted calcaneal fracture with the fracture line vertically extending to the posterior facet (arrows), and horizontally extending to the tuberosity (arrowhead). The principal fragment of the posterior facet (asterisk) contains the upper portion of the tuberosity, and this fragment is called the tongue fragment (T). This intra-articular fracture is designated as a tongue type calcaneal fracture.



Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


