Elderly woman injured in ground-level fall. AP radiograph of the left hip. There is a subcapital fracture of the femoral neck with impaction of the superior cortex (arrow) and minimal displacement at the inferior cortex (arrowhead). A major goal of surgical therapy for fractures such as this is to restore mobility to the patient. Approximately 80% of hip fractures in elderly patients occur in women [1]. The Garden classification for femoral neck fractures is related to the degree of valgus displacement: Type I is impacted (sometimes incomplete) and valgus; Type II is non-displaced (but complete); Type III is varus angulation but only minimal displacement; Type IV is displaced. This case is an example of Garden Type I.
Case 10–2
Displaced subcapital femoral neck fracture

54-year-old man with severe left hip pain, unable to walk. AP radiograph of the right hip. There is a complete subcapital fracture of the femoral neck with varus angulation of the shaft relative to the head, and proximal translation of the neck relative to the head. The risk of osteonecrosis of the femoral head fragment is high when the fracture is displaced. Therefore, fractures such as these are usually treated with hip replacement. This case is an example of Garden type IV.



Coronal CT of the right hip, anterior (B) to posterior (D). The inferior portion of the neck is proximally translated and impacted into the middle of the head fragment. The separation of the superior margins of the head and neck fragments reflects the varus angulation of the shaft fragment relative to the head fragment.
Case 10–3
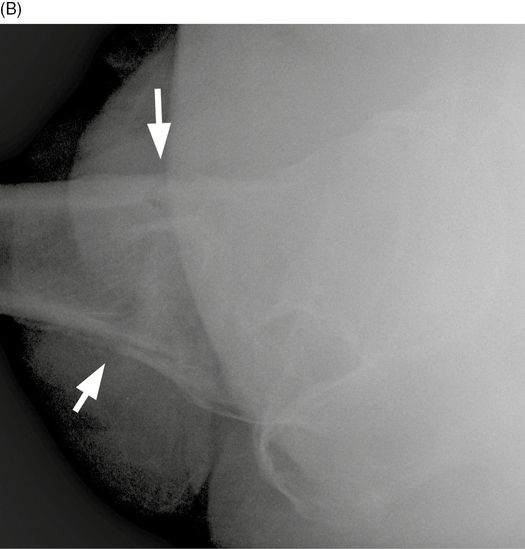
Transcervical femoral neck fracture


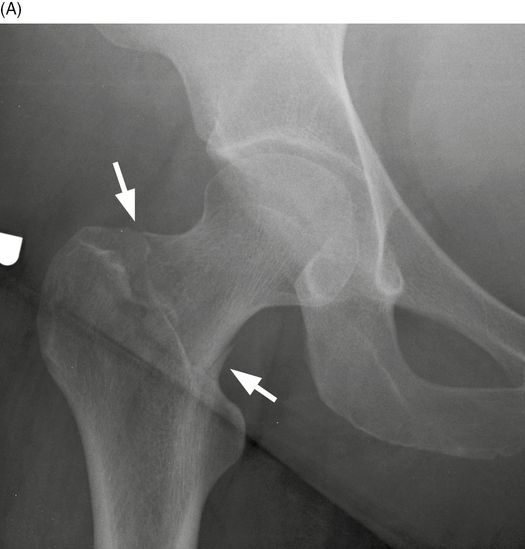
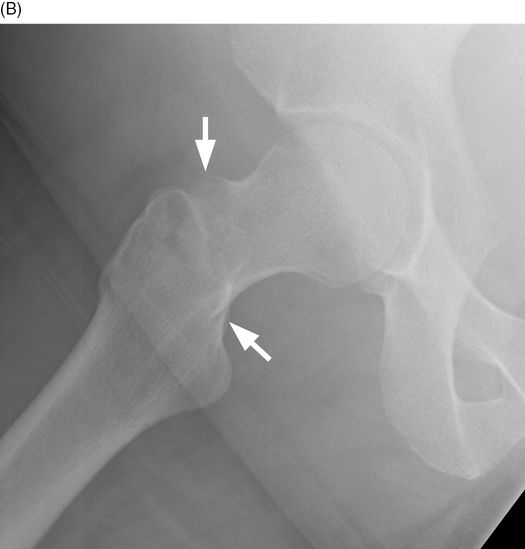
Elderly man injured in ground-level fall. AP (A) and lateral (B) radiographs of the right hip. There is apparent external rotation of the right proximal femur that makes the fracture easy to overlook because the greater trochanter is overlapping the femoral neck. In the appropriate clinical setting, asymmetry of hip rotation when compared with the contralateral side (not shown) should prompt further investigation. The fracture itself is difficult to see (arrowhead). Cross-table lateral radiograph of the right hip shows the fracture (arrow) extending through the middle of the femoral neck.
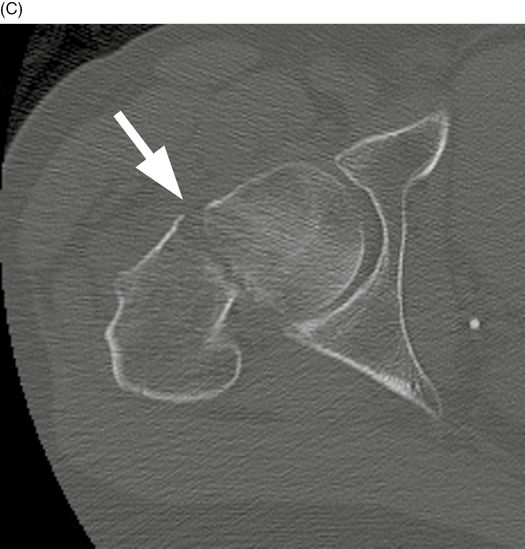
Axial CT of the right hip at the level of the femoral neck. There is a fracture traversing the femoral neck. The fracture is more displaced anteriorly (arrow) than posteriorly because of the greater external rotation of the distal fragment (including the shaft and trochanters) relative to the proximal fragment (including the neck and head).
Case 10–4
Basicervical femoral neck fracture
Middle-aged woman injured in a fall while in the bathroom. AP radiograph of the right hip. There is a fracture (arrow) extending along the base of the femoral neck.
Frog lateral radiograph of the right hip. The fracture (arrows) extends through the base of the femoral neck, but does not involve the trochanters.
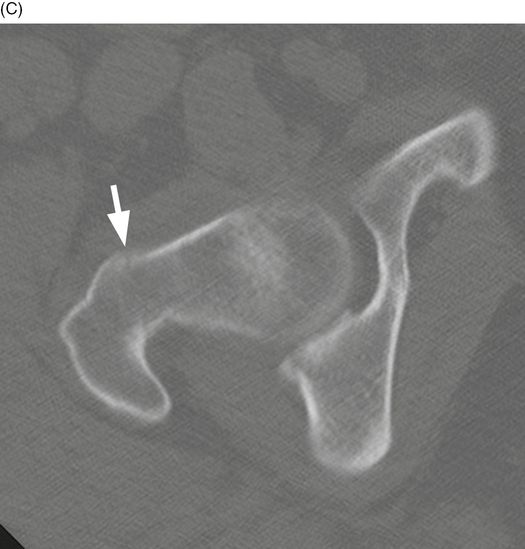
Axial CT of the right hip at the level of the femoral neck. The fracture (arrows) traverses the base of the femoral neck, medial to the greater trochanter.
Case 10–6
Intertrochanteric fracture

Elderly woman injured in a fall from standing. AP radiograph of the right hip. There is a fracture (arrows) extending obliquely from the greater trochanter to the lesser trochanter. The fracture is lateral to the base of the femoral neck. The right hip is externally rotated.
Cross-table lateral radiograph of the right hip. This view does not show the fracture (arrows) very well. The risk of osteonecrosis of the femoral head as a complication of an intertrochanteric fracture is low because the fracture is outside of the hip capsule and extends through cancellous bone with a good blood supply [2].
Case 10–7
Intertrochanteric femur fracture, comminuted


50-year-old woman injured in bicycle accident. AP (A) and true lateral (B) of the left hip. There is a comminuted intertrochanteric fracture of the proximal femur with comminution of the greater trochanter and subtrochanteric extension. There is varus angulation and medial displacement of the shaft.


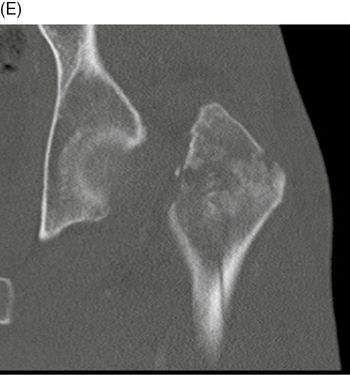
Coronal CT of the left hip, anterior (C) to posterior (E). The major head-neck fragment is impacted into the major shaft fragment. There is comminution of the greater trochanter, but the lesser trochanter is part of the shaft fragment. There are minimally displaced fractures extending into the proximal shaft.
Case 10–8
Intertrochanteric femur fracture, comminuted
27-year-old man in a motorcycle crash. AP radiograph of the left hip. There is a three-part intertrochanteric fracture with displaced lesser trochanter fragment (arrow). Most hip fractures in adults aged 40 years or younger are the result of high-energy trauma such as motor vehicle crashes.
Case 10–9
Intertrochanteric femur fracture, comminuted


Elderly woman injured in ground-level fall. AP (A) and cross-table lateral (B) radiographs of the left hip. There is a four-part intertrochanteric fracture of the left proximal femur. The lesser (arrows) and greater (arrowheads) trochanters are separate fragments; the head and neck comprise another fragment; the shaft is the fourth fragment. Intertrochanteric fractures tend to occur in young adults with high-energy trauma and in very elderly adults with low-energy trauma. Unlike subcapital fractures, for which there is a strong preponderance of women, intertrochanteric fractures in very elderly patients have equal incidence between men and women.
Case 10–10
Intertrochanteric-subtrochanteric (peritrochanteric) femur fracture
72-year-old man in rollover tractor accident. 3D volume-rendered CT of the left hip. There is a four-part intertrochanteric fracture that extends to the subtrochanteric portion of the femoral shaft, with wide displacement.
Case 10–11
Bilateral subtrochanteric femur fractures
Young man in high-speed motor vehicle crash. AP radiograph of the pelvis. There are bilateral subtrochanteric femoral shaft fractures with proximal and medial displacement. The proximal femurs are abducted by the gluteus medius and gluteus minimus; the shaft is pulled proximally by the thigh adductors. Subtrochanteric fractures have a bimodal distribution – that is, typically young men from severe trauma and elderly women from ground-level falls.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


