5-year-old girl who fell onto her outstretched hand. PA radiograph of the right hand. There is fracture of the proximal phalanx of the small finger. The fracture passes through the growth plate such that the epiphysis (arrowhead) is slightly offset from the shaft of the proximal phalanx. There is a metaphyseal fragment (arrow) that has displaced with the epiphysis. There are five types of fractures involving the growth plate according to the Salter-Harris classification [1]: Type I fractures pass the growth plate only; Type II fractures pass through the growth plate and the metaphysis; Type III fractures pass through the growth plate and the epiphysis; Type IV fractures pass through the growth plate and both metaphysis and epiphysis; Type V fractures are crush fractures of the growth plate.
Case 16–2
Metacarpal torus fracture


15-year-old male who fell while skiing. Oblique (A) and PA (B) radiographs of the right first metacarpal. There is a torus fracture (arrow) of the proximal shaft of the first metacarpal. The fracture does not involve the nearby physis or joint.
Case 16–3
Scaphoid fracture
Child who fell on an outstretched hand. PA radiograph of the left wrist. There is a non-displaced waist of scaphoid fracture (arrow) that was seen only on the PA projection. Scaphoid and other carpal bone fractures are infrequent in young children, possibly because the bones are incompletely ossified and are cushioned by cartilage. In the immature skeleton, distal radius fractures are the predominant fractures of the wrist [2].
Case 16–4
Distal radius fracture, salter Type I



12-year-old girl who fell while attempting a back walkover maneuver on the balance beam, landing on her outstretched wrist. PA (A), oblique (B), and lateral (C) radiographs of the right wrist. There is widening of the distal radial physis laterally (arrow) indicative of a Salter I injury. The bones tend to be stronger in adolescents compared to young children, therefore, while younger ages have radial metaphyseal buckle fractures, adolescents tend to have fractures involving the growth plate rather than the bone, with the majority of wrist fractures in adolescents being Salter I (22%) or Salter II (58%) injuries [3]. A chronic stress injury seen in gymnasts can produce a Salter I injury, which is, however, accompanied by irregularity and sclerosis [4]. Premature physeal closure, radial shortening, and positive ulnar variance may be sequelae of so-called gymnast wrist [5]. (Source: Chew FS. Skeletal Radiology: The Bare Bones. 3rd Edition. Copyright © 2010 by Felix Chew.)
Case 16–5
Distal radius fracture, salter Type II



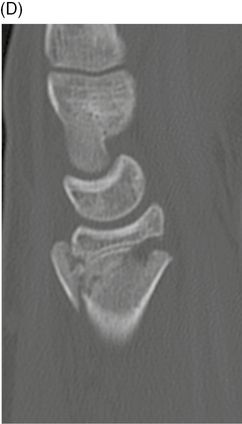
15-year-old male who fell on an outstretched hand. Coronal (A-B) and sagittal (C-D) CT of the right wrist. Coronal CT images show an impacted fracture of the distal radius with comminution of the metaphysis. The fracture extends through the growth plate and there is an accompanying ulnar styloid avulsion fracture. The sagittal CT images show impaction and dorsal angulation of the distal fragment. Ogden [6] extended the Salter-Harris growth plate fracture classification with additional types of periphyseal injuries: Type VI is a peripheral perichondral ring injury (usually open); Type VII is a fracture of the epiphysis only; Type VIII is a metaphyseal fracture; and Type IX is a diaphyseal fracture. The distal radius fracture can be classified as a Salter Type II, and the ulnar styloid fracture can be classified as an Ogden Type VII.
Case 16–6
Buckle fracture of distal radius


8-year-old girl who fell on her outstretched hand. PA (A) and lateral (B) radiographs of the left wrist. There is buckling of the metaphyseal cortex (arrows), involving primarily the dorsal cortex. If the buckling involved the bone circumferentially, it would have the shape of a torus (similar to a donut). This injury is commonly called a buckle fracture or a torus fracture, with these terms being essentially interchangeable. Children’s bones are more pliable, and therefore are more prone to incomplete fractures. Buckle fracture, greenstick fracture, and plastic bowing deformity represent incomplete fractures unique to children. Greenstick and plastic deformity occur from bending (angulation) forces. Fracture occurring on the tension (convex) side of the bone and not the compression side (concave) gives rise to the greenstick fracture. The tension side would be expected to fail first, as bone is weaker to tension forces compared to compression forces. The mechanism of injury for buckle and torus fractures is compression from axial loading [7].
Case 16–7
Plastic bowing deformity of ulna


Child who fell on an outstretched hand. Lateral (A) and AP (B) radiographs of the right forearm. Plastic bowing of the ulna and complete fracture of the mid-radius is seen. Bending of the bone with low force is reversible and constitutes elastic deformity. More intense force gives rise to fractures. Forces that exceed those in reversible bending, but fall short of that required to produce a fracture may result in a plastic bowing deformity in children, owing to the increased pliability of their bones. In older children, where much further growth is not anticipated, the deformity will not correct itself and reduction is necessary. Bowing deformity may only be manifest in only one of the two standard radiographic projections, and may therefore be overlooked.
Case 16–8
Greenstick fractures of the forearm


Child who fell on an outstretched hand. PA (A) and lateral (B) radiographs of the right distal forearm. There is an incomplete fracture with cortical break on the tension side and plastic deformity on the compression side in the mid to distal radius and ulna with ulnar angulation, consistent with greenstick fractures. Greenstick and bowing fractures are unique to children, owing to the greater pliability of their bones. When only a single forearm bone is involved, the proximal and distal radioulnar joints are more prone to injury. Isolated ulnar greenstick fracture may represent a Monteggia fracture equivalent where there has been spontaneous radial head reduction.
Case 16–9
Both bones forearm fractures


12-year-old boy who fell on an outstretched hand. PA (A) and lateral (B) radiographs of the left distal forearm. On the AP radiograph, there are transverse fractures of the shafts of both the distal radius and distal ulna, neither of which involves the growth plate nor the joint. The lateral radiograph shows that the fractures are dorsally displaced in bayonet apposition, with mild dorsal angulation of the distal fragments. Fractures caused by falls onto an outstretched hand in children are different than those in adults. In children, they are typically growth plate, buckle, or both bones fractures of the distal forearm. In adults, this mechanism is more likely to result in intra-articular fractures of the distal radius or carpal bones.
Case 16–10
Radial head subluxation (nursemaids’ elbow)


Child who fell while being led by the hand. AP (A) and lateral (B) radiographs of the right elbow. The radius and capitellum should be collinear on all radiographic projections. In this case, the position of the radial head, which is not yet ossified, can be estimated by a line drawn through the axis of the radial neck, which should point directly at the capitellum. Because the line falls posterior to the capitellum, there is posterior subluxation of the radial head. This is known as nursemaids’ elbow. The mechanism is from pulling a toddler’s hand by an adult. Before 5 years of age, the annular ligament is relatively lax and the radial head may subluxate when the forearm is pronated and pulled [8]. Supination and flexion may return the radial head to its proper location, and therefore the initial subluxation may be undetected on radiographs when interval supination has occurred.
Case 16–11
Supracondylar humerus fracture


5-year-old boy injured in fall. Lateral (A) and AP (B) radiographs of the left elbow. There is a joint effusion, manifested by posterior fat pad sign (arrowhead) and elevation of the anterior fat pad (small arrow). The fracture (arrows) itself may be difficult to see on radiographs. The fracture traverses the condyles and passes across the olecranon and coronoid fossae. The mechanism is fall on an outstretched hand. These are among the most common fractures seen in children. A potential complication is radial artery injury with Volkmann’s contracture of the forearm and hand. The posterior fat pad sign is highly associated with fracture (70–90%) in children and adolescents [9–11].

Lateral radiograph of the right elbow. Contralateral elbow obtained for comparison is normal. Supracondylar fractures are posteriorly angulated relative to the normal alignment of the distal humerus, but because the normal distal humerus is itself anteriorly angulated, the abnormal angulation of the distal fragment may not necessarily be angulated relative to the humeral shaft. A line drawn along the anterior cortex of the distal humeral shaft (anterior humeral line) would normally intersect the middle third of the capitellum (long, long arrow). If the anterior humeral line intersects the anterior third of the capitellum or misses it altogether, a posteriorly angulated fracture is presumably present [12].
Case 16–12
Lateral condylar humerus fracture
Primary school-aged child who fell. AP radiograph of the left elbow. There is a fracture at the lateral condyle, beginning at the lateral aspect of the metaphysis (arrow) and extending medially to the midportion of the humerus (arrowhead) and then distally into the cartilaginous portion of the epiphysis (Salter Type IV). After supracondylar fractures, lateral condylar fractures are the next most frequent elbow fractures and make up 15–20% of childhood elbow injuries [1, 13]. The fracture fragment includes the lateral metaphysis, capitellum, and lateral trochlea. A fall on an outstretched hand with forearm supination and elbow varus angulation is the mechanism. Pull from the extensor attachment at this site contributes to the fracture and may cause distal and posterior displacement of the fragment. The oblique view is best suited for detecting this fracture. (Source: Chew FS. Skeletal Radiology: The Bare Bones. 3rd Edition. Copyright © 2010 by Felix Chew.)
Case 16–13
Medial epicondyle humerus fracture


11-year-old boy injured in fall while playing basketball. AP (A) and lateral (B) radiographs of the right elbow. There is posterior dislocation of the elbow. At the medial aspect of the distal humerus, the apophysis of the medial epicondyle is absent (arrow). At this age, all of the apophyseal and epiphyseal centers should be ossified. On the lateral view, the displaced medial epicondyle is partially visible (arrowhead).

AP radiograph of the right elbow following reduction of the elbow dislocation. The elbow has been reduced. However, the medial epicondyle has only been partially reduced, and multiple fragments are now evident (arrowhead). The common flexor-pronator tendons and medial ulnar collateral ligament originate at the medial epicondyle. As such, it is extra-articular and may be injured without resulting in an elbow effusion [14]. The medial epicondyle is an apophysis, because it does not participate in increasing bone length. Repetitive valgus force with traction from the flexor-pronator tendons may give rise to a chronic avulsion injury, a condition known as little leaguer’s elbow, owing to its historical frequency in child baseball pitchers.
Case 16–14
Medial epicondyle humerus fracture
13-year-old girl injured during gymnastics. AP radiograph of the left elbow. An elbow dislocation (not shown) was been previously reduced before this radiograph was obtained. There is a displaced avulsion fracture of the medial epicondyle (arrow), with proximal retraction and marked overlying soft tissue swelling. There is also an avulsion fracture at the proximal attachment of the ulnar collateral ligament (arrowhead). A potential complication is entrapment of the avulsed ossification center in the joint when reduction is attempted. The ulnar nerve, which runs posterior to the medial epicondyle, may also be injured. Note that at this age in an adolescent female, some but not all of the epiphyseal and apophyseal ossification centers have closed.
Case 16–15
Clavicle fracture
Newborn girl who was not moving her right arm following vaginal delivery. AP radiograph of the right clavicle. There is an acute displaced mid-shaft fracture of the clavicle. The clavicle is the most commonly fractured bone during vaginal birth, with an incidence of about 0.5% [15]. They may be initially undetected [16].
Case 16–16
Atlanto-occipital dissociation
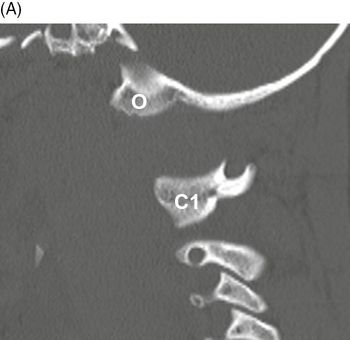
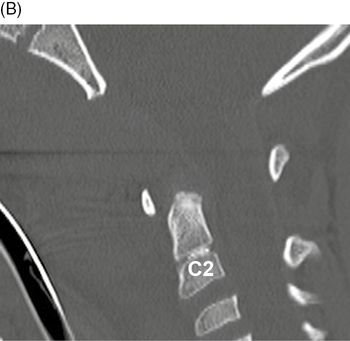
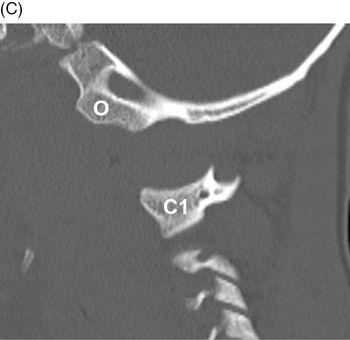
5-year-old child retrieved from severe motor vehicle crash. Sagittal CT of the upper cervical spine, left (A) to right (C). The skull is separated from the cervical spine. There is marked retropharyngeal soft tissue swelling, as demarcated by the endotracheal tube. The left (A) and right (C) occipital condyles are dislocated from the superior articular facets of C1, and separated by approximately 15 mm. The midline image (B) shows marked displacement of the skull base from the top of the cervical spine. The patient did not survive. Atlanto-occipital dissociation is more common in children than adults owing to smaller occipital condyles, larger relative head size, and weaker soft tissue supports.
Case 16–17
Jefferson fracture C1

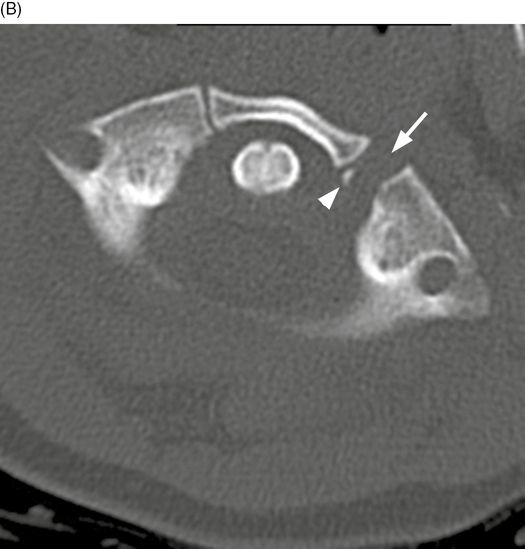
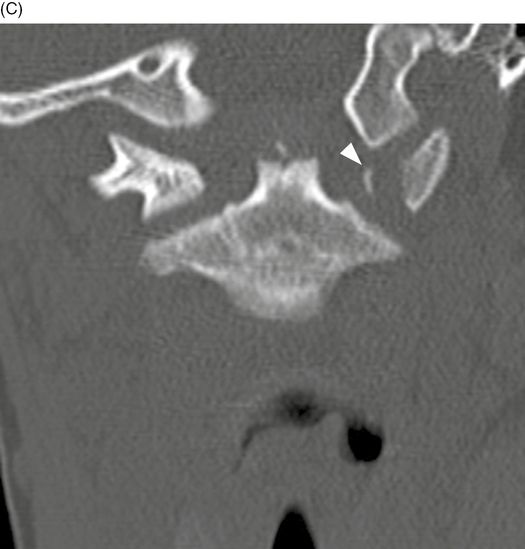
5-year-old child who fell on his head. Axial (A-B) and coronal (C) CT of the upper cervical spine. There is separation of the left anterior C1 synchondrosis (arrow) on the left side. There is a minimally displaced fracture through the posterior arch of C1 (short arrow). Axial CT image shows an avulsion fracture fragment (arrowhead) and separation of the synchondrosis (arrow) on the left side. Coronal CT image shows the avulsion fracture fragment (arrowhead) at C1 on the left.
Case 16–18
Odontoid fracture, Type I


10-year-old child who was struck by a car. Coronal (A) and axial (B) CT of the upper cervical spine. There is a small, laterally displaced, avulsion fracture fragment (arrow) at the tip of the odontoid process. Axial CT image through the ring of C1 shows a small, laterally displaced, avulsion fracture fragment (arrow) at the tip of the odontoid process. Anderson and D’Alonso Type I fractures of the odontoid process are very rare. The mechanism of injury is thought to be an avulsion of the ligamentous attachments of the odontoid process. A pedestrian child struck by a car from the left is likely to suffer severe left lateral flexion of the upper cervical spine, perhaps explaining this right-sided Type I odontoid fracture.
Case 16–19
Vertebral body fractures C6-C7
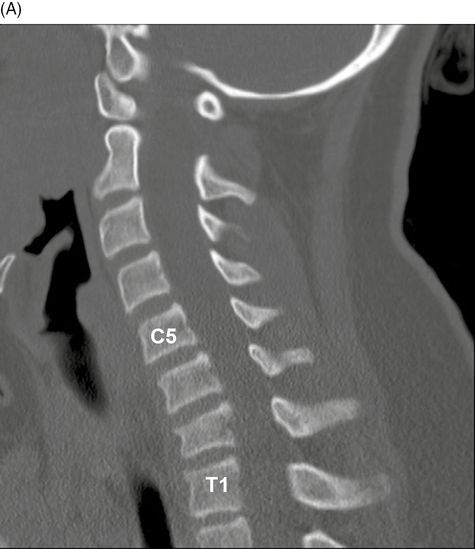

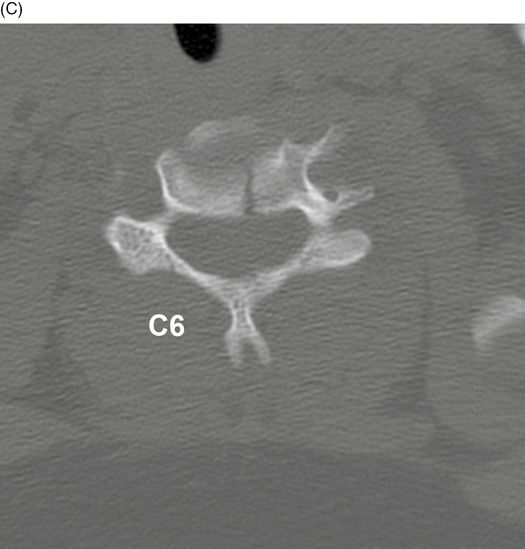
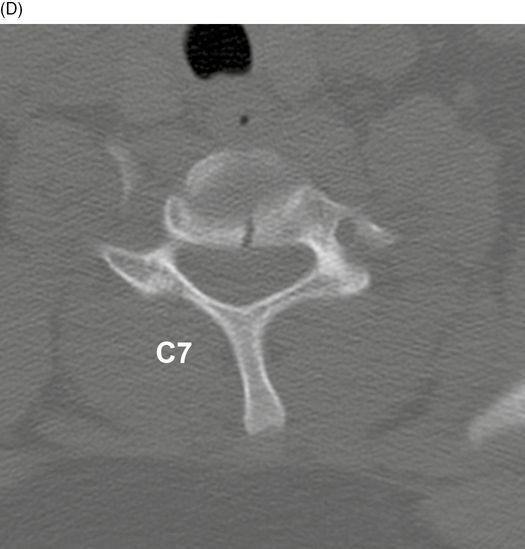
12-year-old girl who hit a metal pipe with her head while sledding. Sagittal (A), coronal (B), and axial (C-D) CT of the cervical spine. A fracture in the sagittal plane divides the C6 and C7 vertebral bodies in half. Compressive forces in this plane cause acute intervertebral disc herniation, which is responsible for this fracture pattern. This is a subtle fracture that may be occult on lateral radiographs and difficult to identify even on the AP radiographs. CT should be obtained when cervical spine fracture is suspected. 44% of cases of flexion teardrop also demonstrate sagittal fractures. Usually, 2 levels are involved. There is a high association of sagittal vertebral body fractures in the cervical spine with spinal cord injury [17].
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


