Sonoanatomy popliteal fossa. CPN, common peroneal nerve; TN, tibial nerve: both nerves constitute the sciatic nerve. PA, popliteal artery.
The sciatic nerve’s whole length can be visualized sonographically, from the gluteal crease to its division in popliteal fossa. The nerve lies deep in the subgluteal region, becoming more superficial as it descends. The hyperechoic and oval structure of the sciatic nerve is located between the biceps femoris and the gluteus muscles at this level (Figure 13.2). The greater trochanter appears hypoechoic and lateral to the sciatic nerve.
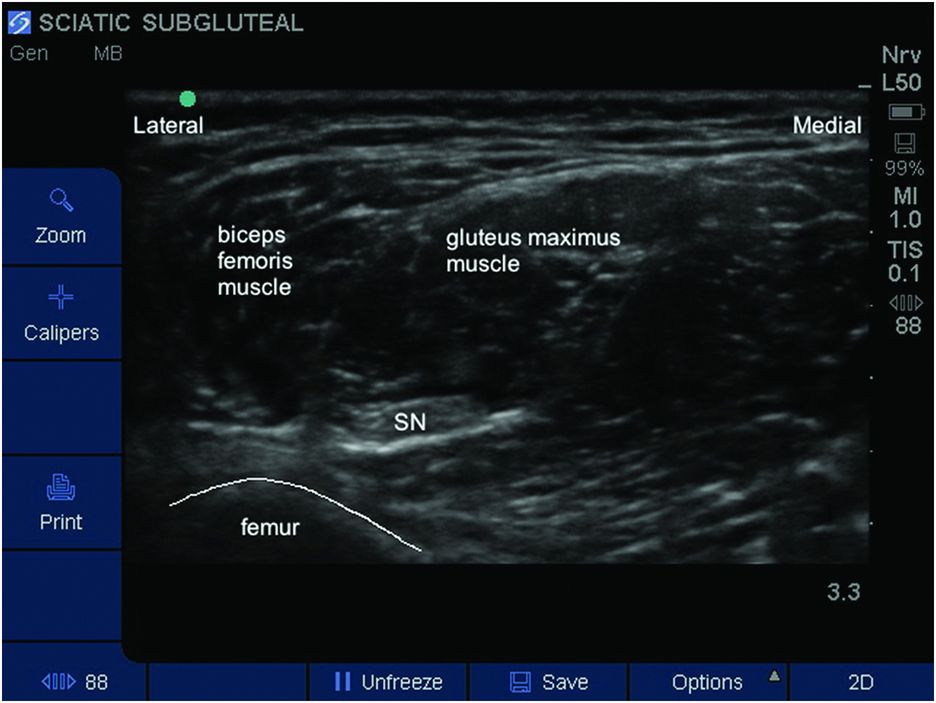
Sonoanatomy subgluteal region. SN, sciatic nerve.
Leaving the subgluteal region, the nerve runs between the long head of the biceps femoris (laterally) and the adductor magnus (medially) muscles initially. In the popliteal region the sciatic nerve is located between the biceps femoris laterally and the semi tendinous and semi membranous muscles medially. The popliteal artery runs medially and more superficial than the sciatic nerve and is of limited use in locating the nerve sonographically (Figure 13.1). It can, however, be used to locate the tibial nerve distally and then the tibial nerve can be followed cephalad to where it separates from the common peroneal nerve. The tibial nerve appears as a hyperechoic structure. The common peroneal nerve is smaller and more hypoechoic than tibial nerve, and runs more laterally.
Landmarks
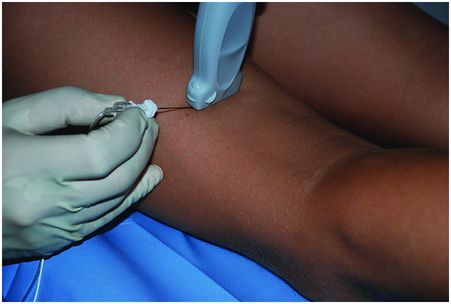
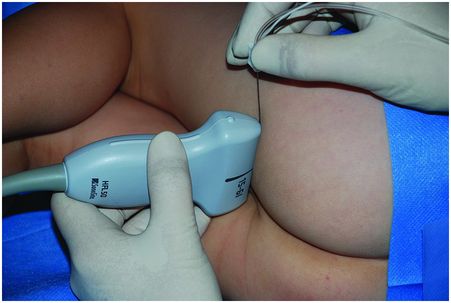
To visualize the sciatic nerve for the popliteal approach, the patient can be placed in the lateral, prone, or supine position. The supine position has advantages in children as positioning anesthetized patients in the prone or lateral positions may be difficult and may compromise the airway. In the supine position the probe must be positioned under the flexed knee and a lateral needle approach taken (Figure 13.3). In the prone or lateral positions the probe is placed in the region of the popliteal fossa and an in-plane or out-of-plane approach taken for needle insertion (Figure 13.4). A flexed knee in either position assists in identifying the muscle landmarks.

Probe placement for lateral popliteal block.
Probe placement for posterior popliteal block.
To visualize the sciatic nerve for the subgluteal approach, the patient can be placed in the lateral or prone position. The probe is then placed in the subgluteal region, below the cleft of the buttock (Figure 13.5).
Probe placement for subgluteal approach for sciatic nerve block.
Block performance
To perform either the subgluteal or the popliteal block, a linear high frequency probe is recommended. For older or obese children, a curved array probe can be required to perform the subgluteal block because of the deeper structures. In the infant population, the use of a “hockey-stick” probe is recommended (Ponde et al., 2013). Depending on the age of the child, the needle length is between 50 and 80 mm.
Popliteal block
For both the lateral and supine positions, the probe is placed transversally to the long axis of leg in the popliteal region. If the sciatic nerve is difficult to locate, the probe can be placed at the popliteal skin crease and the tibial nerve located because of its proximity to the popliteal artery. Then, the tibial nerve is followed by a cephalic movement of the probe until it converges with the common peroneal nerve to form the sciatic nerve.
If an in-plane needle approach is used, the needle is usually inserted through the lateral side of the thigh, between the vastus lateralis muscle and tendon of biceps femoris.
The orientation of the needle must be in line with the transverse probe position. The tip and shaft of the needle must be visualized during the block performance until the targeted nerve is approached (Figure 13.6). The local anesthetic (LA) is injected around the sciatic nerve; the spread of the LA must be seen as hypoechoic and ideally circumferential. The injection of LA may highlight the separate tibial and common peroneal components of the sciatic nerve and additional needle manipulation may be necessary to deposition sufficient LA around each nerve.
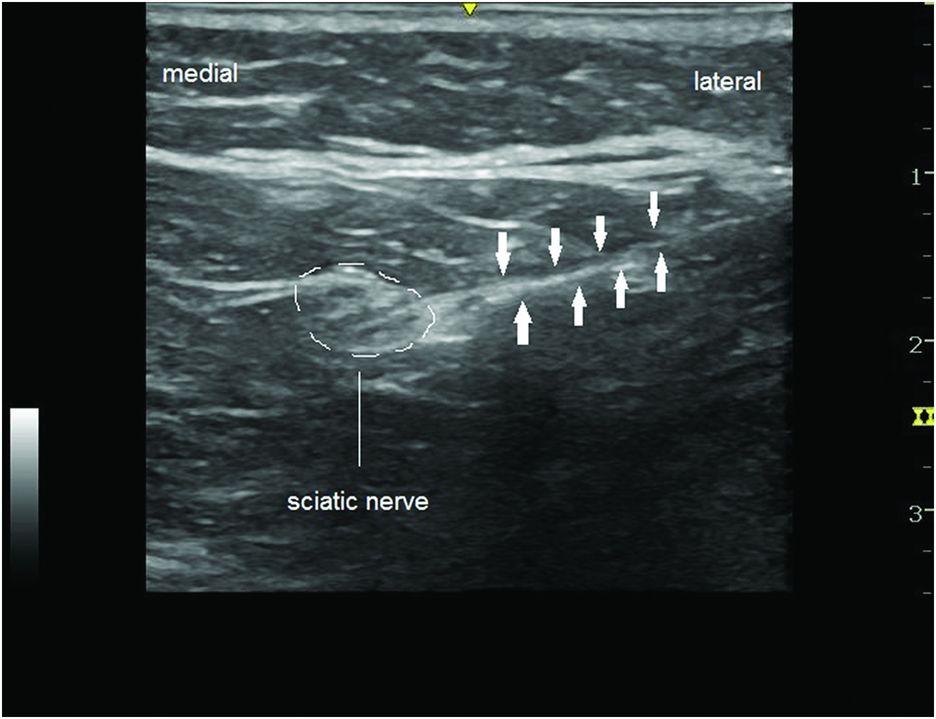
In-plane needle approach for lateral popliteal block. Needle is indicated by arrows.
For insertion of a peripheral nerve catheter, some prefer to use an out-of-plane approach to insert the catheter more easily to the long axis of the nerve. This approach is not possible in the supine position as the needle tip is poorly seen or not visualized.
In the prone position, the leg to be blocked is raised so as to flex the knee. The probe is placed in the transverse position. In general the needle is introduced out-of-plane at 70 degrees to the skin.
The volume of LA usually injected is between 0.1–0.3 ml/kg of ropivacaine 0.2% or levobupivacaine 0.25% for prolonged blockade. Mepivacaine can be used for shorter neural blockade. For continuous sciatic nerve block, an infusion of 0.1 ml/kg/h of 0.1% or 0.2% ropivacaine (in infants or children respectively) is usually administered for 48–72 hours.
Related posts:
 Ultrasound-guided supraclavicular brachial plexus block
Ultrasound-guided supraclavicular brachial plexus block
 Ultrasound-guided ilioinguinal/iliohypogastric block
Ultrasound-guided ilioinguinal/iliohypogastric block
 Ultrasound-guided transversus abdominis plane block
Ultrasound-guided transversus abdominis plane block
 Ultrasound-guided rectus sheath block
Ultrasound-guided rectus sheath block
 Ultrasound for spinal anesthesia
Ultrasound for spinal anesthesia
 Anatomy of the neuraxis, thoracic and abdominal walls, upper and lower limbs
Anatomy of the neuraxis, thoracic and abdominal walls, upper and lower limbs
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


