Sonoanatomy for a rectus sheath block.
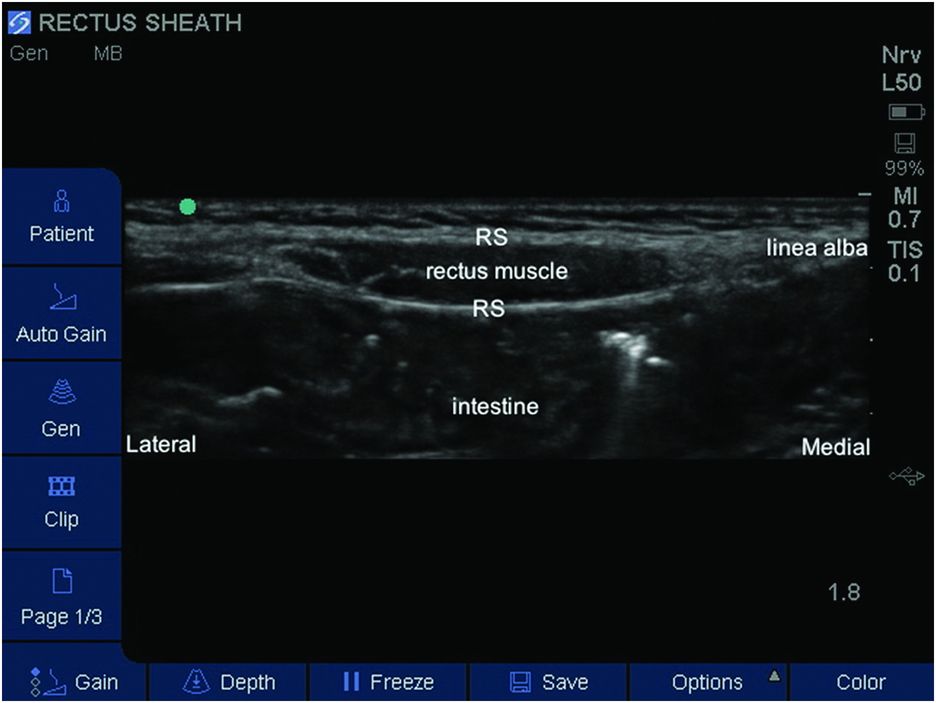
Labeled sonoanatomy for a rectus sheath (RS) block.
Landmarks
The child is placed supine and the outline of the rectus muscle sheath is determined by palpation or ultrasound imaging. The rectus muscles are usually easy to palpate along their length in small children. The probe is placed at the appropriate level, bearing in mind that a number of injections may be required depending on the extent of surgery (Figure 16.3). Bilateral blocks are required for any midline surgeries.

Patient position and probe placement for umbilical surgery.
Block performance
In children a high-frequency low penetrance probe may be sufficient for visualization of the rectus muscle and sheath in the anterior abdominal wall. The depth of the rectus muscle can be variable depending on the amount of subcutaneous tissue. The ultrasound probe can be scanned laterally to identify the junction of the external oblique, internal oblique, and transverus abdominis muscles with the rectus abdominis muscle. The epigastric vessels should also be identified.
The needle is inserted in-plane in a lateral to medial direction and advanced through the anterior rectus sheath and the rectus abdominis muscle. The needle is advanced until the tip is through the muscle and lying on the posterior rectus sheath (Figure 16.4). A small amount of LA or saline can be used to confirm that the location of the needle tip is not intramuscular prior to injection of the appropriate dose of LA.
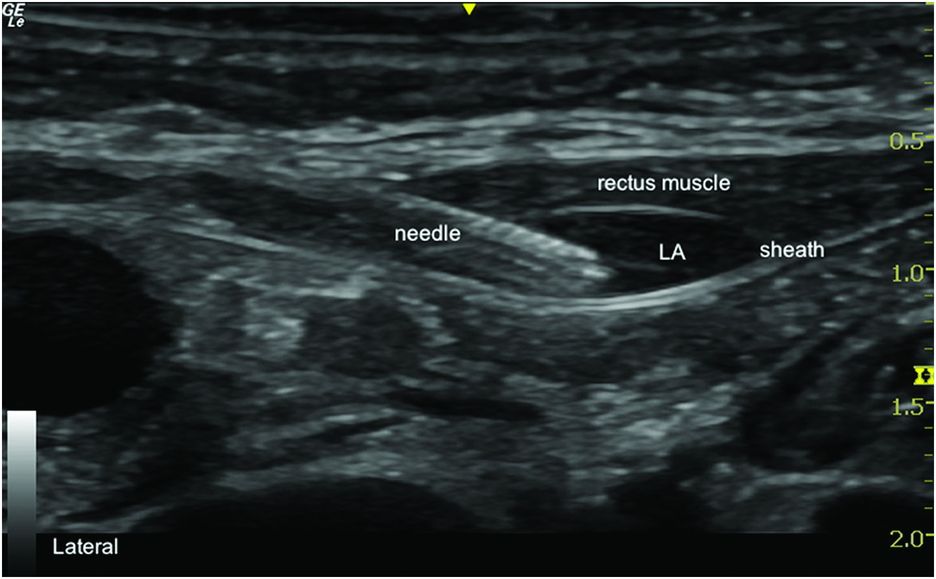
Needle in rectus sheath and local anesthetic (LA) deposition below rectus muscle.
For single injection a 22-gauge 50 mm short-bevel needle can be used, and the length of needle can be elected based on child size and depth of the rectus sheath.
A volume of 0.1 ml/kg of 0.25% bupivacaine or 0.2% ropivacaine is recommended for a rectus sheath block (Flack et al., 2014).
The same procedure should be repeated on the opposite side. An out-of-plane technique may also be used to perform a rectus sheath block.
Continuous catheter technique
The patient position and probe orientation are similar to that of a single injection technique. Once the needle tip is positioned between the rectus abdominis muscle and the posterior rectus sheath, 1–2 ml of normal saline can be injected to confirm the tip location. This will also ease the advancement of the catheter into the space between the rectus abdominis muscle and the posterior rectus sheath. Once the catheter is inserted, the catheter tip position is confirmed by visualizing an injection of a small amount of LA through the catheter. Following this confirmation, the intended dose of LA is administered through the catheter.
Related posts:
 Ultrasound-guided supraclavicular brachial plexus block
Ultrasound-guided supraclavicular brachial plexus block
 Ultrasound-guided ilioinguinal/iliohypogastric block
Ultrasound-guided ilioinguinal/iliohypogastric block
 Ultrasound-guided transversus abdominis plane block
Ultrasound-guided transversus abdominis plane block
 Ultrasound-guided sciatic nerve block
Ultrasound-guided sciatic nerve block
 Ultrasound for spinal anesthesia
Ultrasound for spinal anesthesia
 Anatomy of the neuraxis, thoracic and abdominal walls, upper and lower limbs
Anatomy of the neuraxis, thoracic and abdominal walls, upper and lower limbs
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


