Sonoanatomy of the saphenous nerve in adductor canal.
The canal is bounded anteriorly by the sartorius muscle, antero-laterally by the vastus medialis and postero-medially by the adductor muscles (Figure 12.2). The canal contains the femoral artery and vein, the descending genicular and muscular branches of the femoral artery, the saphenous nerve, and the nerve to vastus medialis.
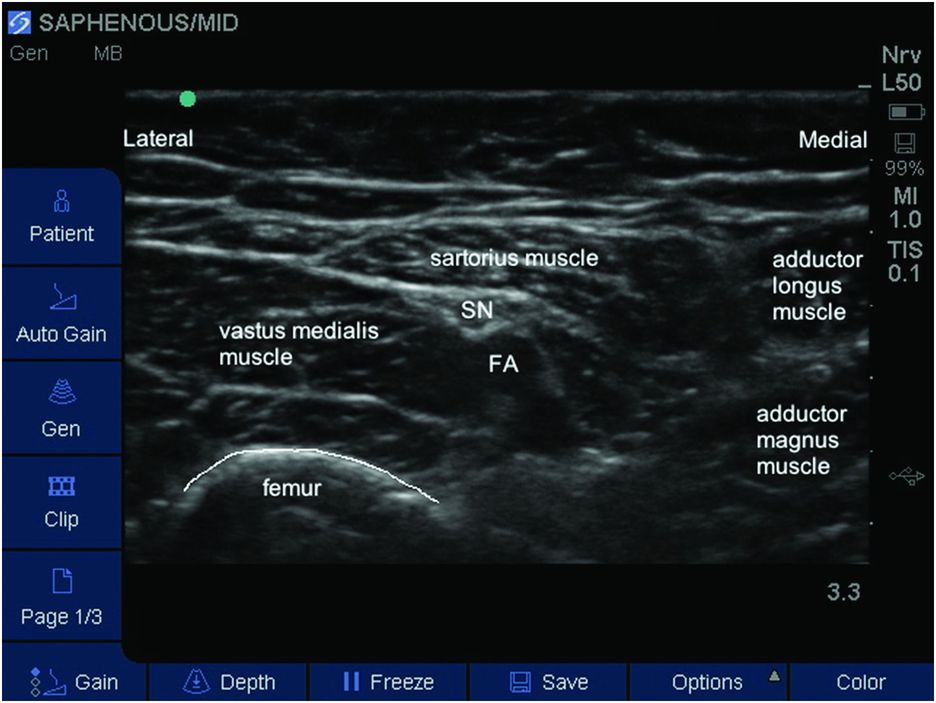
Labeled sonoanatomy of the saphenous nerve in adductor canal. FA, femoral artery; SN, saphenous nerve.
The saphenous nerve can be identified adjacent to the artery. It may be difficult to visualize as it is very small. It is usually hyperechoic and typically creates a small indentation in the posterior aspect of the sartorius muscle.
After the saphenous nerve leaves the adductor canal, it divides into the infrapatellar branch, which provides a sensory branch to the peripatellar plexus of the knee, and the sartorial branch, which perforates the superficial fascia between the gracilis and sartorius muscles, and emerges to lie in the subcutaneous tissue below the knee fold. It then descends along the medial tibial border with the long saphenous vein, giving multiple branches to the medial aspect of the leg, ankle, and forefoot. Ultrasound-guided infrapatellar nerve block can be performed, however, even with small volumes the saphenous nerve is blocked over 90% of the time.
Landmarks
Although ultrasound guidance allows visualization of the saphenous nerve throughout its course, three common sites are used:
1. Adductor canal
2. Just above the knee
3. Mid leg or above the ankle.
The child is placed supine.
To perform the adductor canal block, the ipsilateral hip is externally rotated with slight flexion of the knee. The probe is placed parallel to the inguinal ligament in the mid thigh region (Figure 12.3). For the mid leg or above the ankle approach, the child is positioned supine with the lower limb in neutral position.

Patient position and probe placement for the adductor canal approach.
Block performance
A high frequency linear probe is used for all three blocks.
Adductor canal block
The femoral artery is identified. One may continue scanning towards the knee following the femoral artery until the mid thigh where the femoral artery is usually found deep to the characteristically elliptical sartorius muscle.
Continue to scan caudally following the artery and nerve until the point of separation of the artery and nerve in order to avoid any accidental arterial puncture. The vastus medialis muscle will be anterolateral, the sartorius muscle will be medial and the adductor magnus muscle will lie posteromedial.
An in-plane approach is the commonest approach to allow visualization of the needle and its advancement (Figure 12.4). In younger children or neonates an out-of-plane approach may be needed to allow the shortest distance for needle advancement.
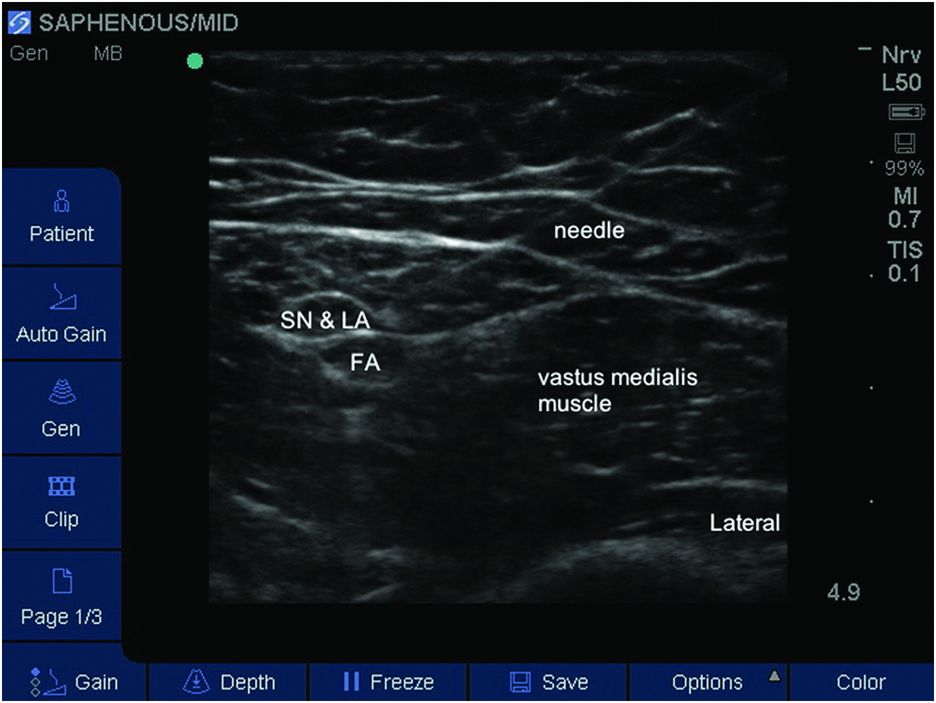
Needle insertion and local anesthetic (LA) injection. FA, femoral artery; SN, saphenous nerve.
A 50-mm block needle may be used, and sufficient local anesthetic (LA) injected into the canal to surround the nerve. There are no data on the optimal dosing regime in children. A clinically effective volume is 0.2 ml/kg of bupivacaine 0.25% with epinephrine (1:200 000).
Just above the knee
This approach is mainly indicated for surgery of the medial aspect of the leg as an alternative to the mid-thigh approach. It has a lower risk of motor block, as the nerve to vastus medialis should have already separated. The probe is placed a few centimeters or 2–3 patient’s own fingerbreadths above the patella on the anterior aspect. Following identification of the vastus medialis muscle, the probe is moved medially until the vastus medialis edge and the sartorius muscle is identified with its characteristic elliptical shape. By scanning the sartorius muscle a few centimeters cranially and caudally, the nerve can be identified as a small hyperechoic structure. This approach has the advantage of a lower incidence of arterial puncture.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


