Fig. 10.1
Sensory supply to the face. (1) Trigeminal ganglion, (2) ophthalmic nerve, (3) maxillary nerve, (4) mandibular nerve, and (5) auriculotemporal nerve (With permission from Danilo Jankovic)
Ophthalmic Nerve (Figs. 10.1 and 10.2)
Fig. 10.2
Trigeminal nerve. (1) Trigeminal (Gasserian, semilunar) ganglion, (2) mandibular nerve in the oval foramen, (3) mandibular nerve and otic ganglion (red point), (4) ophthalmic nerve, (5) frontal nerve, (6) maxillary nerve and pterygopalatine ganglion, (7) infraorbital nerve,(8) auriculotemporal nerve,(9) buccal nerve, (10) lingual nerve, (11) alveolar inferior nerve, (12) mental nerve, (13) dura mater (With permission from Danilo Jankovic)
The optic branch is purely sensory and passes lateral to the cavernous sinus and abducent nerve to the superior orbital fissure. It draws sympathetic fibers from the internal carotid plexus and in turn gives off sensory fibers to the oculomotor nerve, trochlear nerve, and abducent nerve. Before entering the fissure, the ophthalmic nerve branches into the lacrimal nerve, nasociliary nerve, and frontal nerve.
The frontal nerve runs along the levator palpebrae superioris muscle to behind the center of the orbital cavity. There it divides into the supraorbital nerve, which passes to the supraorbital notch, and the supratrochlear nerve, which runs in a medial direction toward the trochlea. The branches of the supratrochlear nerve supply the upper eyelid, the root of the nose, and the adjoining skin of the forehead (upper end branch), as well as the skin and conjunctiva of the medial canthus (lower end branch).
Maxillary Nerve (Figs. 10.1 and 10.2)
The second branch of the trigeminal nerve is also purely sensory. It emerges from the skull through the round foramen and enters the pterygopalatine fossa.
From here, it gives off the zygomatic nerve to the orbit and the pterygopalatine nerves—two very short nerves that connect with the pterygopalatine (sphenopalatine) ganglion (Fig. 10.12). As a continuation of its trunk, the infraorbital nerve penetrates through the inferior orbital fissure to the base of the orbit, to the infraorbital groove and infraorbital canal. After passing through the infraorbital foramen, it reaches the facial surface of the maxilla. Here it divides into three groups of branches, which supply the side of the nose, the lower eyelid, and the upper lip.
Mandibular Nerve (Figs. 10.1 and 10.2)
As the largest branch of the trigeminal nerve, the mandibular nerve contains the sensory parts of the trigeminal ganglion and takes up the motor root of the trigeminal nerve. After passing through the oval foramen, the mandibular nerve forms a short, thick nerve trunk, on the medial side of which lies the otic ganglion. In its later course, the mandibular nerve divides into an anterior trunk with mainly motor fibers and a posterior trunk with nerve branches and end fibers mainly consisting of sensory fibers. The most important nerves and areas of supply in the posterior trunk are:
Mental nerve (skin and mucosa of the lower lip and chin)
Inferior alveolar nerve (molar and premolar teeth of the mandible)
Lingual nerve (floor of the mouth, mucosa of the anterior two thirds of the tongue)
Auriculotemporal nerve (ear, skin, and fascia of the temple)
The sensory branch of the anterior trunk, the buccal nerve, supplies the skin and mucosa in the area of the buccinator muscle.
Peripheral Branches of the Trigeminal Nerve [2, 4, 7, 9–11, 13]
The supraorbital foramen, infraorbital foramen, and mental foramen lie on a single line running about 2.5 cm lateral to the midfacial line and passing through the pupil (Fig. 10.3).
Fig. 10.3
The supraorbital foramen (1), infraorbital foramen (2), and mental foramen (3) lie on a single line running about 2.5 cm lateral to the midfacial line and passing through the pupil (With permission from Danilo Jankovic)
Block of Ophthalmic Nerve Branches, Supraorbital and Supratrochlear Nerves
The end branches of these two nerves provide the sensory supply for the skin of the forehead, the top of the nose, and the skin and conjunctiva of the medial canthus (Figs. 10.4 and 10.30).
Fig. 10.4
(1) Supraorbital and supratrochlear nerves, (2) infraorbital nerve, (3) mental nerve (With permission from Danilo Jankovic)
Indications
Diagnostic
Differential diagnosis of hyperalgesic zones, e.g., the frontal part of the occipitofrontalis muscle
Therapeutic
Trigeminal neuralgia of the first branch and postherpetic neuralgia
Postoperative and post-traumatic pain
Minor surgical interventions (note higher doses) along the surface of the innervated area, e.g., removal of cysts and atheromas, wound care
Specific Contraindications
None.
Procedure
Preparations
Check that the emergency equipment is complete and in working order. Sterile precautions.
Materials
2-mL syringes, fine 26-G needles (25 mm), disinfectant, and swabs for compression.
Skin Prep
For all blocks.
Patient Positioning
Supine.
Landmarks
Supraorbital foramen and upper angle of the orbit.
Supraorbital nerve: palpation of the supraorbital foramen at the orbital margin.
Supratrochlear nerve: palpation of the upper angle of the orbit on the medial side of the root of the nose.
Injection Techniques
Supraorbital Nerve
After palpation of the supraorbital foramen, a swab is laid on the eyelid to prevent uncontrolled spread of the local anesthetic. The needle is introduced as far as the supraorbital foramen (bone contact), slightly withdrawn, and after aspiration the injection is carried out slowly (Figs. 10.3 and 10.5).

Fig. 10.5
Anesthetizing the supraorbital nerve (With permission from Danilo Jankovic)
Supratrochlear Nerve
After palpation of the upper angle of the orbit, a swab is laid on the eyelid to prevent uncontrolled spread of the local anesthetic. The needle is introduced at the upper internal angle of the orbit (Fig. 10.6) and minimally withdrawn after bone contact. Slow injection of the local anesthetic follows after careful aspiration.
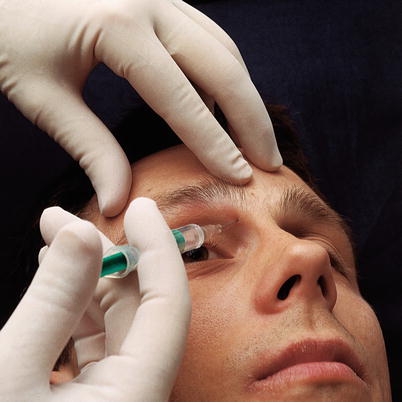
Fig. 10.6
Anesthetizing the supratrochlear nerve (With permission from Danilo Jankovic)
It is not necessary to elicit paresthesias. Look for bone contact, withdraw the needle slightly, aspirate, and inject.
Dosage
Diagnostic
0.5–1 mL local anesthetic, e.g., 0.5–1 % prilocaine, mepivacaine, and lidocaine.
Therapeutic
0.5–1 mL local anesthetic, e.g., 0.5–0.75 % ropivacaine and 0.25–0.5 % bupivacaine.
Surgical
Up to 5 mL local anesthetic.
Shorter procedures: e.g., 1 % prilocaine or 1 % mepivacaine.
Longer procedures: 0.75 % ropivacaine or 0.5 % bupivacaine (0.5 % levobupivacaine).
Side Effects
Possible hematoma formation (prophylactic compression).
After the injection, carry out thorough compression (massaging in) to prevent hematoma formation and to encourage the local anesthetic to spread.
Complications
Risk of blood vessel and nerve damage with injections into the foramina and bone channels.
No injections should be made into the supraorbital foramen due to the risk of nerve injury.
Block of Branches of Maxillary Nerve, Block of the Infraorbital Nerve
The infraorbital nerve, the end branch of the maxillary nerve, emerges about 1 cm below the middle of the lower orbital margin through the infraorbital foramen (Figs. 10.3, 10.4, and 10.32).
Indications
Diagnostic
Differential diagnosis of trigger zones
Therapeutic
Trigeminal neuralgia in the second branch and postherpetic pain
Facial pain in the innervation area of the infraorbital nerve, post-traumatic pain, and pain after dental extraction
Minor surgical procedures on the surface of the area of distribution (note higher dosages)
Specific Contraindications
None.
Procedure
Preparation and Materials (See Supraorbital Block)
Skin Prep
For all blocks.
Patient Positioning
Supine.
Landmarks
Extraoral Injection
Palpation of the infraorbital foramen, about 1 cm below the middle of the lower orbital margin.
Intraoral Injection
Palpation of the lower orbital margin.
Injection Techniques
Extraoral Injection
After palpating the infraorbital foramen, the needle is introduced cranially just below the palpation point until bone contact is made (Fig. 10.7) and then withdrawn slightly.

Fig. 10.7
Extraoral technique for blocking the infraorbital nerve (With permission from Danilo Jankovic)
Intraoral Injection
The center of the lower orbital margin is palpated and marked with the middle finger. The upper lip is raised with a spatula or with the thumb and index finger. The needle is introduced above the second premolar tooth toward the infraorbital foramen, until bone contact is made, and then withdrawn slightly (Fig. 10.8).
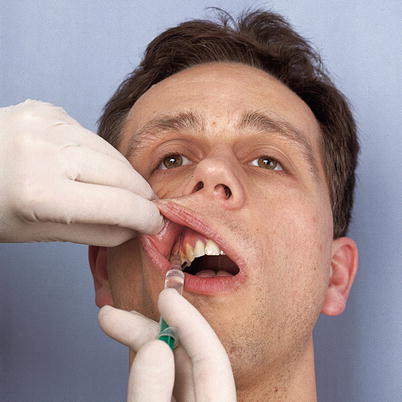
Fig. 10.8
Intraoral technique for blocking the infraorbital nerve (With permission from Danilo Jankovic)
For both of these techniques, it is important that slow injection of the local anesthetic should only be carried out after careful aspiration. Afterward, thorough compression should be carried out to prevent hematoma formation and to obtain better distribution of the local anesthetic.
No injections should be made into the infraorbital canal due to the risk of nerve injury.
Dosages
Diagnostic
0.5–1 mL local anesthetic, e.g., 0.5–1 % prilocaine, mepivacaine, and lidocaine.
Therapeutic (Extraoral Technique)
0.5–1 mL local anesthetic, e.g., 0.5–0.75 % ropivacaine and 0.5 % bupivacaine (0.5 % levobupivacaine).
Surgical
Up to 5 mL local anesthetic extraorally.
Shorter procedures: 1 % prilocaine or 1 % mepivacaine. Longer procedures: 0.75 % ropivacaine or 0.5 % bupivacaine (0.5 % levobupivacaine).
Intraorally: 2–3 mL local anesthetic.
Side Effects
Potential hematoma formation (prophylactic compression).
If the needle is advanced too far, penetration of the orbit can occur.
Symptom: temporary double vision.
Complications
Injection into the bone canal carries a risk of nerve damage.
Block of Branches of the Mandibular Nerve, Block of the Mental Nerve
The mental nerve, the sensory end branch of the mandibular nerve, emerges from the mental foramen at the level of the second premolar (Figs. 10.3 and 10.9).

Fig. 10.9
Extraoral technique for blocking the mental nerve (With permission from Danilo Jankovic)
It provides the sensory supply of the skin and mucosa of the lower lip and chin (Fig. 10.33).
Indications
Diagnostic
Differential diagnosis of trigger points and hyperalgesic zones
Therapeutic
Trigeminal neuralgia of the third branch
Post-traumatic pain and pain in the innervation area of the mental nerve
Dental treatment of the canine tooth and first premolars and incisors of the lower jaw
Postdental extraction pain (intraoral technique)
Surgical procedures on the surface of the lower lip (note higher dosages)
Specific Contraindications
None.
Procedure
Preparation and Materials (See Supraorbital Nerve Block)
Skin Prep
In all blocks.
Patient Positioning
Supine.
Landmarks
Extraoral and intraoral injection
Palpation of the mental foramen at the level of the second premolar.
Injection Techniques
Extraoral Injection
After palpation of the mental foramen, the needle is inserted about 2.5 cm lateral to the midline until bone contact is made (Fig. 10.9).
Intraoral Injection
After palpation of the mental foramen, the lower lip is pressed downward using a spatula. The needle is inserted between the first and second premolars, into the lower reflection of the oral vestibule, in the direction of the neurovascular bundle (Fig. 10.10).

Fig. 10.10
Intraoral technique for blocking the mental nerve (With permission from Danilo Jankovic)
For both of these techniques, it is important that slow injection should only be carried out after careful aspiration. Afterward, thorough compression should be carried out to prevent hematoma formation and to obtain better distribution of the local anesthetic.
Dosage
Diagnostic
0.5–1 mL local anesthetic, e.g., 0.5–1 % prilocaine, mepivacaine, and lidocaine.
Therapeutic (Extraoral Technique)
0.5–1 mL local anesthetic, e.g., 0.5–0.75 % ropivacaine and 0.5 % bupivacaine (0.5 % levobupivacaine).
Surgical
Up to 5 mL local anesthetic extraorally.
Shorter procedures: 1 % prilocaine or 1 % mepivacaine.
Longer procedures: 0.75 % ropivacaine or 0.5 % bupivacaine (0.5 % levobupivacaine).
Intraorally: 2–3 mL local anesthetic.
Side Effects
Potential hematoma formation (prophylactic compression).
Complications
Injection into the bone canal carries a risk of nerve damage.
Injections should never be made into the mental canal, due to the risk of nerve injury.
Ultrasound Imaging for Peripheral Branches of the Trigeminal Nerve
Ban C. H. Tsui
Ultrasound imaging is a common, noninvasive modality to facilitate many regional nerve blocks and to visualize nerves and surrounding soft tissue. However, there is limited available literature describing the use of ultrasound for superficial and deep trigeminal nerve block. This is because the most comprehensive deep trigeminal nerve blocks target the central ganglion. Because the ganglion is deep, blockade is often performed under fluoroscopic guidance or computerized tomography.
While blockade of deep structures is inaccessible to ultrasound, superficial branches of the trigeminal nerve (i.e., supraorbital, infraorbital, and mental nerves) are too small to visualize with most common ultrasound machines. In fact, the superficial branches can be performed easily by palpating their respective foramina. Although these bony foramina are usually easy to palpate physically, they can also be identified by observing a disruption or discontinuity within the bony hyperechoic line when imaging with ultrasound [22], as described below. Due to the superficial nature of these blocks, most experts find it more practical to use ultrasound imaging for landmarking the foramina rather than for real-time guidance.
Scanning Technique
1.
As described in the previous section, all three foramina are typically located approximately 2.5 cm lateral to the midfacial line passing through the pupil in the sagittal plane on each side of the face.
2.
Get Clinical Tree app for offline access

Using a high-frequency linear transducer, the foramina can be identified dynamically by subtle movement of the probe position after placing it in the usual vicinity of the foramina; this technique will allow the user to capture breaks in the linear hyperechogenicity of the bony surface caused by the foramina:
(a)




To locate the supraorbital landmark, the probe is positioned transversely above the roof of the orbital rim and in alignment with the pupil. The bone is scanned slowly in a cephalad-to-caudad direction to identify the supraorbital foramen.
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree