Fig. 27.1
Transverse section at the level of the T2-T3. Rotator cuff muscles and neighboring muscles. (1) Supraspinatus muscle, (2) infraspinatus muscle, (3) subscapularis muscle, (4, 5) scapula, (6) deltoid muscle, (7) greater tubercle of the humerus, (8) spinal cord (Reproduced with permission from Danilo Jankovic)
Fig. 27.2
Anatomy (anterior view): (1) cords of the brachial plexus, (2) subscapular nerve, (3) thoracodorsal nerve, (4) subscapular muscle, (5) circumflex scapular artery (Reproduced with permission from Danilo Jankovic)
Fig. 27.3
Anatomy. Subscapular fossa and subscapular muscle (Reproduced with permission from Danilo Jankovic)
The subscapular nerves consist of two or three nerves emerging from various parts of the brachial plexus for the subscapular, teres major, and latissimus dorsi muscles. The longest and most important of these is the thoracodorsal nerve, which runs along the axillary border of the scapula and supplies the latissimus dorsi muscle.
The superior subscapular nerve emerges from C5 and C6 (C7) and enters the subscapular muscle. The medial subscapular nerve (C5–6) arises from the posterior secondary trunks and supplies the lateral lower part of the subscapular muscle and teres major muscle.
The inferior subscapular nerve (thoracodorsal nerve) is the largest in this group. It arises from the posterior secondary branches or from the axillary nerve, or more rarely from the radial nerve, and passes along the lateral edge of the scapula to the latissimus dorsi muscle.
Innervation and Function
Table 27.1.
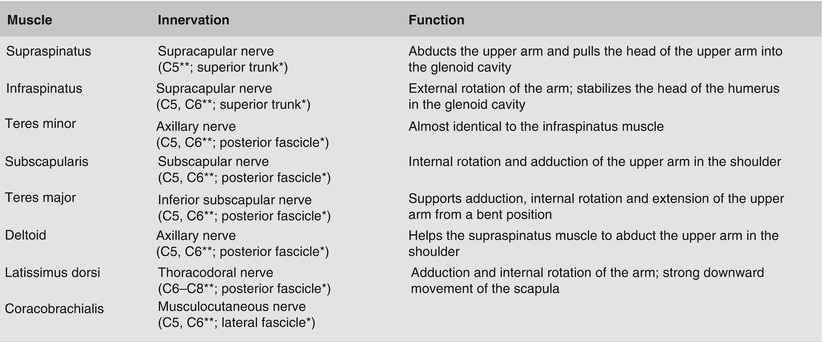
Table 27.1
Rotator cuff muscle (dark blue) and neighboring muscles: innervation and function
Indications
Indications for a subscapular nerve block and subscapularis trigger point infiltration are presented in Table 27.2.
Table 27.2
Indications for subscapular nerve block and subscapularis trigger point
Infiltration |
|---|
Diagnostic: in painful conditions of the shoulder girdle/joint |
Therapeutic: in the following situations (in combination with physiotherapy): |
Frozen shoulder syndrome |
Rheuma |
Diabetes |
Post-trauma neuralgia |
Postherpetic neuralgia |
Post-hemiplegia neuralgia |
Ankylosing spondylitis |
Procedure
Preparations
Check that the emergency equipment is complete and in working order; sterile precautions, intravenous access. Prior information for the patient is an absolute necessity.
Materials
Fine 25-mm-long 26-G needle for local anesthesia, 70-mm-long 20-G needle (with the needle shaft angled by about 20°), local anesthetic, disinfectant, swabs, 2- and 10-mL syringes.
Position
Sitting, with the neck comfortably tilted and the shoulders relaxed.
Location (Fig. 27.4)

Fig. 27.4
Location. Marking the injection site (center of the medial border of the scapula) (Reproduced with permission from Danilo Jankovic)
1.
The patient’s arm is pulled back, so that the contours of the scapula are easily recognized. The center of the medial border of the scapula is marked as the injection point.
2.
Acromion
Skin prep, local anesthesia, drawing up the local anesthetic, and testing the injection needle for patency.
1.
Before the injection, the shaft of the injection needle should be bent by about 20°.
2.
Targeted paresthesias are not elicited.
3.
During the injection, observe the skin for possible subcutaneous spread of the local anesthetic.
Injection Technique
1.
Introduce the 20°-angled needle into the center of the medial border of the scapula, in the direction of the acromion (Figs. 27.5 and 27.6a, b).

Fig. 27.5
Introducing the needle in the direction of the acromion (Reproduced with permission from Danilo Jankovic)
Fig. 27.6
(a) Introducing the needle in the direction of the acromion (skeletal model) (Reproduced with permission from Danilo Jankovic). (b) (1) Inferior angle of the scapula, (2) medial border of the scapula with subscapularis muscle inside, (3) rhomboideus major muscle, (4) infraspinatus muscle, (5) trapezius muscle (Reproduced with permission from Danilo Jankovic)
2.
The needle is introduced subscapularly parallel to the skin surface between the anterior surface of the scapula (costal surface) and the posterior thoracic wall (ribs), into the subscapular fossa. If the needle meets the edge of the ribs, it is withdrawn as far as the subcutaneous tissue and reintroduced.
The signs of a successful injection are spread extending into the shoulder joint, upper arm, and often as far as the wrist, corresponding to the radiation pattern of the trigger points of the subscapular muscle [2] (Fig. 27.7a, b).
Fig. 27.7
Magnetic resonance images 10 min after injection of 10 mL ropivacaine, without radiographic contrast medium, into the subscapular fossa. (a) Axial (cross section). (b) Paracoronal. (1) Thorax wall, (2) subscapular muscle and subscapular fossa, (3) head of the humerus, (4) teres minor muscle, (5) deltoid muscle, (6) scapula, (7) infraspinatus muscle (Reproduced with permission from Danilo Jankovic)
Dosage
Diagnostic
Five millilitres local anesthetic—e.g., 1 % prilocaine or 1 % mepivacaine.
Therapeutic
Ten to fifteen millilitres local anesthetic– e.g., 0.5–0.75 % ropivacaine, 0.25–0.5 % bupivacaine (0.25–0.5 % levobupivacaine). In acute pain, the addition of 40 mg triamcinolone has proved useful.
A combination of the subscapular and suprascapular nerve blocks is possible and often desirable (Table 27.3).
Table 27.3
Shoulder–arm region: blocking techniques in pain therapy
Indications | ||||
|---|---|---|---|---|
Surgical | Postoperative pain therapy | Acute and chronic pain conditions Target area | Mobilization of the shoulder | |
Shoulder | Shoulder–arm | |||
Interscalenea +++++ Dosage: 20–25 mL 0.75 % ropivacaine or 0.5 % bupivacaine (0.5 % levobupivacaine) | Interscaleneb +++++ 20–25 mL 0.375–0.5 % ropivacaine or 0.25 % bupivacaine (0.25 % levobupivacaine) | Subscapular nerves +++++ 10–15 mL 0.5–0.75 % ropivacaine or 0.25 % bupivacaine (0.25 % levobupivacaine) | Interscalene +++++ 10–15 mL 0.375–0.5 % ropivacaine or 0.25 % bupivacaine (0.25 % levobupivacaine) | Interscalene +++++ 20–25 mL 0.375–0.5 % ropivacaine or 0.25 % bupivacaine (0.25 % levobupivacaine) |
Subscapular nervesb
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

| ||||





