Fig. 40.1
(a–c) Spine. (a) Lateral, (b) ventral, (c) dorsal (Reproduced with permission from Danilo Jankovic)
According to research findings, the mean length of the spinal column, from the foramen magnum to the tip of the coccyx, is 73.6 cm (range 67.4–78.8 cm), while in women, it is 7–10 cm shorter [9].
All of the vertebrae have the same basic shape, which is subject to certain variations in the individual sections of the spine. The basic shape consists of an anterior body (the body of the vertebra) and a dorsal arch (the vertebral arch), which consists of pedicles and laminae (Fig. 40.2).
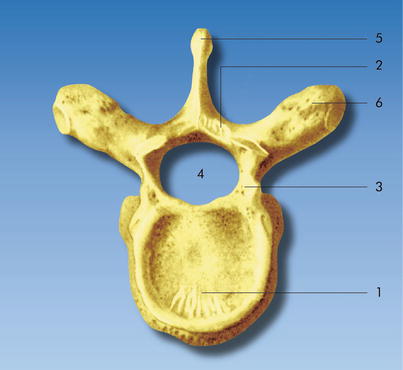
Fig. 40.2
Basic shape of a vertebra. (1) Vertebral body, (2) vertebral arch, (3) pedicle of the vertebral arch, (4) vertebral foramen, (5) spinous process, (6) transverse process (Reproduced with permission from Danilo Jankovic)
The laminae of the vertebral arch join dorsally to form the spinous process. A transverse process branches off on each side of the vertebral arch, as well as a superior and an inferior articular process. The vertebrae in the cervical region are smaller, but their size increases from cranial to caudal. The angle of inclination of the spinous processes—important topographic signposts for neuraxial injections—varies at different levels of the spine.
The cervical spinous processes, the first two thoracic spinous processes, and the lumbar spinous processes lie at the same level as their vertebrae. From T3 to L1, the spinous processes are angled caudally (particularly in the T4–T9 area) (Fig. 40.3a–c).
Fig. 40.3
(a–c) Cervical, thoracic, and lumbar spinous processes. (a) C7 cervical vertebra (vertebra prominens, nuchal tubercle). (b) T8 thoracic vertebra. (c) L3 lumbar vertebra (Reproduced with permission from Danilo Jankovic)
The vertebral canal (which provides excellent protection for the spinal cord) and the spinal cord, with its meningeal covering, extend throughout the whole length of the spine terminating in the cauda equina. The spinal vessels and nerves emerge laterally through openings at the upper and lower margins of the roots of the arches of the adjoining vertebrae (the intervertebral foramina).
Sacrum
The sacrum is wedge shaped and consists of five vertebrae fused together. It lies distal to the fifth lumbar vertebra and is connected distally, at its apex, to the coccyx. Dorsally, the sacrum has a convex surface, in the middle of which the median sacral crest stands out (Fig. 40.4a).
Fig. 40.4
(a) Sacrum (dorsal view). (1) Median sacral crest, (2) sacral horn, (3) sacral hiatus, (4) sacral canal, (5) posterior sacral foramina (Reproduced with permission from Danilo Jankovic). (b) Sacrum (ventral view). (1) Transverse lines, (2) anterior pelvic sacral foramina (With permission from Danilo Jankovic)
The crest is produced by the fusion of the rudimentary spinous processes of the upper third or fourth sacral vertebrae. Normally, the arch of the fifth and occasionally also of the fourth sacral vertebra is absent, so that there is a sacral hiatus at this point. The hiatus is bounded by the sacral horn as a remnant of the caudal articular process, and it is used as a passage by the five small sacral nerves and by the coccygeal nerves. Between the median sacral crest and the lateral sacral crest lie the four sacral openings (the posterior sacral foramina), through which the dorsal branches of the sacral spinal nerves emerge. The anterior view shows a concave aspect. Alongside the transverse lines (fused vertebrae), there are large anterior openings (the anterior pelvic sacral foramina), through which the primary anterior parts of the sacral nerves emerge (Fig. 40.4b).
Spinal Ligaments
The vertebrae are supported from the axis to the cranial sacrum by intervertebral disks and by various ligaments (Fig. 40.5a, b). The intervertebral disks lie between neighboring vertebrae and function as fixed connecting elements and pressure-absorbing buffers. The disks are at their thinnest in the area of T3–T7 and thickest in the lumbar area.
Fig. 40.5
(a) Ligaments of the spinal cord. (1) Supraspinous ligament, (2) interspinous ligament, (3) ligamentum flavum, (4) posterior longitudinal ligament, (5) intervertebral disk, (6) anterior longitudinal ligament (with permission from Danilo Jankovic). (b) Ligaments of the spinal cord. (1) Intertransverse ligament, (2) supraspinous ligament, (3) transverse process (With permission from Danilo Jankovic)
The anterior longitudinal ligament (Figs. 40.6 and 40.7) is attached at the anterior edge of the vertebral bodies and intervertebral disks and is at its thickest in the thoracic area. The posterior longitudinal ligament (Figs. 40.6 and 40.7) is wider cranially than it is caudally, and it lies behind the vertebral bodies in the medullary canal. The supraspinous ligaments extend as far as the sacrum along the tips of the spinous processes, with which they are connected, and continue cranially in the nuchal ligament and caudally in the interspinous ligament. They become thicker from cranial to caudal. The interspinous ligaments connect the roots and tips of the spinous processes.
Fig. 40.6
Ligaments of the spinal cord. (1) Ligamentum flavum, (2) supraspinous ligament, (3) interspinous ligament, (4) posterior longitudinal ligament, (5) anterior longitudinal ligament (With permission from Danilo Jankovic)
Fig. 40.7
Transverse section through the thorax at the level of T9. (1) Ligamentum flavum, (2) posterior epidural space, (3) anterior epidural space, (4) spinal dura mater, (5) subarachnoid space and spinal cord, (6) posterior longitudinal ligament, (7) anterior longitudinal ligament, (8) zygapophyseal joint, (9) aorta, (10) sympathetic trunk ganglion (With permission from Danilo Jankovic)
The intertransverse ligaments serve to connect the transverse processes (Fig. 40.5b).
The ligamentum flavum largely consists of yellow, elastic fibers and it connects the neighboring laminae (Figs. 40.6 and 40.7). It is at its thinnest in the midline (small fissure spaces exist for the veins running from the internal vertebral venous plexus to the external vertebral venous plexus), and its thickness increases laterally. The size and shape of the ligamentum flavum vary at the various levels of the spine. Caudally, for example, it is thicker than in the cranial direction.
There are usually only 22 genuine ligamenta flava, as they do not develop between the atlas and occiput or between the atlas and the axis. The mean length of the ligamentum flavum is 0.84 cm in the cervical spine, 1.03 cm in the thoracic spine, and 1.61 cm in the lumbar spine. The mean width is 2.30 cm in the cervical region, 2.0 cm in the thoracic region, and 3.22 cm in the lumbar region. The ligamenta flava have a mean thickness of 1.37 mm in the cervical spine, 1.75 mm in the thoracic spine, and 2.55 mm in the lumbar spine. According to Yong-Hing et al. (1976), the human ligamentum flavum consists of 50–80 % elastin and 20–50 % collagen [9].
Iliolumbosacral Ligaments (Sacroiliac Joints)
The stability of the iliolumbosacral region is ensured by lumbosacral and sacroiliac connections that transfer the entire weight of the trunk via the hip bones to the lower extremities. These ligamentous connections serve to connect the vertebrae with one another and to stabilize the sacrum.
Clinically important ligaments: interspinous, supraspinous, iliolumbar, interosseous sacroiliac, sacrospinous, and sacrotuberous ligaments (Fig. 40.8a, b).
Fig. 40.8
(a) Iliolumbosacral ligaments (dorsal view). (1) Iliolumbar ligament, (2) dorsal sacroiliac ligament, (3) sacrotuberous ligament, (4) superficial dorsal and deep dorsal sacrococcygeal ligaments, (5) lateral sacrococcygeal ligament, (6) sacrospinous ligament (with permission from Danilo Jankovic). (b) Iliolumbosacral ligaments (ventral view). (1) Iliolumbar ligament, (2) ventral sacroiliac ligament, (3) sacrospinous ligament, (4) sacrotuberous ligament, (5) ventral sacrococcygeal ligament (With permission from Danilo Jankovic)
Spinal Cord
The mean length of the spinal cord from the foramen magnum downward is 45.9 cm in men and 41.5 cm in women [8, 9]. The conus medullaris continues in the threadlike median filum terminale as far as the posterior side of the coccyx (Figs. 40.7, 40.9a–c, and 40.13).
Fig. 40.9
(a) Spinal cord (lower half). (1) Conus medullaris, (2) cauda equina, (3) filum of spinal dura mater (filum terminale), (4) sacral nerves, (5) lumbar nerves, (6) thoracic nerves, (7) dura mater (With permission from Danilo Jankovic). (b) Transverse section at the level of L4/5. (1) Posterior epidural space with fat, (2) anterior epidural space with veins, (3) spinal dura mater, (4) subarachnoid space and cauda equina, (5) zygapophyseal joint, (6) anterior longitudinal ligament, (7) posterior longitudinal ligament (With permission from Danilo Jankovic). (c) The cauda equina at the level of L2–5. Lateral view. (1) Spinal dura mater, (2), epidural space (With permission from Danilo Jankovic)
Rootlets: Cauda Equina [8, 9]
The cauda equina is generally regarded as consisting of the thick, horsetail-shaped fascicle of nerve fibers in the lower part of the dural sac, containing the paired rootlets of the lowest thoracic and entire lumbar and coccygeal medulla. All of the motor and sensory fibers of the lumbosacral plexus, pudendal nerve, and coccygeal nerve course inside the lumbosacral subarachnoid space. A constant increase in the thickness of the root fascicle is seen between the L1 and L3 segments. The terminal filum of the spinal cord is approximately 153 mm long (range 123–178 mm) (Figs. 40.9b, 40.11, 40.13, and 40.14).
The dura mater and arachnoid, and consequently the subarachnoid space as well, extend downward as far as the level of the second sacral vertebra.
Meninges
The spinal cord is surrounded and protected by the meninges (the dura mater, arachnoid mater, and pia mater) and by cerebrospinal fluid, epidural fatty tissue, and veins (Figs. 40.10 and 40.11).
Fig. 40.10
Meninges. (1) Dura mater, (2) arachnoid mater, (3) pia mater, (4) spinal nerve, (5) dorsal (posterior) root, (6) ventral (anterior) root, (7) internal vertebral venous plexus (With permission from Danilo Jankovic)
Fig. 40.11
A lumbar vertebral canal opened from posterior in the area of L3 and L4. The cauda equina has been exposed by partial resection of the spinal dura mater and arachnoid mater. (1) Spinal dura mater, (2) arachnoid mater, (3) with posterior and anterior roots, (4) dorsal root, (5) spinal ganglion, (6) posterior and anterior spinal branches (With permission from Danilo Jankovic)
The meninges form a connected, unified organ with important protective functions for the brain and spinal cord; they provide mechanical, immunological, and thermal protection and are also important for metabolism in the CNS. The mechanical function of the meninges consists of providing fixation for the brain in the cranium and for the spinal cord in the vertebral canal, as well as in forming a highly adaptable fluid mantle that functions like a water bed. The fixation is provided by the dura mater.
Dura Mater of the Spinal Cord (Figs. 40.7, 40.10, 40.11, 40.12, 40.13, and 40.14)
Fig. 40.12
Thoracic region of the spine. (1) Transverse process, (2) spinal dura mater (note the covering of the spinal ganglion), (3) spinal cord with vessels lying above it—the denticulate ligament is located to the left and right, and (4) the spinal dura mater has been removed—posterior longitudinal ligament, (5) thoracic spinous process; note the epidural space above (With permission from Danilo Jankovic)
Fig. 40.13
The spinal cord. (1) Spinal cord with vessels on it—the denticulate ligament is located to the right and left, (2) conus medullaris, (3) terminal filum with cauda equina, (4) sacrum (With permission from Danilo Jankovic)
Fig. 40.14
The spinal cord. Cervical, thoracic, and lumbar. Serial transverse sections at the levels of C6, T3, T9, T12, L3, and L4/5. Note the conus medullaris (T12) and cauda equina (L3, L4/5) (With permission from Danilo Jankovic)
The dura mater of the spinal cord, a fibroelastic membrane, extends as far as the second sacral vertebra, where it ends in a blind sac. It encloses the anterior and posterior spinal nerve roots.
It surrounds the anterior and posterior spinal nerve roots. It consists of collagenous fibers and a few elastic fibers; it is 0.1–0.5 mm thick and is usually thinner anteriorly than it is posteriorly. The dural sac is often enlarged in the area between L4 and S1 and also between T12 and L1 (Spischarny’s terminal cystoma). The thickness of the spinal dura mater declines from medial to lateral. The dura mater is often thinner ventrally than dorsally, and it sends off leaves and fibers into the epidural space. It shows notable foliation near the intervertebral foramina, where it passes on the one hand into the epineurium of the peripheral nerves and into the capsule of the spinal ganglia and on the other hand radiates into the cavernous body of the vascular plexus characterizing this area. One of the major characteristics of the dura mater is its extremely marked vascularization. Particularly in the boundary zone with the arachnoid, numerous capillaries and venules are fenestrated, promoting the exchange of various metabolites and cells between the blood and dura. The vascularization increases strongly in the lateral areas, particularly in the area of the dural infundibulum. The dural vessels are connected with the epidural vascular plexus and thus with the internal and external vertebral vein plexus as well. There are numerous nerve fibers in close proximity to the dural vessels [6, 12]. In terms of size, C fibers predominate. In terms of function, the dural nerves consist of sympathetic, parasympathetic, and sensory fibers. A whole range of neurotransmitters and neuropeptides have been identified in the dural nerves, such as acetylcholine, serotonin, substance P, calcitonin gene-related peptide (CGRP), neuropeptide Y, vasoactive intestinal polypeptide (VIP), etc. [3, 7]. In addition to vasoactive nerves, local factors also play a role in the regulation of dural perfusion, such as adenosine, which has been found abundantly in the dura [4]. Via a multilayered cell cluster known as the subdural nerve papilla (neurothele) [1, 5], the arachnoid membrane is directly connected with the innermost lamellae of the dura. A “subdural fissure”—often present in postmortem and only arising during life in specific circumstances—must be regarded as an artifact.
Between the dura mater and the arachnoid, there is a space, the subdural space, in which a small amount of lymph-like fluid is located.
The arachnoid mater (Figs. 40.10 and 40.11), a nonvascularized membrane, also ends at the level of the second sacral vertebra. Between the arachnoid mater and the pia mater lies the subarachnoid space, which is filled with cerebrospinal fluid (see the section “Cerebrospinal fluid”, below). The expansion forces present here reduce the weight of the brain “floating” in the cerebrospinal fluid to just under 50 g.
This protects the brain from harmful acceleration forces.
The same applies to the spinal cord. There is a substantial amount of exchange between the cranial and spinal cerebrospinal fluid. Magnetic resonance studies have confirmed Du Boulay’s older view that there are fluid waves synchronous with cardiac systole that move the cerebrospinal fluid from the basal cisterns into the cervical subarachnoid space [10]; respiration-synchronous fluid movements are superimposed on these [11]. The spinal subarachnoid space, with the extremely elastic spinal dura and adaptable arachnoid, makes it possible to absorb these rhythmic fluid waves (compliance). Artificial losses of cerebrospinal fluid undoubtedly have severe effects on the system’s natural mechanism and reduce the water-bed function of the exterior subarachnoid space. The subarachnoid space is important for the thermoregulation of the CNS, as it acts as a temperature buffer [13] both against excessive external temperatures and also against functional or pathological increases in temperature in the CNS. The normal basic temperature of the cerebrospinal fluid is approximately 37 °C. It is important to note that the cerebrospinal fluid does not represent “standing water” but is instead constantly in movement and continually being freshly produced, mainly in the choroid plexus. It is reabsorbed over a wide surface, not only via the arachnoid granulations or villi in the area of the nerve exit sites but also diffusely through the arachnoid into the dural vascular system and via the pia into the vessels of the pial vascular network [12]. The choroid plexus is not only a production organ but also a site for reabsorption of cerebrospinal fluid.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


