Hypertension
Judy Cheng PharmD, BCPS
Hypertension is one of the most common and most important risk factors in developing cardiovascular diseases such as coronary artery, cerebrovascular, and renal diseases. Prevention and proper control of hypertension can reduce the risk of developing such diseases. Since the inception of the National High Blood Pressure Education Program in 1972, remarkable progress has been made in detecting, treating, and controlling hypertension (Joint National Committee, 1997). Management of hypertension to date thus revolves around primary prevention via lifestyle modifications, early detection, and optimal treatment, with consideration of patients’ other concurrent medical problems. This chapter will discuss the primary prevention strategy for hypertension as well as the proper therapeutic management once the diagnosis is established. Issues related to the implementation and dissemination of these approaches will be emphasized.
ANATOMY, PHYSIOLOGY, AND PATHOLOGY
Anatomy and Physiology
Arterial blood pressure is defined hemodynamically as the product of the cardiac output and the total peripheral resistance. It reaches its peak during cardiac systole (SBP) and its nadir at the end of diastole (DBP). The cardiac output is the major determinant of SBP, and total peripheral resistance determines DBP. Cardiac output, in turn, depends on stroke volume, heart rate, and venous capacitance. Factors that increase stroke volume and heart rates will increase cardiac output and subsequently SBP. Alternatively, venous capacitance affects the volume of venous blood (preload) that is returned to the heart. Venous dilatation increases venous capacitance and decreases preload, thus decreasing SBP. Total peripheral resistance is regulated by contraction and dilation of the arterioles. Other factors that may also affect intravascular resistance include the elasticity of arteries and blood viscosity.
The difference between SBP and DBP (pulse pressure) is an indicator of the tone of the vessel walls. The mean arterial pressure, which is defined as one third of the pulse pressure plus DBP, is the average pressure throughout the cardiac cycle.
Blood pressure can be regulated by the kidneys, which control blood volume, and the sympathomimetic nervous system. Increased sympathomimetic activity stimulates vasoconstriction of arterioles, thus raising total peripheral resistance, and increases cardiac output, thus elevating blood pressure. For blood pressure to remain within normal limits, specialized receptors (baroreceptors) are used. These stretch receptors are located in the aortic arch and in the carotid sinuses. An increase in blood pressure causes these receptors to stretch and stimulate the activity of the sensory nerve. Sensory nerve activity from the baroreceptors is transmitted via the vagus and glossopharyngeal nerves to the medulla oblongata, which directs the autonomic system to respond appropriately. An effective baroreceptor reflex helps to maintain adequate blood flow to the brain on standing.
Pathophysiology
The vast majority of patients who have hypertension have essential (primary) hypertension. Secondary hypertension makes up only about 10% of the hypertensive population (Joint National Committee, 1997). Some possible causes of secondary hypertension include kidney disease, pheochromocytoma, primary aldosteronism, hyperthyroidism, or drug-induced hypertension (eg, cyclosporine, erythropoietin, sympathomimetic agents). Primary hypertension, on the other hand, may be caused by multiple factors, including abnormal neural mechanisms, defects in peripheral autoregulation, disturbances in sodium, calcium, and natriuretic hormone levels, and malfunctions in either humoral or vasodepressor mechanisms.
Abnormal Neural Mechanisms
The central and the autonomic nervous systems are intricately involved in the maintenance of arterial blood pressure. Located in the presynaptic and postsynaptic nervous endings are alpha and beta receptors. Stimulation of presynaptic alpha and beta receptors will lead to inhibition and enhancement, respectively, of norepinephrine release; stimulation of postsynaptic alpha-1 receptors leads to vasoconstriction. Stimulation of postsynaptic beta-2 receptors leads to vasodilation. Stimulation of beta-1 receptors in the heart enhances cardiac contractility and increases heart rate. The major negative feedback system of the sympathetic nervous system is the baroreceptor reflex. A pathologic disturbance in any of these neural components could lead to sustained elevations of blood pressure.
PERIPHERAL AUTOREGULATION
A defect in renal adaptive mechanisms can lead to plasma volume expansion and increased blood flow to peripheral tissues, even when blood pressure is normal. To offset such increases in blood flow, local tissue autoregulatory processes would induce arteriolar constriction to raise the peripheral vascular resistance.
DISTURBANCES IN SODIUM, CALCIUM, AND NATRIURETIC HORMONE
Increased sodium intake, together with an inherited defect in the kidney’s ability to excrete sodium, leads to an increase in the level of circulating natriuretic hormones. Natriuretic hormones
inhibit intracellular sodium transport, causing increased vascular reactivity and a rise in blood pressure.
inhibit intracellular sodium transport, causing increased vascular reactivity and a rise in blood pressure.
Calcium homeostasis also contributes to the pathogenesis of hypertension. Lack of calcium in the blood circulation leads to a relative elevation of calcium concentration intracellularly, which leads to altered vascular smooth muscle function and increased peripheral vascular resistance.
Potassium depletion may also cause an increase in peripheral vascular resistance, but its clinical impact is not clearly defined.
MALFUNCTION OF HUMORAL MECHANISM
The renin-angiotensin system’s involvement in hypertension has been well described. Renin is synthesized in the kidney and stored in the juxtaglomerular cells. Decreases in perfusion pressure to the kidney and the flux of sodium and chloride across the renal tubule trigger renin release. In blood, renin catalyzes the conversion of angiotensinogen to angiotensin I, which is then converted by angiotensin-converting enzymes (ACE) to angiotensin II. Angiotensin II is a direct vasoconstrictor. It also stimulates catecholamine and aldosterone release from the adrenal gland. This neurohormone will lead to hypertension. Angiotensin is also produced by local tissues of different organs, such as the heart and the brain. Local angiotensin may interact with other humoral regulators and endothelium-derived growth factors to stimulate vascular smooth muscle growth. Components of the local angiotensin system may be responsible for long-term adaptation to hypertension (eg, left ventricular hypertrophy, smooth muscle hypertrophy of blood vessels, and glomerular hypertrophy) (see Chap. 11).
Other neurohormonal mechanisms involved in hypertension include hyperinsulinemia and insulin resistance. Elevation in the serum insulin concentration may induce renal sodium retention and enhanced sympathetic nervous system activity and may cause vascular smooth muscle hypertrophy. The vascular endothelium also plays an important role in blood vessel tone. Vasoactive substances produced by the endothelium, such as prostacyclin, bradykinin, endothelium-derived relaxing factor, and endothelin I, interact with each other to maintain normal vessel tone. Imbalances of these vasoactive substances may contribute to hypertension.
EPIDEMIOLOGY
The Third National Health and Nutritional Examination Survey (NHANES III), which reviewed data collected from 1988 through 1994, indicated that approximately 50 million (or one in every four) adults in the United States have hypertension (Joint National Committee, 1997). Hypertension is associated with an increased risk of developing coronary artery disease, stroke, congestive heart failure, renal insufficiency, and peripheral vascular disease. There is no gender discrimination for such risk throughout the entire adult age range. However, the prevalence of hypertension increases progressively with increasing age. The risk of morbidity and mortality from cardiovascular disease increases in a curvilinear fashion with progressively higher levels of SBP and DBP. Research over the years has helped in identifying environmental, cultural, and social factors that may contribute to the current hypertension pattern.
Cultural Factors
Research in animals and humans has identified the following factors as the most important contributors to age-related increases in blood pressure (Joint National Committee, 1997):
High sodium intake (beyond human physiologic needs)
Overweight
Lack of physical activity
Excessive alcohol consumption
Smoking
Excessive stress
Inadequate potassium intake
Positive family history
Members of minority populations (eg, African Americans).
In a culture with a high level of stress, low physical activity, and excessive consumption of salt and alcohol, the prevalence of hypertension may increase.
Socioeconomic Factors
Socioeconomic status can also be a determinant of blood pressure. In economically developed countries, only a relatively small proportion of the general population has a blood pressure within the optimal range (<120/80 mmHg). This is, however, the norm in less developed societies, where age-related increases in blood pressure are uncommon (Carvalho et al, 1989; He et al, 1991). Reasons that may explain this phenomenon include differences in lifestyle (eg, activity level) and diet (eg, alcohol consumption) among different societies.
DIAGNOSTIC CRITERIA
Hypertension management begins with early detection. Primary care providers should measure a patient’s blood pressure at every clinic visit. Table 12-1 provides the Sixth Report of the Joint National Committee (JNC VI) classification of adult blood pressure based on the risk of developing cardiovascular events (Joint National Committee, 1997). All stages of hypertension are associated with an elevated risk of cardiovascular events and renal disease, but the higher the blood pressure, the greater the risk.
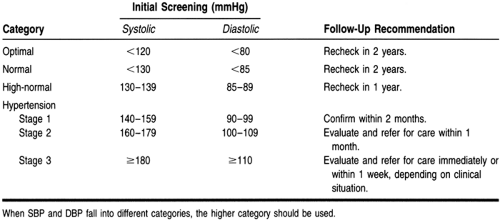 |
Hypertension should never be diagnosed based on a single measurement because various factors, such as coffee consumption and the medical white coat, may affect a patient’s blood pressure. An initial elevated reading should be confirmed on at least two subsequent visits over 1 to several weeks, except if SBP is above 180 mmHg, DBP is above 110 mmHg, or signs and symptoms of end organ damage are present. In these situations, patients need to be referred to emergency care immediately. An overall average SBP above 140 mmHg or a DBP above 90 mmHg will require further diagnosis and treatment. Table 12-1 illustrates the proper follow-up recommendations based on the initial screening blood pressure for patients older than age 18.
Because the risk of developing cardiovascular disease in patients with hypertension is determined not only by the level of blood pressure but also by the presence or absence of target organ damage or other risk factors (as listed below), the JNC VI guidelines recommend that treatment of hypertension be based on the patient’s risk group (Table 12-2).
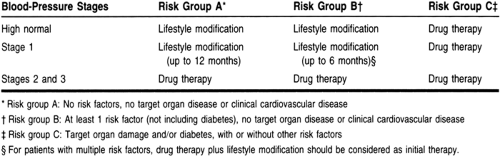 |
Risk factors for developing cardiovascular diseases (besides hypertension) are:
HISTORY AND PHYSICAL EXAMINATION
A complete medical history and physical examination should be performed in all hypertensive patients during their initial evaluation. This examination should include:
Family history of high blood pressure, premature coronary heart disease, stroke, cerebrovascular disease, diabetes, and hypercholesterolemia
Patient history or symptoms of cardiovascular, cerebrovascular, or renal disease, diabetes, hypercholesterolemia, or gout
Known duration and levels of elevated blood pressure
History of weight gain, stress, physical activity, and smoking
Dietary assessment, including sodium intake, alcohol use, and intake of cholesterol and saturated fat
Complete medication history, including the use of over-the-counter products as well as the results and side effects of previous antihypertensive agents
Symptoms suggesting secondary hypertension
Psychosocial and environmental factors that may influence blood-pressure control (eg, family and employment situations, educational level)
Verification of blood pressure by two or more blood-pressure measurements separated by 2 minutes with the patient either supine or seated and after standing for at least 2 minutes
Verification of blood pressure in the contralateral arm (if different, the higher value should be used)
Height, weight, and waist circumference
Funduscopic examination for arteriolar narrowing, arteriovenous nicking, hemorrhages, exudates, or papilledema
Examination of the neck for carotid bruits, distended veins, or an enlarged thyroid gland
Examination of the heart for tachycardia, hypertrophy, pericardial heave, clicks, murmurs, arrhythmias, and third or fourth heart sound
Abdominal examination for bruits, enlarged kidneys, masses, and abnormal aortic pulsation
Examination of extremities for diminished or absent peripheral arterial pulsations, bruits, and edemaRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








