28-year-old man who was shot in the hand. PA radiograph of the left small finger. There is a comminuted fracture of the small finger involving the PIP joint with small bullet fragments.
Case 17–2
Gunshot wound (hand)

19-year-old man who was shot in the hand. PA radiograph of the right hand. There is a comminuted fracture of the third metacarpal. The bullet passed completely through, leaving only a few small metal fragments.
Case 17–3
Gunshot wound (hand)

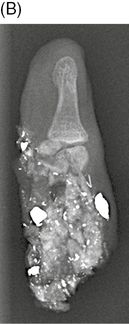
47-year-old man with gunshot wound. PA radiographs of the left hand (A) and left small finger (B). Small bullet and bone fragments are scattered through the hand along the path of the projectile. The bullet entered the hand at the third metacarpal, passed through the fourth MCP joint, and exited through the proximal phalanx of the little finger, amputating it. Low-velocity gunshot wounds have less soft tissue deformity than high-velocity gunshot wounds [1–3]. The mechanism of injury is direct loading along the path of the projectile. Entry and exit wounds may be seen and infection is a potential complication because foreign material is often drawn into the wound. Although the amputated portion of the little finger was recovered at the scene and brought to the hospital with the patient, it was too severely damaged to replant.
Case 17–4
Gunshot wound (carpal bones)


16-year-old male who was struck in the wrist as he attempted to run from gunfire. Lateral (A) and PA (B) radiographs of the right hand. There is a large, intact bullet in the dorsal soft tissues of the left hand. There are comminuted fractures and intercarpal dislocations involving the hamate, capitate, triquetrum, and lunate. There are dislocations of the fourth and fifth CMC joints. There is marked soft tissue swelling of the dorsum of the hand with pockets of gas. A small amount of gas is also seen in the volar aspect of the wrist, corresponding to the entrance wound. The bullet then passed through the ulnar side of the carpus and came to rest in the subcutaneous tissues of the dorsum of the hand.

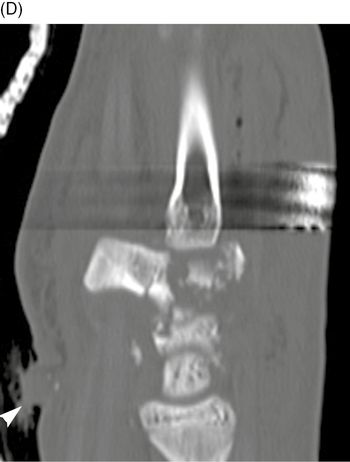

Sagittal (C-D) and coronal (E) CT of the right wrist. There are multiple carpal fractures and a trail of small bone fragments along the trajectory of the bullet. The entry site is at the volar aspect of the wrist (arrowhead), and the bullet passed through the body of the hamate, fracturing it into small pieces.
Case 17–5
Gunshot wound (hand and wrist)


32-year-old man who suffered multiple gunshot wounds. PA (A) and oblique (B) radiographs of the left wrist. Numerous metal fragments obscure the bones and carpal bone fractures are difficult to define, but are undoubtedly present. Fractures of the fourth and fifth metacarpals are evident. The carpal arcs are not clearly delineated and there is some overlap of the proximal and distal carpal row on the PA projection and some ulnar shift of the proximal carpal row as well, which suggests dislocation. Subtle vertical lucencies are seen in the distal radius on the oblique view, indicating additional fractures. Tissue damage sustained by a projectile is governed by several factors, including the kinetic energy of the projectile, propagation of secondary missiles, and cavitation of tissue. The denser the tissue impacted, the greater the transfer of kinetic energy from the projectile, with greater damage to the tissues. Bone, having a relatively high density for biological tissue, sustains greater damage. Fragmentation of the bullet and of the bones, as seen here, releases secondary missiles, which in turn can increase the volume of damage and in some instances cause worse injuries than the primary missile. Low-energy projectiles create cavities only mildly larger than themselves. High-energy projectiles have the capacity to create large cavities and tissue damage and can increase in size even after the projectile has exited. One of the complications with gunshot wounds is infection, a complication seen in about 8% of civilian gunshot wounds to the hand [2].
Case 17–6
Gunshot wound (radius)


23-year-old woman with gunshot wound. Lateral (A) and AP (B) radiographs of the left forearm. Very comminuted fracture of the mid-shaft of the radius is seen from a gunshot wound. The bullet passed completely through the limb, with a trail of bone and metal fragments leading to the exit wound (arrowhead).
Case 17–7
Gunshot wound (humerus)

22-year-old man with multiple gunshot wounds. AP radiograph of the left upper arm. There is a comminuted fracture of the humerus at mid-shaft with multiple bullet fragments at the site, two of them large, representing a low-velocity gunshot wound in which the bullet struck the humerus and did not exit. There is a comminuted fracture of the medial condyle of the distal humerus with multiple small bullet fragments, and missing bone fragments, representing a low-velocity gunshot wound in which the bullet passed through and through, taking bone fragments with it. The distal forearm was noted to be poorly perfused, suggesting brachial artery injury at the humeral shaft.
Case 17–8
Gunshot wound (shoulder)
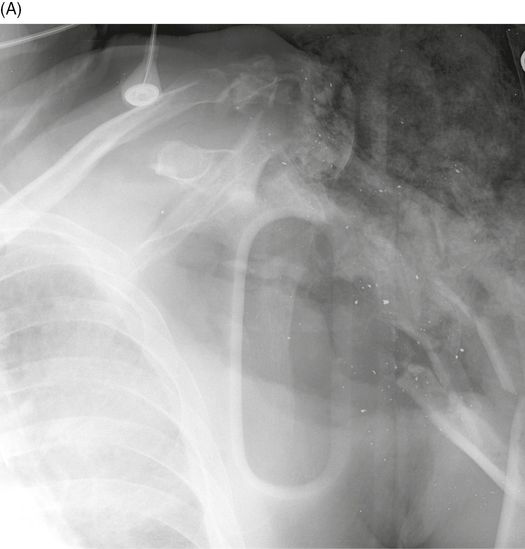

This patient sustained a high-velocity gunshot wound to the shoulder at close range. AP radiographs of the left shoulder (A) and humerus (B). The proximal humerus and surrounding soft tissues have been obliterated, and a temporary dressing packed into the wound at the scene of injury is present. The proximal humeral shaft shows severe splintering with a displacement pattern emanating from the site of entry. The projectile passed completely through the tissues, leaving only a few small fragments of metal.
Case 17–9
Gunshot wound (lumbar spine)

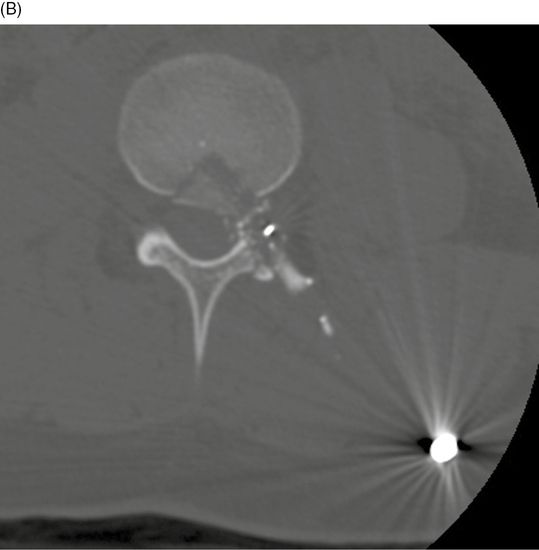
20-year-old man who was shot in the abdomen. Axial CT of the lumbar spine at L3, superior (A) to inferior (B). The entry wound was in the right abdomen, and the bullet passed through L3 vertebral body and left facet joint, coming to rest in the left posterior abdominal wall. A fragment of the vertebral body is displaced into the spinal canal.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


