DEFINITION AND SCOPE
Neurolytic celiac plexus block (NCPB) is a therapeutic analgesic technique predominantly employed in the management of patients suffering from visceral pain due to intra-abdominal malignancies. The block is achieved by the injection of neurolytic solutions (e.g., alcohol or phenol) around the celiac plexus or splanchnic nerves. In view of the inherent risks involved with neurolysis, most practitioners proceed with NCPB only after a positive response to a “prognostic” block performed with local anesthetic. Indications for NCPB primarily include intra-abdominal malignancies, but there is anecdotal evidence to suggest that this procedure may be effective in treating noncancer pain such as that caused by chronic pancreatitis as well.1,2 Pain related to esophageal cancer, gastric cancer, colorectal cancer, gallbladder cancer, cholangiocarcinoma, and liver metastases has been treated effectively with a celiac plexus block.3 It has also been shown to be helpful in the treatment of pediatric patients with hepatoblastoma and neuroblastoma.4,5
The National Cancer Institute estimates that there are over 43,000 new cases of pancreatic cancer each year in the United States alone. Combined with the NCI estimates for the yearly incidence of colorectal cancer (140,000), gastric cancer (21,000), esophageal cancer (16,000), gallbladder cancer (10,000), and cancer of the small intestine (7,000), there are over 200,000 new cases of malignancies amenable to NCBP diagnosed each year in the United States.6 Most frequently though, NCPB is employed in the treatment of pain caused by pancreatic cancer, with some patients experiencing relief for half a year or longer. Anatomical location of the tumor seems to affect the efficacy of the block, with cancer confined to the head of the pancreas showing a more favorable response compared with that involving the body or tail, or spread to other structures.7 This may be because metastatic or direct spread indicates a more advanced tumor. In a randomized controlled trial by Wong et al. involving patients with pancreatic cancer, NCPB was shown to provide superior analgesia to pharmacological therapy, as well as a reduction in systemic opioid use with a concomitant reduction in untoward, medication-related side effects.8 Because NCPB targets the visceral component of pain, celiac plexus block with local anesthetic solutions can also be used as a “diagnostic” test used to differentiate visceral from somatic pain. However, up to 28% of patients who obtain a successful diagnostic celiac plexus block with local anesthetic fail to achieve a positive outcome with neurolytic blockade.9 There is some evidence to suggest that lower baseline opioid doses and not using sedation during the diagnostic block may be associated with positive outcome from NCPB.10
Anatomy
The celiac plexus and splanchnic nerves are responsible for relaying the majority of visceral pain from the abdomen (Fig. 23-1). The celiac plexus is comprised of a complex network of presynaptic sympathetic nerves and ganglia overlying the anterolateral surface of the abdominal aorta surrounding the origin of the celiac artery at roughly the T12/L1 vertebral levels. The largest of all anatomical plexuses, it is made up of nerve fibers branching mainly from the greater (T5-T9), lesser (T10-T11), and least (T12) splanchnic nerves. Postsympathetic fibers leaving the ganglia synapse directly on the upper abdominal organs, excluding the descending colon, sigmoid colon, rectum, and pelvic viscera. Celiac plexus block is often carried out using computed tomography (CT), and this allows direct visualization of the structures that are adjacent to the celiac plexus as well as the structures that lie directly along the path of the advancing needle (Fig. 23-2).
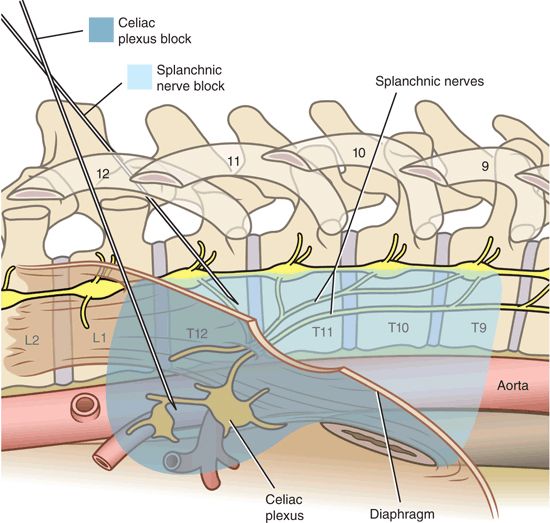
FIGURE 23-1. Anatomy of the celiac plexus and splanchnic nerves. The celiac plexus is comprised of a diffuse network of nerve fibers and individual ganglia located in close proximity to the anterolateral surface of the aorta at the T12/L1 vertebral level. Presynaptic sympathetic fibers travel from the thoracic sympathetic chain toward the celiac ganglia, traversing over the anterolateral aspect of the inferior thoracic vertebrae as the greater (T5-T9), lesser (T10-T11), and least (T12) splanchnic nerves. Celiac plexus block using a transcrural approach places the local anesthetic or neurolytic solution in direct contact with the celiac ganglion anterolateral to the aorta. The needles pass through the crura of the diaphragm en route to the celiac plexus. In contrast, for splanchnic nerve block, the needles remain posterior to the diaphragmatic crura in close apposition to the T12 vertebral body. Shading indicates the pattern of solution spread for each technique. (Reproduced from Rathmell JP. Atlas of Image-Guided Intervention in Regional Anesthesia and Pain Medicine. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2012, with permission.)
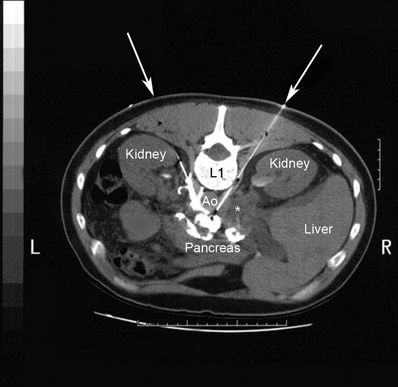
FIGURE 23-2. CT after the placement of two transcrural needles for NCPB. Neurolytic solution (10% phenol in iohexol 100 mg/mL) has been injected through both needles (10 mL on each side). The arrows indicate the approximate needle trajectory on each side. Contrast extends over the left anterolateral surface of the aorta and anteriorly along the posterior surface of the pancreas. There is a large soft tissue mass adjacent to the right-sided needle (asterisk) consistent with lymphadenopathy or metastatic tumor. (Reproduced from Rathmell JP, Gallant JM, Brown DL. Computed tomography and the anatomy of celiac plexus block. Reg Anesth Pain Med 2000;25:411–416, with permission.)
Block Techniques
Celiac plexus blocks can be performed via multiple techniques including posterior and anterior approaches. The posterior approaches can be further classified into transcrural (aka anterocrural), retrocrural (through or adjacent to the vertebral disc), and its variant bilateral splanchnic nerve block (Fig. 23-1). The less frequently employed anterior approach can be further categorized into percutaneous and laparoscopic techniques. In addition, celiac plexus neurolysis can be accomplished intraoperatively by the surgeon under direct visualization. Ideally, the technique utilized should be dictated by the patient’s anatomy, tumor burden, and the likelihood of complications, which can vary based on technique.
Most of the techniques employed for celiac plexus block are described in terms of their relationship to the diaphragmatic crura. The crura of the diaphragm are tendinous structures that extend posteroinferiorly from the diaphragm and attach to the vertebral column. In the transcrural approach, the needles are inserted posteriorly and are advanced such that they traverse the crura and continue to the vicinity of the celiac plexus. This technique places the block solution anterolateral to the aorta in direct contact with the celiac plexus proper. In this approach, the diaphragm can act as a barrier to posterior spread of neurolytic solution, possibly decreasing the likelihood of it contacting and inadvertently damaging a spinal segmental artery or radicular tissue. In the transaortic variation of the transcrural block, generally done from the left side, the abdominal aorta is intentionally pierced in a posteroanterior direction in order to reach the celiac plexus on its anterolateral surface. Tissues traversed by the advancing needle during the transcrural technique include skin, subcutaneous adipose tissue, lumbar paraspinal muscles, the posterior abdominal wall, and the crura of the diaphragm. Structures in close proximity to the passage of the needle are the epidural and intrathecal spaces, the kidneys, and the pancreas.
In the retrocrural approach, the needles begin posteriorly, usually at the cephalad portion of L1, and are advanced superiorly and anteriorly, stopping proximal to the crura. In this technique, the advancement of the needle stops before it reaches the aorta and might therefore reduce the risk of aortic trauma. In addition, smaller volumes of solution are needed for this technique, and the diaphragm works as a barrier to reduce the influence of extensive tumor burden on the spread of the neurolytic solution.
Variations of the classic two-needle retrocrural technique utilize a single-needle approach. In one adaptation, a long needle is inserted under fluoroscopy guidance until the tip is positioned cephalad to the celiac artery to achieve a wider, bilateral spread of neurolytic solution.11 In a second variant, a small-gauge needle is inserted transdiscally through one of the lower thoracic levels, until the tip is situated in the midline just anterior to the annulus fibrosus. A single-needle approach has been shown to decrease fluoroscopy time when compared with the classic technique12 and is probably less painful owing to reduced tissue trauma.13 Traversing an intervertebral disc carries the risk of discitis,14 a higher incidence of nerve root injury, and possibly increased disc degeneration at long-term follow-up.15 Risk mitigation strategies include using a smaller gauge needle to minimize the likelihood of disc degeneration; the judicious use of sedation to diminish the risk of nerve injury; and employing a double-needle technique, which has been postulated to reduce the risk of discitis during lumbar discograms.16 Whereas some experts have advocated prophylactic antibiotics to reduce the risk of discitis, systematic reviews have failed to support this.15,17,18
Splanchnic nerve block is a variant of the retrocrural technique, with the main difference being that it warrants the needles being placed more cephalad at the mid- to anterior border of the T12 vertebral body. Both the splanchnic and classic retrocrural approaches block the splanchnic nerves via the cephalad spread of solution and are essentially the same technique. Whereas arguments have been made advocating the use of one approach over the other, no evidence exists that supports the superiority of either.
In the percutaneous anterior approach, the patient lies in the supine position. The origin of the celiac trunk is identified using ultrasound or CT. After superficial injection of local anesthesia, a 15 cm needle is ultrasonographically guided into the preaortic area near the origin of the celiac trunk where local anesthetic and/or neurolytic solution is injected.19 Pain relief with this technique is comparable to that associated with posterior approaches.20 Advantages of the anterior approach include the fact that it is done with the patient in the supine position, which is significantly more comfortable for many patients with terminal intra-abdominal malignancies. In addition, the needle trajectory does not traverse any major neural structures other than the celiac plexus itself and therefore may be associated with a lower theoretical risk of neurologic complications. Disadvantages of the anterior approach include the possibility of piercing the bowel, and there is a case report of a patient developing a retroperitoneal abscess with the formation of a vascular-enteric fistula following this technique.21 The laparoscopic anterior approach may decrease some of these risks owing to its performance under direct visualization but carries with it the inherent risks associated with general anesthesia.
Neurolytic Solutions
Neurodestructive agents such as ethanol and phenol are typically employed during the neurolytic procedure. The most commonly used neurolytic agent is ethanol. Typical concentrations range between 50% and 100%, with volumes ranging between 20 and 50 mL, though somewhat smaller volumes are needed for retrocrural techniques.22 The mechanism of action of ethanol is thought to be via the extraction of cholesterol and phospholipids from neural cell membranes, causing precipitation of lipoproteins and mucoproteins.9 Ethanol can produce severe pain when injected by itself. Therefore, some experts advocate injecting 5 to 10 mL of local anesthetic 5 minutes prior to the administration of ethanol to minimize discomfort. Another approach is to dilute 100% ethanol by 50% with a local anesthetic.
Some authors have advocated the use of phenol in a concentration >6% because phenol (often mixed with glycerin) induces necrosis when applied directly to the neural tissue.9,23 At lower concentrations, it has reversible local anesthetic effects, rendering it less effective for long-term analgesia. Phenol produces nonselective tissue destruction by denaturing proteins in axons and adjacent blood vessels. The degree of damage after peripheral nerve block is concentration-dependent, and the changes range from segmental demyelination to complete Wallerian degeneration.24 One advantage of phenol is the fact that it is painless on injection. Disadvantages of phenol include its slower and shorter duration of action. Axonal regeneration occurs more rapidly than after ethanol. In addition, its increased viscosity limits its usefulness in clinical practice.
 FREQUENCY AND MECHANISM OF SPECIFIC COMPLICATIONS
FREQUENCY AND MECHANISM OF SPECIFIC COMPLICATIONS
Although NCPB is a relatively safe procedure, it may be associated with a variety of complications. These complications range from minor, often expected untoward effects of successful celiac plexus/splanchnic nerve blockade, to those that are major and life-threatening. The potential for complications must be considered carefully while being cognizant of the fact that in many patients with limited life expectancies associated with intra-abdominal malignancies, the analgesic benefit of the procedure outweighs these risks. Nonetheless, all potential complications should be discussed with patients and/or their legal power of attorney prior to the procedure.
In a randomized controlled study by Wong et al.8 involving 104 NCPBs, the most common complications were weakness or numbness in the T10-L2 distribution (8%), lower chest pain (3%), postural hypotension (2%), failure of ejaculation (2%), difficult urination (1%), and warmth and fullness of the leg (1%). In a review of 2,730 patients conducted between 1986 and 1990, the overall incidence of major complications from NCPB, such as paraplegia and bladder and bowel dysfunction, was 1 in 683 procedures.25
Ischia et al.26 compared three percutaneous NCPB techniques—transaortic approach, classic retrocrural approach, and bilateral splanchnic blocks—in a prospective study involving 61 patients with pancreatic cancer. Although there were no differences in analgesic efficacy or major complications among the various approaches, orthostatic hypotension occurred more frequently with the retrocrural or splanchnic nerve blocks, and bowel hypermotility (e.g., diarrhea) was more common with the transaortic, transcrural technique.
Systemic Complications
When neurolysis is performed with ethanol, acetaldehyde toxicity may occur in individuals who lack the enzyme aldehyde dehydrogenase. This mutation occurs when a lysine residue replaces a glutamate in the active site at position 487 of ALDH-2 and is more common in East Asians. The accumulation of aldehyde in the blood results in palpitations, facial flushing, and hypotension. Alcohol neurolysis can also induce toxic reactions in patients treated with drugs that inhibit acetaldehyde dehydrogenase. In two separate case reports,27,28 patients taking the drugs moxalactam and carmofur that inhibit this enzyme experienced disulfiram-like reactions characterized by temporary flushing, sweating, dizziness, vomiting, and hypotension following alcohol celiac plexus neurolysis. Other agents that possess this property include metronidazole, chloramphenicol, tolbutamide, chlorpropamide, and other β-lactam–type antibiotics.
Some patients who undergo blocks with alcohol may experience systemic effects similar to those observed after ethanol ingestion. Thompson and colleagues found that blood alcohol levels in five patients rose acutely over the first 20 minutes to a peak level of 0.021 g/dL following celiac plexus neurolysis with 50 mL of 50% alcohol.29 Although this is only 25% of the common legal limit for alcohol intoxication, it is possible that cognitive effects may occur when higher concentrations are injected in elderly patients, or those with low body weights. Treatment of systemic complications is supportive in nature, as most are self-limited.
The intravascular injection, or rapid vascular uptake, of phenol may also result in systemic toxicity. In addition to sensory and motor deficits, the intravascular injection of phenol may result in convulsions resulting from an increase in acetylcholine in the central nervous system. Systemic doses of phenol in excess of typical clinical doses (more than 8 g) cause effects similar to those seen with local anesthetic overdose, such as generalized seizures and cardiovascular collapse. This effect may be at least partially due to an increase in acetylcholine in the central nervous system.30 Clinical doses up to 1 g are unlikely to cause serious toxicity in the absence of intravenous injection.31
Neurologic Complications
Neurologic complications from NCPB primarily manifest as sensory and/or motor deficits distal to the celiac plexus in the trunk and lower extremities. Although the incidence is low (1 in 683 procedures resulted in paraplegia),25 major neurologic deficits can cause dramatic reductions in the quality of life. There are multiple proposed mechanisms for these complications. The most widely accepted is the inadvertent injection of neurolytic solution into the vicinity of the neural tissue other than the celiac plexus or splanchnic nerves. Neural structures in close proximity to the needle trajectory that may be accidentally damaged include the spinal cord via the epidural and intrathecal space, thoracic and lumbar nerve roots exiting the vertebral foramen, and the lumbar plexus. Even in the absence of direct contact of these neural structures, interruption of their blood supply can cause necrosis and permanent deficits. Ethanol has been shown to induce vasospasm of the segmental lumbar arteries in dogs, and accidental injection into a radicular artery supplying the spinal cord may be a potential ischemic cause of paraplegia after celiac plexus block (Fig. 23-3).22,32 If arterial vasospasm is suspected, immediate radiological consultation is needed, as previous studies have shown that the timely administration of intra-arterial vasodilators may reverse neurological sequelae.33 It is important to emphasize that the use of radiographic guidance does not provide certain protection from neurologic complications. In a large series of 2,730 patients receiving NCPB, four cases of permanent paraplegia occurred.25 In all four cases, radiographic guidance was used, including the use of radiographic contrast to confirm final needle placement.

FIGURE 23-3. Arterial supply of the spinal cord at the level of low thoracic and high lumbar vertebral levels. The largest feeding artery to the spinal cord is the artery of Adamkiewicz (anterior radicular artery), which branches from the lumbar artery (in this figure).



