
CHEST INJURY
Chest trauma is a significant contributor to patient morbidity and mortality. Thoracic injuries are often accompanied by substantial injuries to other regions. These injuries contribute to approximately 50% of all trauma-related deaths in this country and are the leading cause of death in those under 40-years-old.1–3 Fortunately, most of these injuries can be managed with skills easily acquired by physicians involved in the initial care of the trauma patient. Only 10%-15% will require operative intervention for life-threatening thoracic injuries. The skill set involved in treatment of these severe thoracic injuries is complex and requires a thorough knowledge of thoracic anatomy and cardiopulmonary physiology. This chapter will discuss the diagnosis and management of the spectrum of thoracic injuries as well as indications for intervention.
INITIAL ASSESSMENT
Initial evaluation of the trauma patient follows the guidelines common to evaluation of any patient suspected to have multitrauma. The evaluation begins with a rapid assessment of the elements of the primary survey to evaluate and quickly treat any immediate life-threatening problems. The primary survey is discussed elsewhere in this text, but the specifics of this survey as they relate to thoracic trauma deserve mention here. Injuries that should be identified during the primary survey include tension and open pneumothorax, massive hemothorax, flail chest, and cardiac tamponade. The specifics of treating these injuries will be discussed later in the chapter.
Establishment of an adequate airway is the first priority during this survey. Severely injured patients will require nasotracheal or orotracheal intubation. Some patients with extensive maxillofacial trauma may require cricothyroidotomy or tracheostomy. Once the airway is deemed intact, the next priority is determining the adequacy of ventilation. If the patient is not breathing, endotracheal intubation is indicated immediately. Other sources of ventilatory insufficiency include the presence of open or tension pneumothorax. These injuries must be promptly addressed as soon as they are recognized.
The next priority is hemorrhage control and restoration of adequate circulation. External hemorrhage is best controlled with direct pressure. Inadequate perfusion is most often a result of either hypovolemia or an inadequate pump. Ongoing internal hemorrhage contributing to hypovolemia must be addressed operatively. Distended neck veins signal one of four common traumatic causes of pump failure: tension pneumothorax, pericardial tamponade, coronary air embolism, or cardiac contusion/myocardial infarction. One must rapidly undertake treatment of these problems to restore circulation.
SECONDARY SURVEY AND RADIOLOGIC ADJUNCTS
If there are no immediately life-threatening injuries identified during the primary survey, the trauma team can progress to a more thorough evaluation and physical examination. Secondary survey of the thorax should focus on identification of potentially life-threatening injuries not identified in the primary survey and discovery of other thoracic injuries. Important injuries to recognize during the secondary survey include simple pneumothorax, hemothorax, pulmonary contusion, tracheobronchial injury, blunt cardiac injury, aortic transection, and diaphragmatic injury. Pain from clinically relevant rib fractures will be evident upon palpation of the chest wall. Pneumothorax and hemothorax may become evident at this stage of evaluation if they were not discovered on primary survey. Visualization of chest wall movement during spontaneous respiration can diagnose flail chest.
Important adjuncts to the secondary survey include the portable chest radiograph, the standard and extended Focused Assessment with Sonography for Trauma (FAST) exam, formal echocardiography, and CT angiography. Chest radiography remains a vital first imaging step in the injured trauma patient. Pneumothorax, hemothorax, rib fractures, and mediastinal abnormalities may be identified on a chest radiograph. Extended FAST is useful in rapid diagnosis of pneumothorax and may also assist in diagnosis of pulmonary contusion.4–6 FAST also has an excellent ability to evaluate for hemopericardium with reported sensitivities of 96%-100% and a specificity of 100%.7 The accuracy of these examinations is significantly operator-dependent. Formal echocardiography may be used in later stages of evaluation to assess cardiac function, but it is time consuming and requires appropriately trained personnel. CT angiography is recommended in stable patients with evidence of blunt multisystem trauma, even among those without obvious signs of injury as a substantial number of patients with a normal chest radiograph will have findings of thoracic injury on CT scan.8,9
INDICATIONS FOR OPERATION
Emergency Department Resuscitative Thoracotomy
Emergency department resuscitative thoracotomy (ED-RT) is a drastic measure employed only in patients in extremis after penetrating and, to a lesser extent, blunt trauma. The purpose of this procedure is to attempt to stabilize the patient for transport to the operating room for definitive repair of their injuries. For this reason, the ED-RT must be performed expediently and with clear goals in mind. These goals include relief of cardiac tamponade if present, control of hemorrhage, effective cardiac compression, cross-clamping of the pulmonary hilum in the presence of major lung hemorrhage, air embolism, or massive broncho-pleural fistula, and cross-clamping of the descending aorta for lower torso hemorrhage control. The average survival rate to discharge following this procedure is approximately 7%.10–12
RT has the best chance of success when reserved for those who arrive at the ED and subsequently deteriorate or those who suffered cardiac arrest just prior to arrival. RT should not be performed in those who have had prehospital CPR for longer than 10 minutes in the setting of blunt trauma and 15 minutes in the setting of penetrating trauma or when the initial presenting rhythm is asystole. The survival rate for patients injured by blunt mechanism undergoing ED thoracotomy is reported to be around 1%.12 Survival rates are significantly better for those undergoing this procedure following penetrating trauma; survival to discharge rates of 16%-57% have been reported.10–14 Better outcomes are seen when ED thoracotomy is performed for stab wounds than for gunshot wounds. Worse outcomes are described when ED thoracotomy is performed following multiple gunshot wounds.13
To perform ED thoracotomy, a left anterolateral thoracotomy incision is used to enter the chest. Attention is directed first to the injury. If there is exsanguination from a great vessel, the hemorrhage is controlled with pressure. If air embolism is the cause of the arrest, the hilum is clamped, and air evacuated from the left cardiac chambers. Otherwise, the pericardium is opened anterior and parallel to the phrenic nerve. The hemopericardium is evacuated, the cardiac injury is controlled with digital pressure, and a temporary repair is performed. After the cause of the arrest has been addressed, the descending thoracic aorta is occluded with a vascular clamp or digital pressure, and intrathoracic cardiac compression is initiated. The patient’s intravascular volume is restored, and electrolyte imbalances are corrected. If the patient can be saved, he or she is transported to the OR for definitive repair and closure.
URGENT THORACOTOMY
Urgent thoracotomy in the trauma patient is indicated for suspicion of life-threatening injuries that may require surgical repair. Indications for operative treatment of thoracic injuries fall into four broad categories: (1) hemorrhage, (2) major airway disruption, (3) cardiac and vascular injuries, and (4) esophageal disruption. For hemorrhage, operative intervention is indicated by the volume of chest tube output in combination with the hemodynamic profile of the patient. In general, thoracotomy is indicated when chest tube output initially exceeds 1,500 mL initially or if ongoing bleeding exceeds 300 mL per hour for 3 hours. There are, however, pitfalls inherent in this method of determining need for operation. A caveat to chest tube output as an indication for thoracotomy is chest trauma with a delayed presentation and the presence of a coagulopathy. Patients presenting with chest trauma in a delayed fashion may have a substantial hemothorax that has accumulated in the time it has taken the patient to arrive in the ED. Furthermore, in some instances, a tube thoracostomy is malpositioned, kinked, or clotted, allowing accumulation of a hemothorax prior to arrival. In these situations, placement of a second chest tube and/or evidence of ongoing bleeding rather than an absolute amount may be a more reliable indicator of the need for thoracic operation.15 In addition to chest tube output, patient physiology suggestive of ongoing hemorrhage should play a role in the decision for operative intervention. Low-tube thoracostomy output due to a malpositioned tube may also be misleading. As a result, a chest radiograph should be obtained following tube placement to determine whether the hemothorax has been adequately evacuated. Complete lung re-expansion should also be confirmed on this film, as hemostasis in the chest often will not occur until expansion is complete. Massive air leak after chest tube placement or the presence of gastric or esophageal contents in the chest tube effluent are also indications for operation.
The order of an exploratory thoracotomy should proceed in a logical and orderly fashion. If the diagnosis is uncertain, a posterolateral thoracotomy is the incision of choice. With a known diagnosis, the incision should be chosen to provide optimal exposure of the injury. First, the remaining hemothorax should be evacuated. The lung is then packed out of the field; this procedure may be facilitated by the division of the inferior pulmonary ligament. The mediastinum and pericardium should be evaluated carefully for bleeding. It is difficult to detect the presence of blood in the pericardium by simple visual inspection. A small (5 mm) pericardotomy that can be expanded as necessary is useful to confirm or exclude the presence of hemopericardium. The presence of clear fluid in the pericardium precludes the need for creating a larger pericardial incision. Major vascular injuries are isolated using proximal and distal control; hilar control can be used in cases of pulmonary parenchymal bleeding. Formal repair of injuries may then proceed. The use of a double lumen endotracheal tube or bronchial blocker may be useful and should be considered when patient physiology and injury pattern permit.
INCISION CHOICE
Appropriate incision choice is essential for obtaining adequate exposure of thoracic injuries requiring operative intervention. The choice of incision varies according to several factors, including suspected site of injury and the indication for operation, the urgency of the situation, the presence of associated injuries, the mechanism of injury, and the results of preoperative studies. For injuries that are suspected or diagnosed preoperatively, the choice of approach to the affected structure is greatly simplified (Table 27.1). Preoperative imaging using CTA in the stable patient, even with penetrating mechanism, can assist with the identification of specific injuries and operative planning.16
TABLE 27.1
SURGICAL APPROACHES FOR TRAUMATIC INJURIES TO THORACIC VESSELS
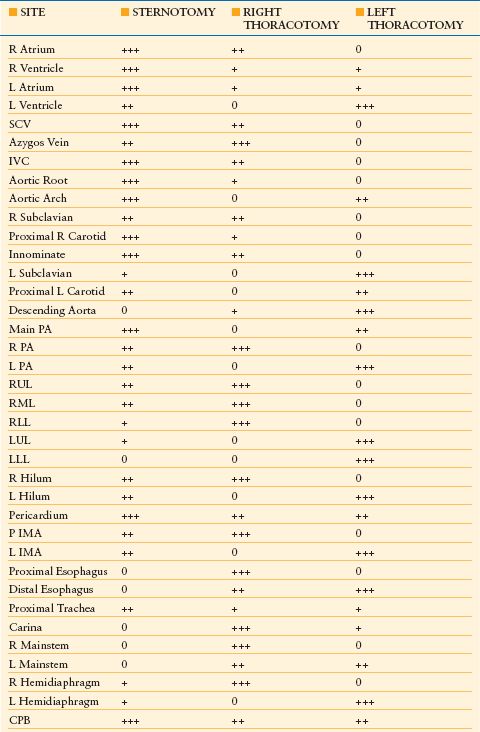
CPB, cardiopulmonary bypass; IMA, internal mammary artery; IVC, inferior vena cava; LL, lower lobe; ML, middle lobe; PA, pulmonary artery; SVC, superior vena cava; UL, upper lobe.
+++, preferred; ++, acceptable; +, with difficulty; 0, not acceptable.
A median sternotomy is one of the more versatile thoracic incisions. It can be opened and closed more quickly than a thoracotomy, is associated with less postoperative pain, and may be less likely to result in contamination of the dependent hemithorax, which may occur with the patient in a lateral position during thoracotomy. In general, a median sternotomy provides the best exposure of the right-side cardiac chambers, the ascending aorta, the aortic arch, and the arch vessels (excluding the left subclavian artery), and it provides adequate exposure of the right lung and hemidiaphragm. A sternotomy may be extended into the neck or supraclavicular fossa to enhance exposure of the great vessels. The main limitation of this incision is that it does not provide exposure of the posterior mediastinal structures (Fig. 27.1).
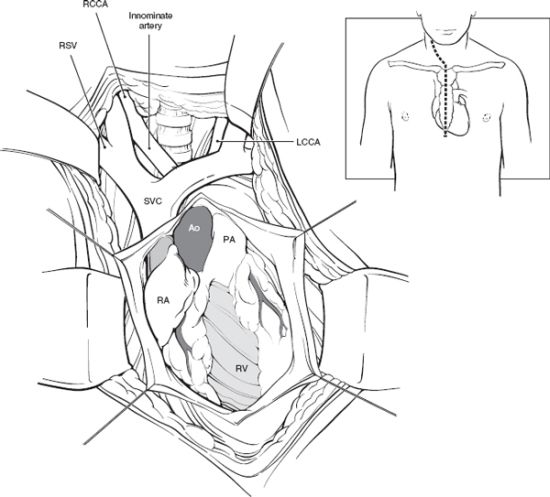
FIGURE 27.1. Median sternotomy with optimal extension. A median sternotomy provides excellent exposure for the right atrium and ventricle, the superior vena cava, atrial appendage, right pulmonary artery, and lung. If necessary, the incision may be extended into the neck or supraclavicular fossa (inset) to enhance exposure of the great vessels. Ao, aorta; LCCA, left common carotid artery; PA, pulmonary artery; RA, right atrium; RCCA, right common carotid artery; RSV, right subclavian vein; RV, right ventricle; SVC, superior vena cava.
For the exploration of lateral stab or gunshot wounds or massive hemothorax, a posterolateral thoracotomy on the side of the injury is the incision of choice. The fifth interspace thoracotomy is the most versatile approach to ipsilateral pulmonary and mediastinal pathologic states. Exposure can be markedly enhanced by the removal of the fifth rib. Right thoracotomy is an excellent approach for right lung, tracheal, and proximal left mainstem bronchial injuries. Most injuries of the thoracic esophagus can also be accessed in this manner, except in the case of distal esophageal injuries, which are best approached via left thoracotomy. The right atrium and ventricle are easily exposed by a right thoracotomy as well. Left thoracotomy is ideal for the exposure of the left lung, left pulmonary hilum, aorta, proximal left subclavian artery, left heart chambers, distal esophagus, and distal left mainstem bronchus (Fig. 27.2). In urgent/emergent situations, a clamshell incision, formed by extending a left anterolateral thoracotomy incision transversely across the sternum, provides access but only suboptimal exposure of intrathoracic and mediastinal structures except the right ventricle and atrium (Fig. 27.3).
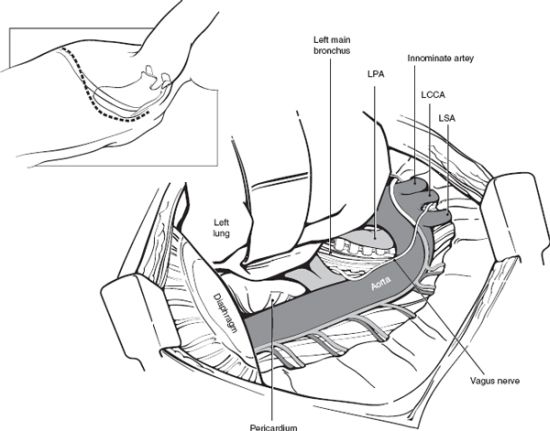
FIGURE 27.2. Left posterolateral thoracotomy. A left posterolateral thoracotomy (inset) provides excellent exposure of the left pulmonary hilum, left lung, proximal left subclavian artery, descending aorta, distal esophagus, and left diaphragm. LCCA, left common carotid artery; LPA, left pulmonary artery; LSA, left subclavian artery.
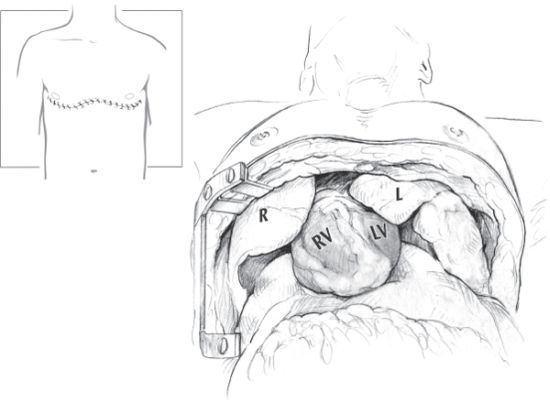
FIGURE 27.3. Clamshell extension of left anterolateral thoracotomy. In urgent/emergent situations, a clamshell incision, formed by extending a left anterolateral thoracotomy incision, transversely across the sternum, provides access but only suboptimal exposure of intrathoracic and mediastinal structures except the right ventricle and atrium. R, right lung; RV, right ventricle; LV, left ventricle; L, left lung.
THORACIC DAMAGE CONTROL
While damage control is critically important in abdominal trauma, it is less frequently needed in thoracic trauma. In most instances, serious bleeding from thoracic structures is unlikely to be controlled with packing; however, severe coagulopathy occasionally prevents definitive repair and necessitates abbreviation of surgery and temporary closure of the chest by suturing or stapling the skin incision only.17 The two most common locations of injury in these scenarios are the lung and the chest wall. Hemorrhage from lung lacerations in patients with metabolic exhaustion generally should not be treated with formal anatomic resection: stapled wedge resection, tractotomy, or simple suture repair is more appropriate. In patients with persistent chest wall bleeding that is not associated with a major vessel, treatment with lung re-expansion for local tamponade and correction of coagulopathy usually suffices. Patients who have air embolus or massive bronchopleural fistula will require temporary clamping or twisting of the pulmonary hilum on the affected side, so that the patient may be stabilized prior to proceeding with definitive operation. In rare circumstances, complex esophageal injuries may be associated with extensive loss of tissue, necessitating rapid exclusion and proximal diversion. In most patients with any chance of survival, however, the surgeon should attempt primary closure of the injury, buttressing the repair with autologous tissue, and employing wide drainage. Even with large defects, this approach has a surprisingly high rate of ultimate success. The VAC dressing may be employed for temporary closure when definitive closure of the thorax is not possible.
INDICATIONS FOR DELAYED THORACOTOMY
Indications for delayed thoracotomy include missed tracheobronchial injuries, traumatic aortic rupture, intracardiac injuries, retained hemothorax, and posttraumatic empyema. Specifics of intervention for these injuries will be discussed in the ensuing sections.
MANAGEMENT OF SPECIFIC INJURIES
Chest Wall Injuries
Rib Fractures. Rib fractures are quite common following blunt trauma and can be present in as many as 10% of total trauma admissions. These injuries rarely require operative stabilization, but they do contribute significantly to patient morbidity and mortality. Rib fractures carry a risk of 12% for mortality and 33% for pulmonary complications.18 Rib fractures in the elderly are associated with especially high morbidity and mortality. The mortality associated with rib fractures is twice as high in patients older than 65 years than in younger patients, and the relative increase in the incidence of pneumonia in older patients is even higher, even after patient comorbidities are considered.19,20
The main pathophysiologic consequences of rib fractures are pain, splinting, and prevention of adequate cough, impeding pulmonary toilet. The diagnosis should be suspected if pain or splinting occurs on deep inspiration, and it is confirmed by careful physical examination, consisting of anterior–posterior and lateral–lateral manual compression. If an alert patient feels no pain with these maneuvers, clinically important rib fractures can be excluded. Although rib fractures are often identified on routine chest radiographs, they are more likely to be detected on rib-detail films, which are rarely clinically indicated. A variant of rib fracture that falls into the same physiologic category is costochondral or costosternal separation. This condition is usually detected during physical examination or on CT scan of the thorax but is not seen on routine chest radiographs.
Pain from isolated rib fractures can usually be adequately managed with oral or parenteral analgesics, encouraging good pulmonary toilet, and use of thoracic epidural anesthesia (discussed below) in select patients. We mention chest wall strapping, taping, and bracing only to condemn these practices. Binding devices generally restrict tidal volume and thus promote rather than prevent atelectasis and pulmonary complications. Increasingly, reports have demonstrated the feasibility of rib fracture repair using a variety of different methods including wire sutures, intramedullary wires, staples, and various plating systems.21 Potential indications for operative repair of rib fractures include flail chest, painful, and mobile rib fractures, which are refractory to conventional management, chest wall deformity/defect, rib fracture nonunion, and during thoracotomy for other indications. In isolated reports, clinical outcomes have been excellent when repair is undertaken. However, there is a need for clinical trials documenting the superiority of rib fracture repair versus conventional management in select patient populations and defining indications for repair.22,23
Sternal Fractures. Sternal fractures commonly result from motor vehicle collisions and are associated with the use of three-point restraints. Isolated sternal fractures are relatively benign, having a low incidence of associated cardiac, great vessel, and pulmonary injuries. Sternal fractures in unrestrained occupants and victims of crush injuries, however, are commonly associated with underlying visceral injuries, which must be excluded.17,24
The diagnosis of sternal fracture is based on the presence of severe pain, often associated with instability on sternal palpation. In many cases, physical examination can clarify the nature of the fracture. Sternal fractures are almost invariably transverse, with the majority occurring at the sternomanubrial joint or in the midbody of the sternum. They may be characterized as simple (two fragments) or comminuted (multiple fragments), as displaced or aligned, or as stable or unstable. The fragments of an unstable fracture move substantially with activity.
Initial management of a sternal fracture is directed toward resuscitation and identification or exclusion of other life-threatening injuries. In patients with isolated sternal fractures, a normal electrocardiogram and a normal chest radiograph suggest that associated serious injuries are unlikely. If the pain is controlled with oral analgesics, these fractures can usually be managed on an outpatient basis. Displaced fractures may be reduced by the simple (albeit painful) maneuver of having the patient simultaneously raise his or her head and legs from the bed. Such a position requires contraction of the rectus abdominis, which distracts the caudad segment inferiorly, and the sternocleidomastoid muscles, which retract the cephalad segments superiorly. The physician can then depress the anterior segment and allow the patient to relax. This measure often suffices for alleviation of subsequent pain and sometimes constitutes adequate long-term treatment.
The vast majority of sternal fractures heal without repair. Those that are unstable or are displaced by more than 1 cm of overlap are more likely to exhibit malunion or nonunion and subsequent chronic pain; they may require open reduction and internal fixation. Occasionally, a patient with a clinically stable, minimally displaced sternal fracture associated with lower extremity injuries who requires crutches for ambulation, experiences such disabling sternal pain during ambulation that fracture repair is necessary. Sternal fractures may be repaired with either of two operative techniques. In both, the sternum is approached via either a vertical midline incision or a sweeping transverse inframammary incision similar to that used for repair of pectus excavatum. The fracture is exposed, and the ends are mobilized and fixed with either reconstruction plates or No. 6 sternal wires. Both wire fixation and plate fixation are well tolerated and are appropriate for properly selected patients.
Flail Chest. Flail chest is defined as the presence of two or more ribs fractured in two or more places, resulting in paradoxical movement of a section of the chest wall. It is the most serious of the chest wall injuries caused by blunt trauma. Although flail chest may present as an isolated injury, it is much more commonly associated with other injuries.25 The diagnosis may be suspected based on radiologic findings and confirmed by examination of the spontaneously breathing patient. The flail segment may be overlooked in the patient receiving mechanical ventilation because of the absence of paradoxical movement.
There are three important pathophysiologic components that contribute to the severity of flail chest. The first is the alteration in chest wall mechanics secondary to the flail segment. Although this is usually not the most clinically important abnormality, the paradoxical motion of a large flail segment occasionally impairs the patient’s ability to achieve an adequate tidal volume or an effective cough. The second important pathophysiologic component is underlying pulmonary contusion. In the vast majority of serious flail chest injuries, this is the most important physiologic aberration.26 In the contused portion of the lung, there is extravasation and accumulation of blood and fluid in the alveolar air space, which results in sufficient shunting to produce hypoxemia. The third factor is the pain of multiple rib fractures, leading to splinting and diminution of tidal volumes; it prevents adequate coughing and pulmonary toilet. The combination of depressed tidal volume and inadequate cough leads to hypoventilation, atelectasis, and often pneumonia.
Central to management of the flail chest is the concept that the injury is not static but is in constant evolution. Frequent re-evaluation is essential; prompt intervention should be undertaken when patient physiology changes. All awake and alert patients with adequate oxygenation and ventilation deserve a trial of management without intubation.27 Pain cannot be eliminated entirely, but it usually can be diminished sufficiently to allow an adequate tidal volume and a forceful cough. Oral analgesics rarely suffice for patients with even a small flail segment; stronger agents are required for all but the most stoic of patients. Parenteral narcotics are effective, especially when administered in a patient-controlled analgesia (PCA) device. Potential disadvantages of parenteral narcotics include excess sedation, cough suppression, and respiratory depression.
When PCA analgesia is not adequate or is contraindicated, other modalities of analgesia may be considered. These methods include epidural analgesia, intercostal nerve block, intrapleural anesthesia, and thoracic paravertebral block. Each of these modalities has inherent risks and benefits, and choice of analgesia should be based on patient physiology, injuries, and medical history.
Epidural analgesia is the most common method used for the treatment of chest wall pain. It consists of insertion of a catheter into the thoracic or lumbar epidural space with infusion of a narcotic, a local anesthetic, or most commonly, a combination of the two medications. Purported benefits include improved analgesia as well as improvement in respiratory mechanics and decrease in proinflammatory cytokines.28,29 The benefits of epidural analgesia may translate into decrease in ventilator days, decrease in pulmonary complications, and lower mortality.19,30 Disadvantages include the potential for epidural infection and hematoma as well as direct spinal cord trauma. Hypotension (when local anesthetic agents are used), peripheral neurologic effects, and pruritus are also potential side effects.
The Eastern Association for the Surgery of Trauma (EAST) has published recent guidelines regarding the use of analgesic adjuncts. These guidelines state that epidural analgesia is the preferred method of pain relief for blunt chest wall injury. They recommend epidural analgesia for patients who are ≥65-years-old if there is no contraindication, and they state that it may be considered for those under 65 years as well.31 When epidural analgesia is contraindicated, another regional anesthetic technique may be considered. These other techniques, including intercostal nerve block, intrapleural analgesia, and paravertebral block, are relatively safe but have not been studied extensively in the trauma population.
The decision-making process for the management of flail chest should begin with the assessment of the patient’s ability to cough. If the patient is able to clear tracheal secretions, then observation in an acute care setting with small, infrequent doses of narcotics, is appropriate. If the patient has no cough or has a very truncated cough that moves secretions but does not propel them into the oropharynx, an aggressive program to promote pulmonary toilet should be instituted. If a sufficiently vigorous cough cannot be achieved and there is no specific contraindication, an epidural catheter is considered, and the patient is followed closely with frequent physical examinations in the intensive care unit. Ambulation is encouraged, and frequent coughing is required. It is important that management decisions be made early, so that effective therapy can be started expeditiously. There is no role for antibiotic prophylaxis or steroid use in the management of patients with flail chest or pulmonary contusion.
Any patient with flail chest demonstrates that further deterioration of pulmonary function as evidenced by worsening hypoxia or hypercarbia should undergo endotracheal intubation and mechanical ventilation. Goals of mechanical ventilation include the establishment of tidal volume adequate for normal chest wall excursion and maintenance of normocarbia through an adequate respiratory rate. Hypoxia is managed by increasing the fraction of inspired oxygen (FiO2) and applying sufficient positive end-expiratory pressure to achieve adequate oxygenation (usually defined as arterial oxygen saturation >90%) with nontoxic levels of FiO2.
A few patients with severe disruption of chest wall mechanics as a result of flail chest continue to require positive pressure ventilation even though adequate pain control has been achieved, and the pulmonary contusions are beginning to resolve. Some of these patients may benefit from internal fixation of the multiple rib fractures, which restores chest wall stability and eliminates much of the fracture-related pain. A variety of methods have been described to stabilize the ribs and obtain compression osteosynthesis of each fracture site. Two single institutional series describe the efficacy of this procedure in patients with flail chest.32,33 Further clinical trials are needed to better define indications for fracture repair.
Penetrating Chest Wall Injury
In most cases of penetrating thoracic trauma, the injury to the chest wall is vastly overshadowed by the injury, or potential for injury, to the intrathoracic structures. The notable exceptions to this general rule are hemorrhage and open chest wounds.
Hemorrhage. Stab wounds and low-caliber gunshot wounds to the anterior chest are common in urban areas. Once serious injury to intrathoracic organs has been excluded, such injuries often can be managed with tube thoracostomy or observation alone. Indications for urgent thoracotomy have been discussed previously.
In patients with persistent hemorrhage from chest tubes who require thoracotomy, the most common source of the bleeding is a lacerated internal mammary or intercostal artery. Attempts to control bleeding from these vessels nonoperatively usually fail. Angiography to localize the bleeding vessel is unnecessary and delays definitive care; coupled with embolization of the lacerated vessel, it is more time-consuming than surgical intervention and does not address associated injuries and hemothorax.
Penetrating wounds to the midportion of the pectoral muscle occur with surprising frequency, possibly as a result of an assailant’s erroneous conception of the location of the heart. Such injuries often lacerate the pectoral branch of the thoracoacromial artery, which courses along the posterior surface of the pectoral muscle. Control of this troublesome bleeding is extremely difficult to achieve if exploration is attempted directly through an extension of the entrance wound. Exposure is much improved if exploration is attempted through an oblique wound along the lateral pectoral margin after entry into the subpectoral plane.
Open Chest Wounds. The diagnosis of an open chest wound is usually obvious, and treatment of this wound depends on the size of the wound the chest wall defect. Most small open pneumothoraces can be managed initially with occlusive dressings, but there is usually an underlying pulmonary injury with air leakage, which necessitates early tube thoracostomy to prevent tension pneumothorax. Once the patient’s condition is stable, the wound can be débrided and closed. Occasionally, primary skin closure must be delayed.
Larger chest wall defects pose a challenging therapeutic problem. Such wounds usually result from high-velocity missiles or shotguns fired at close range. Initial management is directed toward restoration of respiratory mechanics with early intubation and mechanical ventilation.
The next priority is to address any underlying intrathoracic injuries, which may range from mild pulmonary contusion to massive hemorrhage in conjunction with severe lung or hollow viscus injury. When associated intrathoracic injuries are present, the first step in the closure of the defect is to select an appropriate operative approach. Although the primary objective in this situation is to provide adequate exposure for repair of what may be life-threatening injuries, whenever possible, the thoracotomy should be performed in such a way as to preserve the blood supply and muscle mass of the chest wall adjacent to the defect.
After definitive repair of intrathoracic injuries and debridement of devitalized chest wall tissue, planning begins for wound closure. Such planning requires a degree of familiarity with current and developing techniques and an understanding of pleural drainage, respiratory mechanics, and techniques of tissue transfer. Collaboration with plastic and thoracic surgeons is often helpful. Most chest wall defects can be closed with viable autogenous tissue, usually through rotation of local myocutaneous or myofascial flaps of the pectoral muscle, the latissimus dorsi, or the rectus abdominis.
Pleura and Lungs
Pneumothorax. Pneumothorax occurs when there is injury to the lung and/or tracheobronchial tree, resulting in air in the pleural space. A simple pneumothorax requires tube thoracostomy when it is large enough to be seen on plain chest radiograph. With the advent of modern imaging techniques, even clinically insignificant pneumothoraces may be identified during evaluation of the patient. If a pneumothorax is seen on thoracic CT but not on plain chest radiograph, it is known as an occult pneumothorax. Studies have examined the need for tube thoracostomy in these cases. The majority of evidence indicates that asymptomatic occult pneumothoraces may be observed, regardless of the need for positive pressure ventilation.34–38 Patients with occult pneumothoraces who are treated without tube thoracostomy should be observed for at least 24 hours with repeat chest radiography to ensure the pneumothorax has not enlarged.
Progression of simple pneumothorax leads to tension pneumothorax, a life-threatening injury that should be recognized on primary survey. Air released from the lung parenchyma and tracheobronchial tree continues to accumulate in the pleural space, leading to an increased intrapleural pressure. This pressure is transmitted to the cardiac chambers and vena cava, impeding venous return to the heart and ultimately resulting in cardiovascular collapse. This entity may be recognized by unilateral decreased breath sounds, tympany on the affected side, tracheal deviation, and distension of neck veins. However, these signs may be absent or go unrecognized in a busy ED. The diagnosis is often suggested by the presence of shock accompanied by the evidence of inadequate venous filling on physical examination as well as recognition of asymmetric chest wall motion.
Radiographic evaluation should not delay treatment of a suspected tension pneumothorax with tube thoracostomy in patients with hemodynamic compromise.
Hemothorax. Hemothorax may occur in isolation or present in combination with pneumothorax. Hemothorax may be recognized on plain chest radiography as well as on thoracic CT. If the volume of hemothorax is great enough (massive hemothorax), physiologic compromise occurs in a manner similar to that of tension pneumothorax. Initial treatment of hemothorax is similar to the treatment of pneumothorax. After placement of tube thoracostomy, initial tube output as well as ongoing output should be carefully monitored. Indications for urgent thoracotomy based on tube thoracostomy output have been previously outlined.
The goal of treatment with tube thoracostomy is complete removal of blood. Prophylactic antibiotics for tube thoracostomy placement are not currently indicated.39 Complications such as atelectasis and empyema after chest trauma are clearly related to the presence of residual blood, fluid, and air, as can occur secondary to improper positioning (i.e., within a fissure) or obstruction of the tube. A retained hemothorax is suggested by the presence of a persistent opacification in the pleural space in a patient with a known previous hemothorax. However, plain chest radiography can be misleading and often underestimates the amount of fluid in the chest. The radiodensity seen can be confused with adjacent pulmonary contusion or atelectasis. Thoracic CT confirms the diagnosis, providing information about the size and location of the hemothorax that can be used intraoperatively to make the appropriate incision. Evacuation of hemothorax is indicated, as blood can serve as a nidus for infection.40 If the hemothorax is incompletely evacuated using a functional single tube, placement of a second tube is unlikely to be helpful in removing clotted blood and may likely increase the risk of infection.41
Thus, an operative approach is needed. When used early (<5 days after injury), video-assisted thoracic surgery (VATS) has been shown to be cost-effective method for managing clotted hemothoraces and free-flowing blood in patients who ideally can tolerate single-lung ventilation. However, VATS reduces the surgeon’s ability to control bleeding and perform definitive repair of injuries; thus, in patients who have ongoing bleeding, posterolateral thoracotomy is required.42–44 It is our practice to routinely obtain chest CT when patients have persistent pleural effusion after tube thoracostomy on chest radiograph within 48 hours of injury. In patients confirmed to have a persistent pleural effusion, we proceed directly to VATS as it is well documented that delaying the operation increases the technical difficulty of the procedure and rate of conversion to thoracotomy.45,46
Empyema Thoracis. Empyema thoracis is a troublesome complication after chest trauma, occurring in approximately 1.5%-5% of patients.39,40,47,48 Possible causes include retained hemothorax, pneumonia with parapneumonic effusion, persistent foreign body, ruptured pulmonary abscess, bronchopleural fistula, esophageal leakage, and tracking through the intact or injured diaphragm from an abdominal source. Empyema may be difficult to diagnose in the posttraumatic setting and must be differentiated from pleural thickening, pulmonary contusion, or uninfected effusion. Thoracic CT with intravenous contrast usually demonstrates a fluid collection with loculations or an enhancing rim. Such findings, coupled with a clinical scenario of low-grade sepsis, worsening respiratory function, or failure to thrive, are diagnostic. Analysis and culture of fluid obtained at thoracocentesis or chest tube placement typically confirm the diagnosis, but the fluid may be sterile if the patient is already receiving antibiotics.
Antibiotic therapy, either broad-spectrum or specifically directed against cultured organisms (usually gram-positive pathogens), is certainly an important component of therapy for empyema thoracis, but the primary goal is the removal of the infection while the fluid is still thin. When this goal is met, a more modest therapeutic procedure can be performed, there is less risk that a restrictive pulmonary peel will develop, and the injured patient recovers faster overall. Rarely, in the early stages, tube thoracostomy may suffice for treatment; more commonly, the infected pleural process cannot be completely evacuated via chest tube because of thicker fluid, loculations, or pleural adhesions. In these cases, VATS or a formal thoracotomy with decortication is generally required.
Decortication is the cornerstone of effective therapy for posttraumatic empyema. Emphasis should be placed on completely removing the visceral pleural peel to allow complete lung expansion postoperatively. Decortication should not be undertaken in the face of severe sepsis. Instead, antibiotics and drainage (via tube thoracostomy, CT-directed catheter placement, or open rib resection) should be employed until the sepsis is controlled. Once the patient’s condition has stabilized, decortication may be performed. In cases of early empyema, VATS has been successfully used for lysis of adhesions and removal of fluid.48,49 Because of the limited capacity for performing pleurectomy with this procedure, VATS should not be used when thick peel or a trapped lung is present.
Pulmonary Contusion. Pulmonary contusions are bruises to the lung that are caused by either blunt or penetrating trauma. The contused segment of the lung has a profound ventilation–perfusion mismatch, which produces an intrapulmonary right-to-left shunt and hypoxia. The clinical sequelae of lung contusion vary from simple shortness of breath to respiratory failure requiring mechanical ventilation. Lung contusion results in systemic activation of the innate immune system as evidenced by local and systemic production of various inflammatory mediators such as the interleukins, prostaglandins, and chemokines. This resultant inflammatory response contributes to the evolution of pulmonary and remote organ dysfunction.50 The contusion is usually not fully evident on plain chest radiograph but is better imaged with thoracic CT. The size of the contusion has been found to be directly proportional to the risk of developing acute respiratory distress syndrome.51 Lung contusion is a well-established risk factor for pneumonia, and the bruised lung also may serve later as a source of sepsis.
Most pulmonary contusions that are not complicated by excessive attempts at resuscitation or by superinfection resolve over 3–5 days. Cardiovascular and ventilatory support is provided. In general, pulmonary contusion is treated in much the same fashion as flail chest. Patients with rib fractures and painful chest wall excursions must be given sufficient analgesic support to allow them to produce a forceful cough. Intubated patients should undergo suctioning frequently. Patients with pulmonary contusions who require substantial volume resuscitation should be considered for pulmonary arterial catheter monitoring. Steroids are not indicated, because they have no effect on the development or resolution of the contusion and because they set the stage for subsequent infection. Diuretics and prophylactic antibiotics are also unnecessary.
Pulmonary Lacerations. Bleeding pulmonary lacerations can be oversewn, resected, or explored via pulmonary tractotomy. Bleeding from small or shallow lacerations can be controlled with a continuous monofilament suture. Bleeding from deeper lacerations is controlled with resection or tractotomy. Most pulmonary resections for trauma should be stapled, nonanatomic resections. However, anatomic lung resection is required in rare instances, and trauma surgeons should remain familiar with the technical aspects of this procedure. Mortality is proportional to the amount of lung tissue resected: with suture repair alone, mortality is 9%; with tractotomy, 13%; with wedge resection, 30%; with lobectomy, 43%; and with pneumonectomy, 50%.52,53
Tractotomy is especially useful for deep through-and-through injuries that do not involve the hilum.54 In this technique, the injury tract is opened with a linear stapler or between two aortic clamps. If clamps are used, the cut lung edges are oversewn and the tract left open (Fig. 27.4). Tractotomy exposes bleeding vessels and air leaks inside the tract and permits selective ligation. Occasionally, it exposes an injury to a major vascular or airway structure that must be treated with a formal resection. Because of the risk of exsanguination or excessive devitalization of lung tissue, tractotomy is not indicated when the injury traverses the hilum or when the entire thickness of a lobe will be cut.
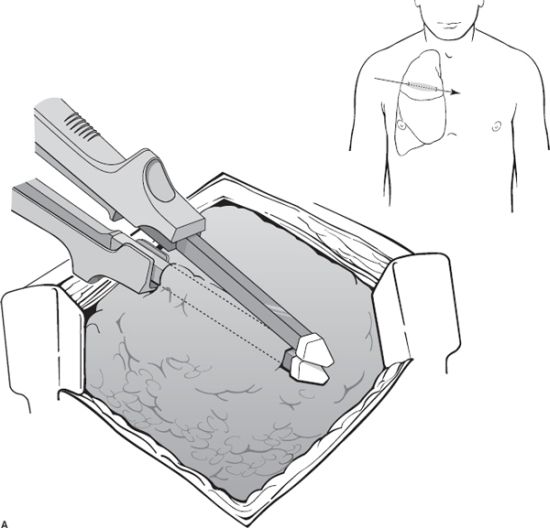
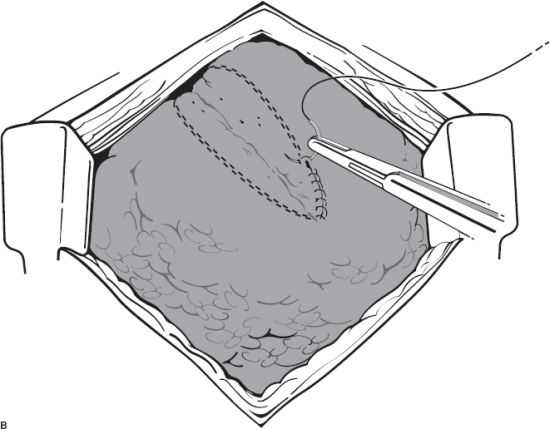
FIGURE 27.4. Tractotomy for nonhilar pulmonary injuries. A: The principle is to open the tract of the bullet or knife wound (inset), so that larger interior vessels may be identified and ligated individually. B: 3-0 polypropylene suture may be used to individually ligate the vessels or may be run along the length of the tractotomy.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


