Fig. 32.1
Typical distribution of anesthesia and analgesia following successful axillary plexus blockade [13] (With permission from Danilo Jankovic)
It may be performed as either a single-shot or continuous catheter technique; however it can be more difficult to maintain hygiene of the catheter insertion site compared to other brachial plexus approaches.
Contraindications
Absolute
Inability to abduct the arm at the shoulder and access the injection site
Generic contraindications such as patient refusal, allergy to local anesthetics, and local infection at the site of injection apply as usual
Relative
Previous axillary node clearance
Congenital or acquired vascular malformations in the upper arm or axilla (e.g., arteriovenous fistula), although the ultrasound-guided approach may still be feasible in skilled hands
Advantages Compared to Other Brachial Plexus Block Techniques
1.
The ultrasound-guided technique is a highly efficacious technique, with block success rates as high as 97.5 % reported [2].
2.
It is a superficial site that is easily compressible and carries a low risk of compressive injury to surrounding structures by hematoma formation. This makes it a viable option in coagulopathic patients, particularly if ultrasound guidance is used.
3.
There is no risk of pneumothorax or of adverse effects associated with injections administered more proximally in the root of the neck, e.g., phrenic nerve palsy and Horner’s syndrome.
4.
Adequate ultrasound images can be obtained even in very obese patients.
Disadvantages Compared to Other Brachial Plexus Block Techniques
1.
The axillary block can only be performed with the arm abducted (and ideally externally rotated) at the shoulder.
2.
The landmark-guided techniques of axillary block have relatively poor block success rates, especially if single-injection techniques are used. Multiple-injection techniques are complex and require good understanding of anatomy as well as dexterity with needle and nerve stimulator.
Functional Anatomy
At the level of the axillary block, the cords of the brachial plexus have divided into the major terminal nerves: the median nerve, ulnar nerve, radial nerve, musculocutaneous nerve, and medial brachial and antebrachial cutaneous nerves (Fig. 32.2). These last two nerves are not usually sought out separately as they lie close to the ulnar nerve and are readily anesthetized with it.
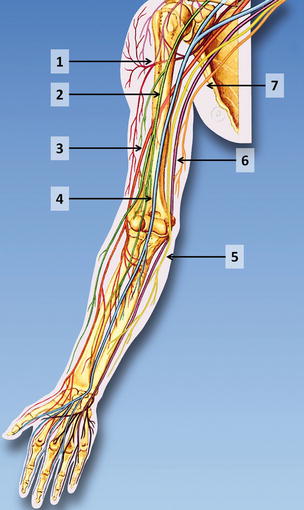
Fig. 32.2
Major terminal branches of the brachial plexus in the axillary region. (1) Axillary nerve, (2) musculocutaneous nerve, (3) radial nerve, (4) median nerve, (5) medial antebrachial cutaneous nerve, (6) ulnar nerve, (7) medial brachial cutaneous nerve (With permission from Danilo Jankovic)
The nerves are distributed around the axillary artery, together with one or more accompanying axillary veins, and together they constitute the neurovascular bundle (Fig. 32.3). The median nerve is most commonly located in the anterolateral quadrant, the ulnar nerve in the anteromedial quadrant, and the radial nerve in the posteromedial quadrant around the artery (Fig. 32.4). However, these nerves are highly mobile, and on ultrasound, their position can be observed to vary significantly with the pressure exerted through the probe. The musculocutaneous nerve starts in a location adjacent to the median nerve in the posterolateral quadrant around the artery but then courses out laterally in the fascial plane between biceps and coracobrachialis muscle. Its exact location in any given subject is highly variable and depends on how proximally or distally it takes off from the lateral cord; this is the main reason for the high failure rate with single-injection landmark-guided approaches [1].
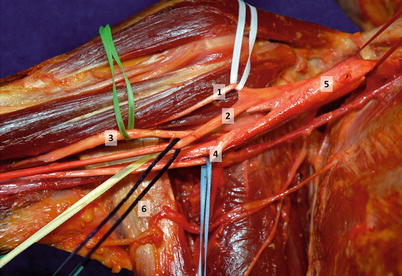
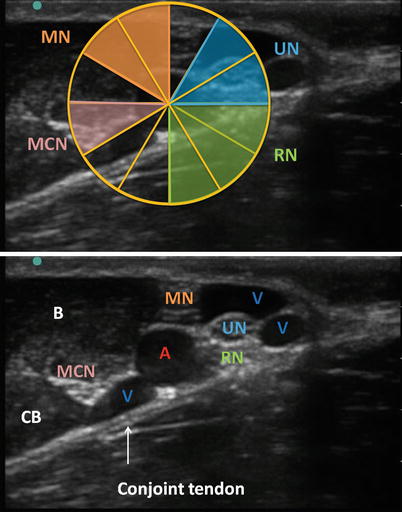
Fig. 32.3
Cadaveric dissection of the axillary brachial plexus. The musculocutaneous nerve (1) (white) and median nerve (2) (dark blue) originate from the lateral cord. The radial nerve (3) (green) and ulnar nerve (4) (light blue) run posterior and medial to the axillary artery (5) but have been displaced here for visibility. Note the conjoint tendon (6) of teres major and latissimus dorsi which inserts onto the humerus posterior to the axillary neurovascular bundle (With permission from Danilo Jankovic)
Fig. 32.4
Typical ultrasound image of the axillary brachial plexus. The pulsatile axillary artery (A) is usually accompanied by more than one vein (V). All the vessels and nerves lie on the hyperechoic conjoint tendon. The most common location of the median nerve (MN), ulnar nerve (UN), radial nerve (RN), and musculocutaneous nerve (MCN) in relation to the artery is illustrated in the top image. The musculocutaneous nerve often lies in the fascial plane between biceps (B) and coracobrachialis (CB) (Image courtesy of KJ Chin MPC)
A fascial sheath surrounds the brachial plexus in this location but is subdivided by thinner septa into compartments that contain the median, ulnar, and radial nerves. These are most evident during ultrasound-guided perineural block. While large-volume injection in a single location close to the artery may traverse these septa, they are nevertheless likely to be another reason for the poor efficacy of the single-injection landmark-guided techniques [1].
The most important landmark in the ultrasound-guided approach, apart from the axillary artery, is the conjoint tendon of teres major and latissimus dorsi (Figs. 32.3 and 32.4). This inserts onto the proximal humerus and forms a “floor” on which the artery and all the associated nerves lie [3]. In particular the radial nerve can always be visualized lying superficial to the conjoint tendon on ultrasound. Distal to the lateral edge of the conjoint tendon, the radial nerve rapidly courses posteriorly and away from the axillary artery, descending between the heads of the triceps muscle to lie in the spiral groove of the humerus. Ultrasound-guided axillary nerve blocks performed where the conjoint tendon cannot be visualized therefore carry a significant risk of failure to block the radial nerve.
Technique: Surface Landmark-Guided Approach, Single-Shot
Required Supplies and Equipment
Disinfectant solution and swabs for skin preparation
Sterile gloves and drapes
Short-beveled 22-G, 50-mm block needle with extension tubing
Note that a sharp hypodermic needle may be preferred in the transarterial approach.
Local anesthetic of choice in 10- or 20-ml syringes
Peripheral nerve stimulator (optional, depending on approach)
Lidocaine 1–2 % in 3-ml syringe with a 25–27-G hypodermic needle for skin infiltration (at operator’s discretion)
Equipment and supplies for managing life-threatening acute complications, including Intralipid for local anesthetic systemic toxicity
Drugs for intravenous sedation during the block (at operator’s discretion)
Preparation of Patient
Obtain informed consent for the block.
Explain expected clinical course including care of the insensate limb and managing the transition to systemic analgesia.
Establish intravenous access, supplemental oxygen delivery, and standard monitors (ECG, noninvasive blood pressure, pulse oximetry)
Perform a time-out to confirm patient identity and site and side of surgery.
Block Performance
Patient Position
The patient is placed supine with the arm externally rotated and abducted to 90° at the shoulder, with the elbow flexed (Fig. 32.5). Abduction beyond 90° should be avoided, as it makes arterial palpation more difficult and may impair distribution of the local anesthetic.

Fig. 32.5
Patient positioning for the axillary block. The patient is supine with the arm externally rotated and abducted to 90° at the shoulder. The shoulder should not be abducted more than 90°, as it makes arterial palpation more difficult, distorts the ultrasonographic view, and may impair distribution of the local anesthetic [8] (With permission from Danilo Jankovic)
The operator stands on the side of the patient to be blocked.
Surface Landmarks
The axillary artery is palpated as proximally as possible under the lateral edge of the pectoralis major muscle (Fig. 32.6). This increases the efficacy of the block for two reasons: (1) there is a higher likelihood that the musculocutaneous nerve will be close enough to the plexus for local anesthetic spread to reach it; (2) the plexus is targeted where it lies on the conjoint tendon, which is an important boundary for containing and directing local anesthetic spread, especially around the radial nerve.
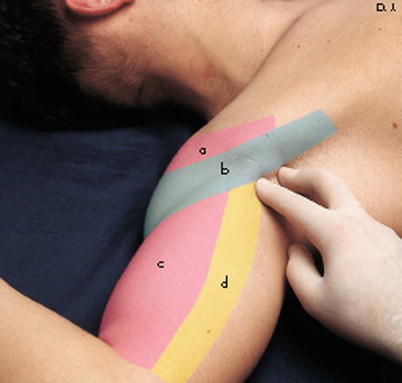
Fig. 32.6
Palpation of the axillary artery. This is done with two fingers (usually the 2nd and 3rd fingers), so that the skin and artery may be fixed in position between them. Palpation should be performed as proximal as possible (a deltoid muscle, b pectoralis major muscle, c biceps muscle, d coracobrachialis muscle) (With permission from Danilo Jankovic)
The median nerve is expected to lie superior and anterior (superficial) to the artery, the ulnar nerve lies inferior and posterior, and the radial nerve lies posterior (deep) to the artery.
Needle Insertion and Injection Technique
A variety of methods of nerve localization have been described, including the elicitation of paresthesia and seeking a fascial click to indicate entry into the fascial sheath [4, 5]. These are primarily of historical interest and will not be described further here. The two methods that will be described are:
1.
Transarterial double-injection technique
Get Clinical Tree app for offline access

Disinfect the skin, drape the area appropriately, and prime the block needle and tubing with local anesthetic solution.
Place the 2nd and 3rd fingers of the nondominant hand on either side of the artery to anchor it in position.
Advance the block needle at a 90° angle to the skin to puncture the artery, as evidenced by pulsatile backflow of bright-red blood into the tubing (Fig. 32.7).
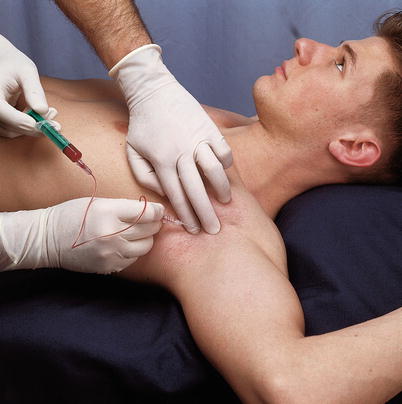
Fig. 32.7
Performance of the transarterial axillary block. The artery is fixed firmly between the fingers of the nondominant hand. The operator advances the block needle, while an assistant aspirates to confirm that the artery has been pierced. The needle is advanced further until blood can no longer be aspirated, signaling that the needle tip is now posterior to the artery. Half the volume of local anesthetic is injected in this location (in fractionated doses). The needle tip is withdrawn; blood is again aspirated as the needle tip reenters the arterial lumen and ceases as the tip exits the lumen to lie anterior to the artery, at which time the remaining half of local anesthetic is injected (again in fractionated doses) (With permission from Danilo Jankovic)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree







