Obese patients become hypoxic rapidly and can tolerate only brief periods of apnea, such as that associated with airway manipulation.
The metabolic activity of fat and supportive tissues increases oxygen consumption and carbon dioxide (CO2) production in obese patients. This is compensated for with increased minute ventilation and cardiac output. Due to the aforementioned mechanical limitations, patients may be unable to increase tidal volume at times of increased oxygen need and must rely on tachypnea to improve minute ventilation.
Obstructive sleep apnea (OSA), characterized by recurrent episodes of upper airway obstruction during sleep, occurs in up to 70% of morbidly obese patients undergoing bariatric surgery and is a risk factor for adverse perioperative outcomes. Airway obstruction occurs due to growth of adipose tissue in oral and pharyngeal structures. Obesity hypoventilation syndrome (OHS) or Pickwickian syndrome is seen in 5% to 10% of patients with OSA, characterized by daytime hypercapnia and hypoventilation and sleep disordered breathing. Patients with OHS are at increased risk for sedative- and opioid-related ventilatory impairment because of upper airway obstruction, depressed central respiratory drive, and impaired lung mechanics. Over the long term, OSA and OHS lead to polycythemia, systemic and pulmonary hypertension, left ventricular hypertrophy, cardiac dysrhythmias, right heart strain, and cor pulmonale (Fig. 28-1).
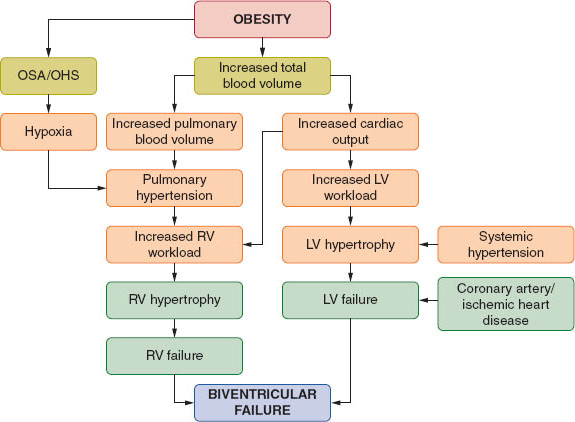
FIGURE 28-1 Interrelationship of cardiovascular and pulmonary sequelae of obesity. OSA, obstructive sleep apnea; OHS, obesity hypoventilation syndrome; LV, left ventricular; RV, right ventricular. (From Bucklin BA, Fernandez-Bustamante A. Anesthesia and obesity. In: Barash PG, Cullen BF, Stoelting RK, et al. Clinical Anesthesia, 7th ed. Philadelphia: Lippincott Williams & Wilkins, 2013:1278.)
 VIDEO 28-1
VIDEO 28-1
Sequelae of Obesity
Cardiovascular System
Obesity is associated with an increase in blood volume, although the weight-based blood volume is reduced (from 70 mL/kg in lean individuals to 50 mL/kg in obese patients). As noted, obese patients are at higher risk for hypertension, left ventricular hypertrophy, diastolic dysfunction, and heart failure. The combination of dyslipidemia, diabetes, and hypertension predisposes obese patients to atherosclerosis and hence coronary and cerebrovascular disease. Obesity also predisposes to a hypercoagulable state because of increased levels of procoagulant factors and decreased fibrinolysis.
Gastrointestinal System
Aspiration risk associated with obesity is discussed later. Obesity-associated liver disease includes fatty infiltration (nonalcoholic fatty liver disease), inflammation (nonalcoholic steatohepatitis), focal necrosis, and cirrhosis. Obese patients are also at risk for cholelithiasis, particularly after intestinal bypass surgery.
Endocrine and Metabolic Systems
Obese patients often exhibit metabolic syndrome, which is a combination of risk factors (abdominal obesity, hypertension, dyslipidemia, and insulin resistance or impaired glucose tolerance). This increases their risk for cardiovascular-related morbidity and mortality, type 2 diabetes, polycystic ovary syndrome, nonalcoholic fatty liver disease, cholelithiasis, and a proinflammatory state.
B. Pharmacologic Principles
Drug dosing in obesity is affected by multiple factors, including increased total body fat, reduced total body water, altered protein binding, increased blood volume and cardiac output, increased lipid concentrations in blood, organomegaly, enhanced phase II reactions (glucuronidation and sulfation), and drug absorption in fat stores.
Drugs that are mainly distributed to lean tissues (e.g., nondepolarizing neuromuscular blocking agents) should be dosed based on the lean body weight (LBW α ideal body weight [IBW] × 1.2). Although initial doses for lipophilic drugs (e.g., benzodiazepines, barbiturates) have to be based on LBW as well, maintenance doses should be based on total body weight (TBW) because of the significantly increased volume of distribution. Multiple doses of lipophilic drugs lead to accumulation in fat stores, causing a prolonged response as the drug is released back into circulation.
In morbidly obese patients, it is more appropriate to use LBW rather than TBW for induction of general anesthesia with propofol. Studies have shown that dosing based on LBW in morbidly obese patients resulted in similar doses and similar times to loss of consciousness when compared to nonobese control patients with dosing based on TBW. However, TBW-based dosing accurately predicted the volume and clearance of propofol, suggesting the use of TBW as the dosing scalar when administering maintenance infusions of propofol.
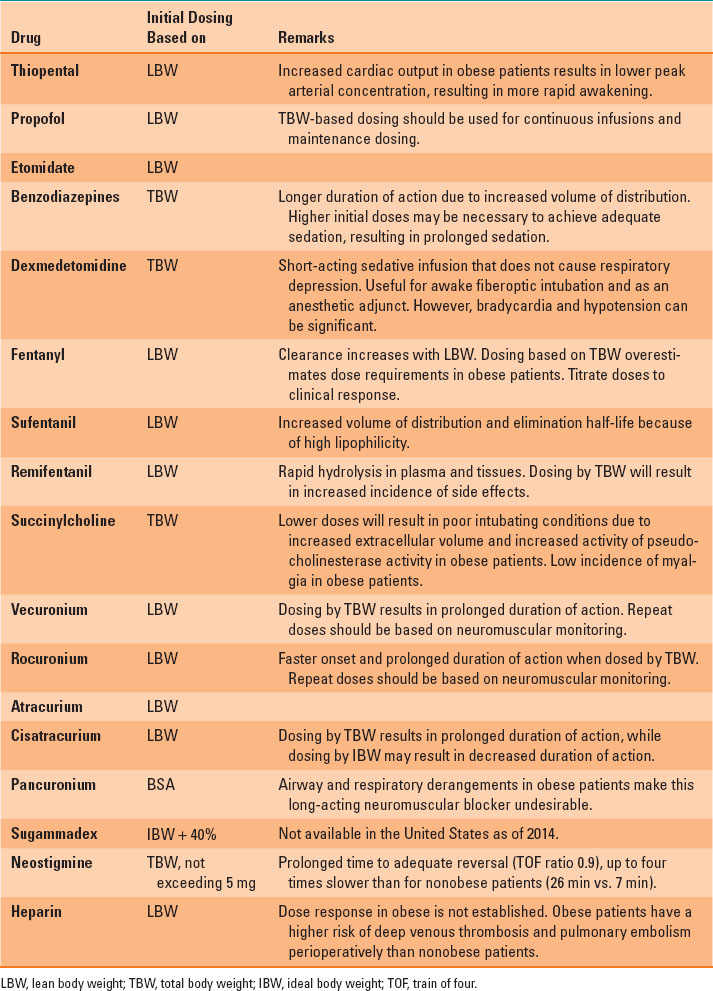
The principles for administration of commonly used perioperative drugs in obese patients are listed in Table 28-1. It must be noted that the dose–response relationships for most drugs in obese patients have not been completely elucidated. For inhaled anesthetics, the longer time constants for equilibrium with fat along with poor perfusion of fat tissue counteract the effect of increased fat mass on uptake. As a result, obesity does not influence induction times and only modestly affects the wake-up time with the inhaled anesthetics in routine clinical practice, especially in surgeries lasting <4 hours.
Table 28-1 Principles for Administration of Common Perioperative Drugs in Obese Patients
C. Preoperative Evaluation
Preoperative evaluation should include assessment of the risk of airway management difficulties, vascular access options, identification of relevant comorbidities, and education of the patient regarding the perioperative anesthetic plan.
There is a high prevalence of difficult airways in obese patients due to a large tongue, perimandibular and nuchal fat tissue, and redundant pharyngeal soft tissue. OSA independently correlates with difficult mask ventilation. Difficult intubation rates in obese patients range from 5% to 15% and up to 21% in patients with OSA. Male sex, neck circumference, and Mallampati score have been shown to predict difficult intubation in obese patients, although these results are inconsistent across multiple studies and the positive predictive value for such factors is low. Laryngoscopic view is improved in morbidly obese patients with the use of a video laryngoscope. The ramped position, as described later, also improves laryngoscopic view.
Preoperative evaluation for OSA and initiation of continuous positive airway pressure (CPAP) at home is recommended. In the absence of a formal preoperative sleep study, tools like the STOP-BANG questionnaire help identify patients with OSA. The questionnaire consists of questions on Snoring, Tiredness, Observed apnea, high blood Pressure, BMI >35, Age >50, Neck circumference >40 cm, and male Gender, with positive answers to three or more questions suggesting a higher risk for OSA.
Preoperative assessment of obese patients should include an evaluation of common comorbidities (systemic or pulmonary hypertension, diabetes, OSA, ischemic heart disease, heart failure). Preoperative medical management of the comorbidities, when possible, may help reduce the perioperative risk. Patients with OSA should be educated about the use of perioperative CPAP.
D. Intraoperative Considerations
Equipment and Positioning
Whenever possible, patients should position themselves on the operating table. In extreme cases, a mechanical lifting device may be required to move the patient. Although most operating room tables are capable of handling moderately obese patients, specially designed tables are required for surgery in the extremely obese. Well-padded sleds or arm boards are often required to position the arms. For surgeries that require tilting or turning of the table, strapping or taping the patient to the table along with stiffened “bean bags” can prevent accidental falls. Gel and foam pads should be used to support pressure points and prevent peripheral neuropathy and skin breakdown. The supine position is associated with reduction in lung volumes and hypoxemia, and venous return may be impeded through caval compression. In the prone position, emphasis should be placed on free abdominal wall movement, with support for the chest wall and the pelvis. Shoulder bars may cause injury to the brachial plexus if incorrectly placed. The Trendelenburg position causes the highest degree of respiratory compromise with a decrease in FRC and lung compliance. Lateral positioning and the sitting position allow the weight of the abdominal fat to fall away from the chest and diaphragm (Fig. 28-2).
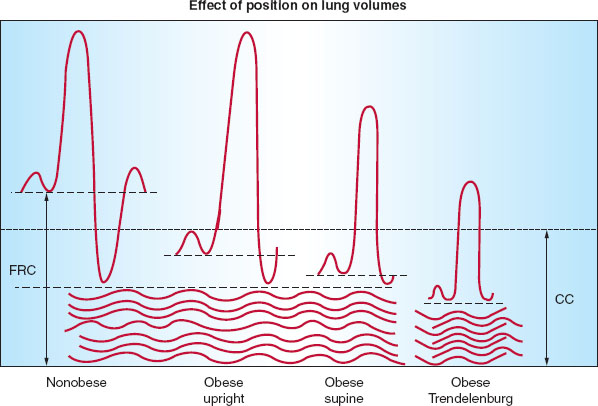
FIGURE 28-2 Effects of obesity, positioning, and anesthesia on lung volumes. FRC, functional residual capacity; CC, closing capacity; CV, closing volume; RV, residual volume. (From Bucklin BA, Fernandez-Bustamante A. Anesthesia and obesity. In: Barash PG, Cullen BF, Stoelting RK, et al. Clinical Anesthesia, 7th ed. Philadelphia: Lippincott Williams & Wilkins, 2013:1277.)
Monitoring and Vascular Access
Noninvasive monitoring of blood pressure overestimates the blood pressure in a large proportion of obese patients because of inappropriate cuff size and the conical shape of the arm. Also, recording times may be prolonged, leading to delayed recognition of a change in blood pressure. Although the use of the forearm for blood pressure measurement may be adequate, use of invasive monitoring should be considered, especially in the presence of comorbid conditions. Peripheral venous access can also be challenging and may require ultrasound guidance.
Airway Management
In order to reduce the incidence and impact of aspiration, antacids, prokinetics, H2 receptor antagonists or proton-pump inhibitors should be administered prior to induction in patients with an identifiable risk of aspiration (discussed later). Although cricoid pressure is reasonable, the risk of aspiration should be weighed against the risk of worsened view during laryngoscopy.

The best position for inducing anesthesia in obese patients is a semisitting position using a ramp to place the patient’s ears at the level of the anterior chest wall.
With induction of anesthesia in the supine position, obese patients experience a further reduction of FRC, and oxygen saturation may fall rapidly. Maneuvers that prolong safe apnea times during induction include preoxygenation with 100% oxygen, use of a 25- to 30-degree reverse Trendelenburg or semisitting beach-chair position, application of 10 cm H2O CPAP during preoxygenation, and positive end-expiratory pressure (PEEP) during mask ventilation. The head-up position also minimizes the risk of passive regurgitation.
Placing the obese patient in a ramped position can be beneficial for laryngoscopy and intubation. It can be achieved with towels or folded blankets under the patient’s shoulders and head or with a commercially available device. The head, shoulders, and upper body are elevated above the chest, with the goal of elevating the external auditory meatus to the level of the anterior chest wall (Fig. 28-3).
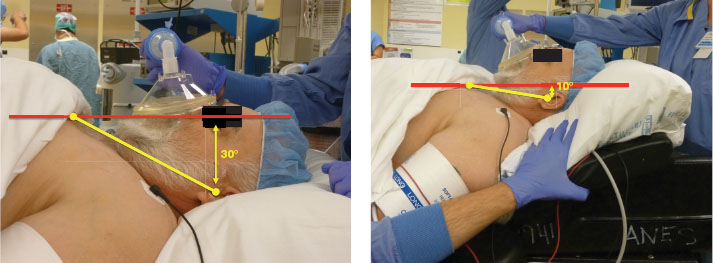
FIGURE 28-3 Positioning of an obese patient supine on the operating table with use of an upper body (shoulder/head) “ramp” will likely enhance laryngoscopic view of the vocal cords and facilitate tracheal intubation. The goal of such positioning is to bring a line drawn between the external auditory meatus and the sternal notch (yellow line) into a position parallel to the horizontal plane (red line). Standard supine positioning (left) demonstrates a 30° difference between these two lines, whereas proper ramp positioning (right) has reduced this angle to only 10°.
Mechanical Ventilation
There is no clear evidence of the benefit of volume- versus pressure-controlled ventilation in obese patients. Tidal volumes of 6 to 8 mL/kg IBW with sufficient PEEP are recommended for intraoperative ventilation. Alveolar recruitment maneuvers and subsequent application of moderate PEEP (10 cm H2O) helps prevent atelectasis, particularly in patients undergoing laparoscopic surgery. Reduced ventilatory compliance can cause high airway pressures, making it difficult to maintain plateau pressures <30, especially with pneumoperitoneum during laparoscopic surgeries. High airway pressures can cause barotrauma and hypotension. Hypercapnia might have to be tolerated. However, hypercapnia can result in a further increase of pulmonary vascular resistance in patients with pre-existing pulmonary hypertension.
Fluid Management
Obese patients may suffer increased perioperative blood loss because of technical difficulties with surgical exposure. It can also be difficult to estimate fluid balance, adequacy of peripheral perfusion, and blood loss. Measurement of urine output, venous pressures, and acid–base balance may be indicated.
Emergence
Precautions similar to induction should be observed. Patients should be extubated when neuromuscular blockade has been completely reversed (ideally assessed quantitatively) and the patient is awake and positioned in a semisitting or reverse Trendelenburg position, with CPAP maintained to prevent alveolar derecruitment. Postoperative lung function is improved with application of CPAP immediately after extubation.
Monitored Anesthesia Care and Sedation
Procedural sedation of the obese patient is not to be taken lightly. There should be close monitoring of respiratory function because of pre-existing respiratory compromise, increased risk of respiratory depression with sedation, and the potential for difficult mask ventilation and intubation. The presence of OSA increases the risk of perioperative hypoxemia and the requirement of airway interventions during sedation. Dexmedetomidine is a selective α2-adrenergic agonist that provides sedation without respiratory depression. However, its clinical use can be limited because of hemodynamic instability.
E. Regional Anesthesia
The 2006 American Society of Anesthesiologists’ (ASA) practice guidelines for management of patients with OSA recommend that regional analgesic techniques be considered to reduce or eliminate the requirement for systemic opioids. However, excessive sedation used to perform or manage the regional anesthetic may negate the advantages.
Neuraxial Techniques
Spinal or epidural placement in the sitting position allows for easier identification of the vertebral midline. Ultrasound can be used to identify the spinous processes and to reduce the number of needle passes. When longer needles are used, a careful assessment of the midline will avoid injury. Epidural placement can be challenging because of the loss of resistance felt in fat planes and difficulties in predicting the depth of the epidural space. There is a higher initial failure rate for epidural catheters in obese laboring patients than in lean patients.

When placing a spinal or epidural needle in the obese patient, it is best done with the patient sitting up.
During spinal anesthesia, local anesthetics and opioids can have an exaggerated cephalad spread because of (a) decreased cerebrospinal fluid volume due to fatty tissue spread into the intervertebral foramina and engorged epidural veins (due to elevated venous pressures) and (b) head-down positioning of the vertebral column due to large buttocks. A ramp under the chest elevates the cervical and thoracic spine, limiting cephalad spread of hyperbaric local anesthetic.
Peripheral Nerve Blocks
Local anesthetic dosing for peripheral nerve blocks in obese patients should be based on IBW, rather than TBW, to avoid systemic toxicity. Obese patients suffer a higher rate of block failure than nonobese patients, particularly with epidural, paravertebral, continuous supraclavicular, and superficial cervical blocks. Although the use of ultrasound may improve the success rate and reduce procedure time, ultrasound imaging in obese patients can be suboptimal due to an increased number of reflective surfaces and greater depth to the structures. Retraction and taping of the excessive soft tissue away from the procedural site allow for sterile preparation and easier access to insertion sites.
F. Anesthesia for Bariatric Surgery
Surgical treatment of obesity is generally considered if BMI is >40 kg/m2 (or BMI >35 kg/m2
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


