Kyle E. Johnson
I. Vascular Disease: Epidemiologic, Medical, and Surgical Aspects
The incidence of atherosclerosis and vascular disease increases with advancing age. Therefore, it can be expected that there will be higher demand for vascular procedures, especially novel techniques such as angioplasty and endovascular stent placement. In addition, vascular surgery patients are some of the most complex patients to manage in the perioperative period. This chapter will focus on the principles of that management.
A. Pathophysiology of Atherosclerosis
Atherosclerosis describes a multifactorial inflammatory disease of the vascular tree. Predisposing risk factors for atherosclerosis include hypertension, dyslipidemia, abdominal obesity, insulin resistance, cigarette smoking, increasing age, family history, proinflammatory states, and prothrombotic states. The development of atherosclerosis occurs in two stages: endothelial injury and inflammatory response to injury. The primary injury occurs as low-density lipoprotein and apolipoprotein-B–containing lipoproteins invade the vascular endothelium and become proinflammatory. As the inflammatory cascade ensues, the subendothelial space is filled with atherogenic lipoproteins and macrophages, which form foam cells. Foam cells form the atheromatous core of a plaque, which becomes necrotic and further enhances the inflammatory process. Disruption of the fibrous cap over a lipid deposit can lead to plaque rupture and ulceration. Vascular disease is not a localized phenomenon, but rather a systemic one affecting multiple organs including the heart with myocardial infarction (MI) and the brain with cerebrovascular accidents (CVA).
B. Natural History of Patients with Peripheral Vascular Disease
More than 25 million people in the United States have clinical manifestations of atherosclerotic vascular disease (Fig. 36-1). For example, 43% of men and 34% of women older than 65 years of age have >25% carotid stenosis, and stroke remains the leading cause of disability and the third leading cause of death in the United States. Peripheral arterial disease (PAD) can cause claudication and limb ischemia (2% prevalence in aging individuals). Aortic atherosclerotic disease can lead to abdominal aortic aneurysm (AAA), aortic dissection, peripheral atheroembolism, penetrating aortic ulcer, and intramural hematoma. Coronary atherosclerosis that leads to MI is the leading cause of death and disability worldwide.

Approximately 30 to 40 million people in the United States have peripheral arterial disease.
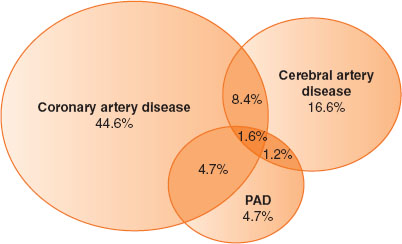
FIGURE 36-1 Typical overlap in vascular disease affecting different territories. Based on REACH data. PAD, peripheral arterial disease. (From Smaka TJ, Miller TE, Hutchens MP, et al. Anesthesia for vascular surgery. In: Barash PG, Cullen BF, Stoelting RK, et al. Clinical Anesthesia, 7th ed. Philadelphia: Lippincott Williams & Wilkins, 2013:1114.)
C. Medical Therapy for Atherosclerosis
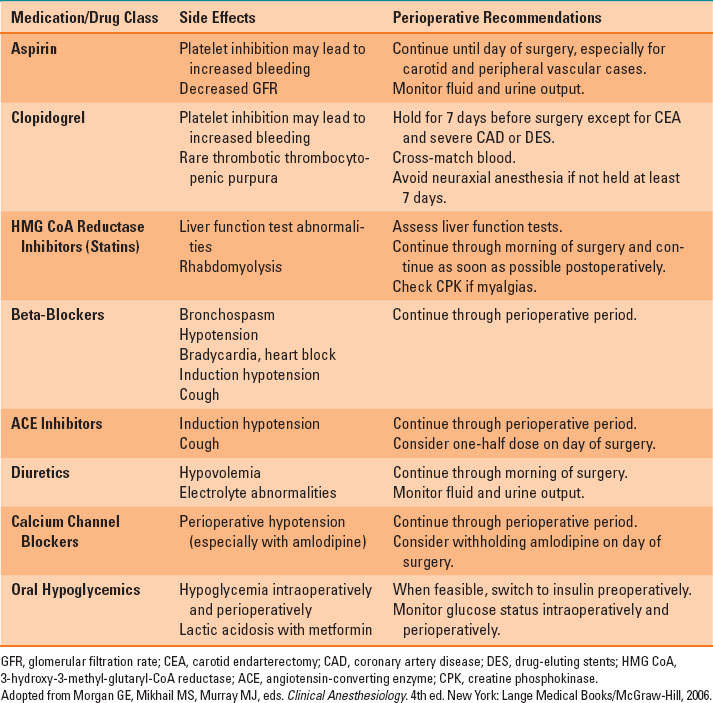
Management of contributing systemic diseases such as hypertension (using antihypertensives such as beta-blockers), hyperlipidemia (using statins or other lipid-lowering agents), diabetes (using oral hypoglycemic agents or insulin therapy), and obesity (through exercise, weight loss, and diet) may significantly retard the progression of atherosclerosis and may reduce perioperative morbidity and mortality after vascular surgery. Treatment with statin drugs reduces progression and may cause regression of atherosclerotic plaques, improve endothelial function, and reduce cardiovascular events. Chronic therapy with aspirin, angiotensin-converting enzyme inhibitors, and especially smoking cessation have all been shown to significantly slow or reverse the progression of atherosclerosis. Most medical therapies, including statins, aspirin, and beta-blockers, should be continued up to and throughout the perioperative period to reduce the risk of perioperative cardiovascular events (Table 36-1).
Table 36-1 Medical Therapy, Side Effects, and Current Recommendations
II. Chronic Medical Problems and Management in Vascular Surgery Patients
The patient undergoing vascular surgery likely has systemic vascular disease complicated by medical problems such as coronary artery disease, systemic hypertension, hyperlipidemia, diabetes, obesity, and tobacco abuse.

As many as 25% of adults presenting for vascular surgery have severe coronary artery disease.
A. Coronary Artery Disease in Patients with Peripheral Vascular Disease
As many as 25% of patients presenting for vascular surgery have severe coronary artery disease (CAD). The American Heart Association and others have published guidelines for cardiac evaluation and management prior to noncardiac surgery (Fig. 36-2) (1).
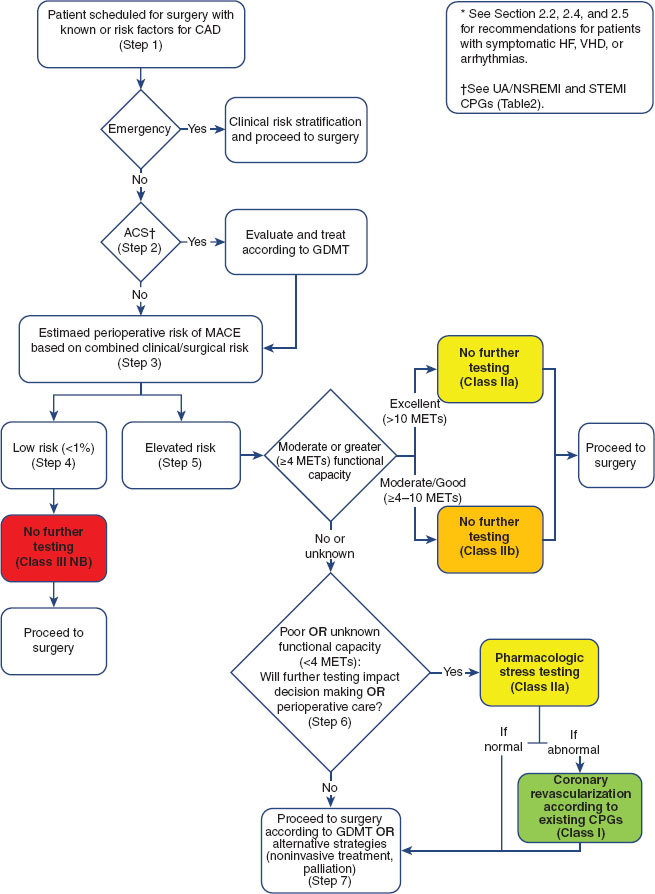
FIGURE 36-2 Stepwise Approach to Perioperative Cardiac Assessment for Coronary Artery Disease. The American College of Cardiology/American Heart Association (ACC /AHA) guideline calls for stepwise cardiac risk assessment involving consideration of the patient’s cardiac risk factors, functional capacity, and the planned surgical procedure. See Figure 16-1 and accompanying legend for details. (From Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am CollCardiol. 2014;():. doi:10.1016/j.jacc.2014.07.944. Available at http://content.onlinejacc.org/article.aspx?articleid=1893784. Page 30 of 105)
B. Preoperative Coronary Revascularization
The Coronary Artery Revascularization Prophylaxis trial randomized patients with coronary disease before elective vascular surgery to either coronary revascularization or medical therapy and found no benefit to coronary revascularization if aggressive medical therapy (including beta-blockers, aspirin, and statins) was instituted. Revascularization may therefore be of minimal value in preventing coronary events after vascular surgery, except in patients in whom revascularization is indicated for acute coronary syndrome. If a coronary stent is placed, elective surgery should be delayed: for bare metal stents, a minimum of 6 weeks of dual antiplatelet therapy (DAPT); and for drug-eluting stents, 12 months (or longer) of DAPT (2). Aspirin is recommended indefinitely to prevent in-stent thrombosis. With the advent of new stents, the time required for DAPT and delay of surgery will likely evolve.
III. Other Medical Problems in Vascular Surgery Patients
In addition to known common comorbid conditions such as CAD, systemic hypertension, hyperlipidemia, diabetes, obesity, and tobacco abuse, the vascular patient may have other undiagnosed conditions including hypercoagulable states, renal insufficiency, heart failure, chronic obstructive pulmonary disease, sleep apnea and others. If surgery is elective, preoperative management should focus on optimizing all the patient’s chronic conditions, a process that cannot be accomplished if the patient presents on the morning of surgery.
IV. Organ Protection in Vascular Surgery
Many vascular procedures involve the occlusion of blood flow through the application of clamps, shunts (providing flow at a lower perfusion pressure), or bypasses (directing flow from a well perfused region to a poorly perfused region). Therefore, vital organs may suffer ischemia for varying durations.
 VIDEO 36-1
VIDEO 36-1
Carotid Shunting
A. Ischemia-Reperfusion Injury in the Vascular Surgery Patient: Fundamental Concepts
Reduction or interruption of blood flow (ischemia) compromises delivery of oxygen, glucose, and other essential nutrients for aerobic metabolism and thus slows the generation of adenosine triphosphate. When adenosine triphosphate is fully depleted, cellular processes fail and cellular integrity is lost (ischemic injury). The duration of ischemia correlates directly with the degree of cellular injury. In addition, toxic metabolites of anaerobic metabolism accumulate in the low or no-flow regions during the ischemic period. Upon restoration of flow and resumption of delivery of nutrients, further damage occurs via generation of toxic oxygen species, release of cytotoxic amino acids, up-regulation of nitric oxide synthase, and initiation of cellular apoptosis. In addition, toxic by-products of anaerobic metabolism are released into the systemic circulation, causing electrolyte abnormalities, labile blood pressures, alterations in systemic vascular resistance, and potentially severe acid-base disequilibrium.
B. Prevention of Myocardial Injury
Vascular surgery can result in dramatic changes in blood pressure, especially during procedures requiring aortic clamping. (See Chapter 35 for further discussion of myocardial oxygen supply and demand as well as techniques for monitoring and treating myocardial ischemia.)
C. Prevention of Kidney Injury
Postoperative acute renal failure (ARF)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


