Ultrasound-Guided Obturator Nerve Block
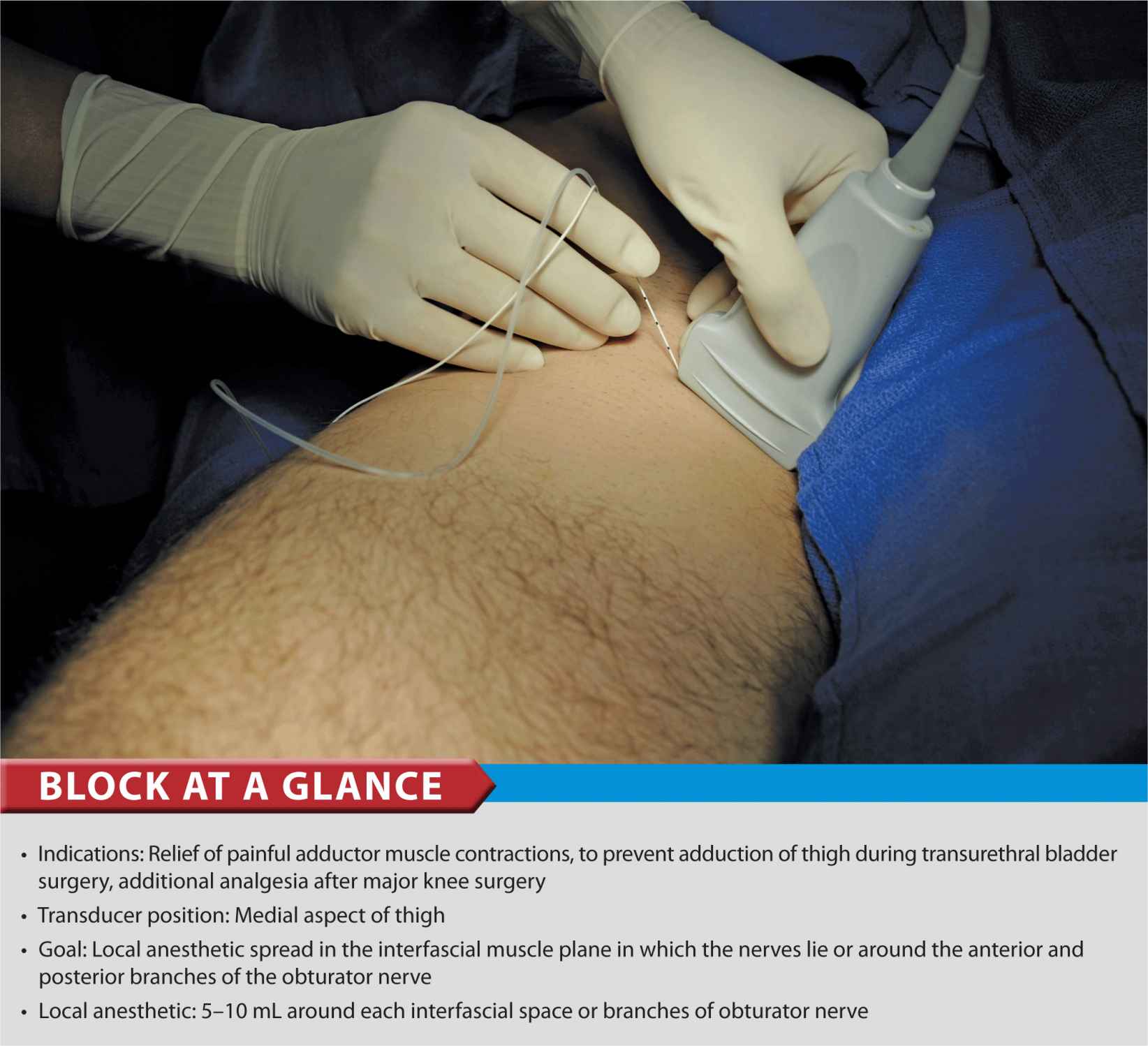
FIGURE 37-1. Needle insertion using an in-plane technique to accomplish an obturator nerve block.
General Considerations
There is renewed interest in obturator nerve block because of the recognition that the obturator nerve is spared after a “3-in-1 block” and yet can be easier accomplished using ultrasound guidance. In some patients, the quality of postoperative analgesia is improved after knee surgery when an obturator nerve block is added to a femoral nerve block. However, a routine use of the obturator block does not result in improved analgesia in all patients having knee surgery. For this reason, obturator block is used selectively.
Ultrasound-guided obturator nerve block is simpler to perform, more reliable, and associated with patient discomfort when compared with surface landmark-based techniques.
There are two approaches to performing ultrasound-guided obturator nerve block. The interfascial injection technique relies on injecting local anesthetic solution into the fascial planes that contain the branches of the obturator nerve. With this technique, it is not important to identify the branches of obturator nerve on the sonogram but rather to identify the adductor muscles and the fascial boundaries within which the nerves lie. This is similar in concept to other fascial plane blocks (e.g. transversus abdominis plane block [TAP]) where local anesthetic solution is injected between the internal oblique and transverse abdominis muscles without the need to indentify the nerves. Alternatively, the branches of the obturator nerve can be visualized with ultrasound imaging and blocked after eliciting a motor response.
Anatomy
The obturator nerve forms in the lumbar plexus from the anterior primary rami of L2-L4 roots and descends to the pelvis in the psoas muscle. In most individuals, the nerve divides into an anterior branch and posterior branch before exiting the pelvis through the obturator foramen. In the thigh, at the level of the femoral crease, the anterior branch is located between the fascia of pectineus and adductor brevis muscles. The anterior branch lies further caudad between the pectineus and adductor brevis muscles. The anterior branch provides motor fibers to the adductor muscles and cutaneous branches to the medial aspect of the thigh. The anterior branch has a great variability in the extent of sensory innervation of the medial thigh. The posterior branch lies between the fascial planes of the adductor brevis and adductor magnus muscles (Figures 37-2 and 37-3). The posterior branch is primarily a motor nerve for the adductors of the thigh; however it also may provide articular branches to the medial aspect of the knee joint. The articular branches to the hip joint usually arise from the obturator nerve proximal to its division and only occasionally from the individual branches (Figure 37-4).
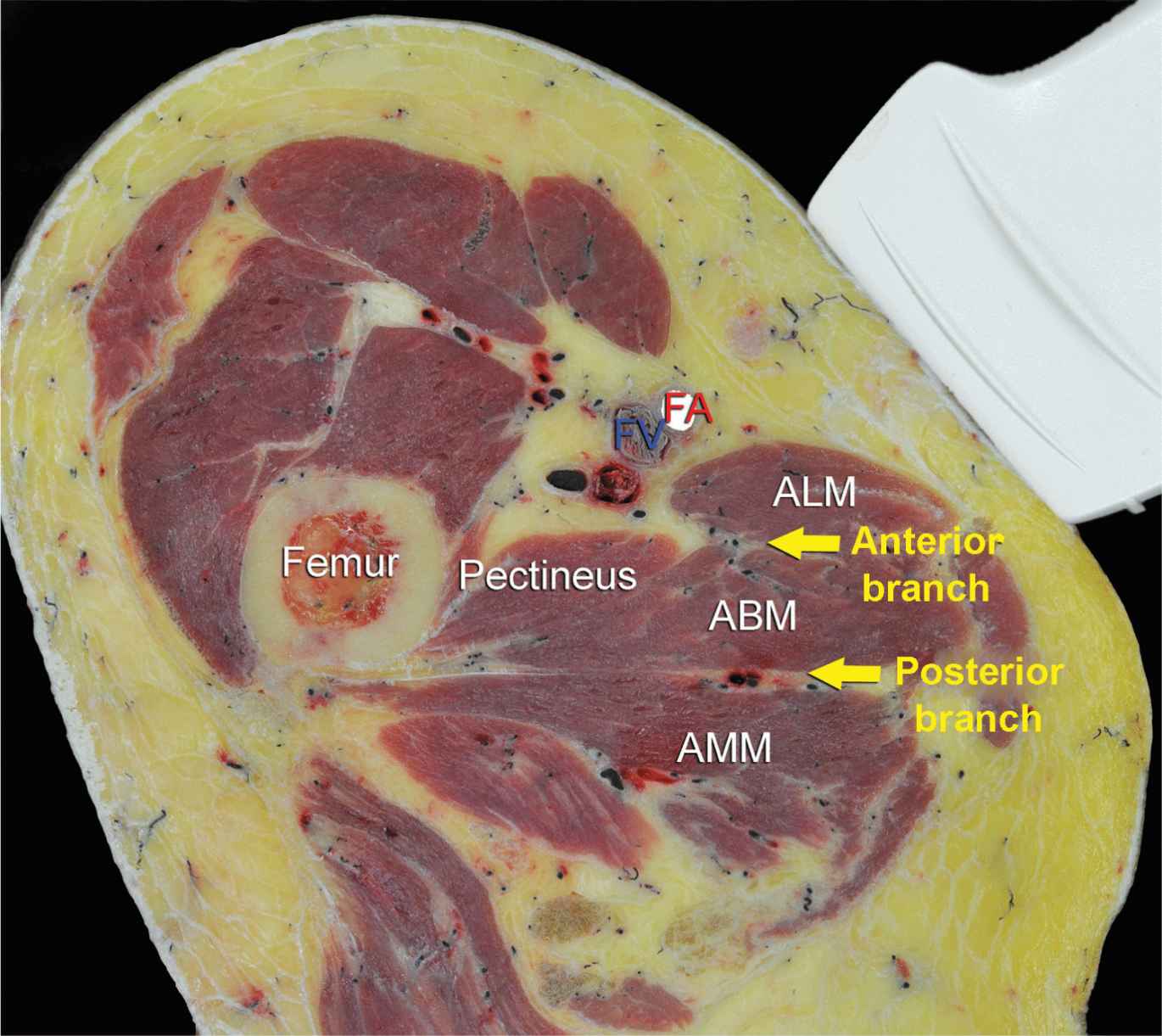
FIGURE 37-2. Cross-sectional anatomy of relevance to the obturator nerve block. Shown are femoral vessels (FV, FA), pectineus muscle, adductor longus (ALM), adductor brevis (ABM), and adductor magnus (AMM) muscles. The anterior branch of the obturator nerve is seen between ALM and ABM, whereas the posterior branch is seen between ABM and AMM.
FIGURE 37-3. Anterior branch (Ant. Br.) of the obturator nerve (ObN) is seen between the adductor longus (ALM) and the adductor brevis (ABM), whereas the posterior branch (Post. Br.) is seen between the ABM and the adductor magnus (AMM).
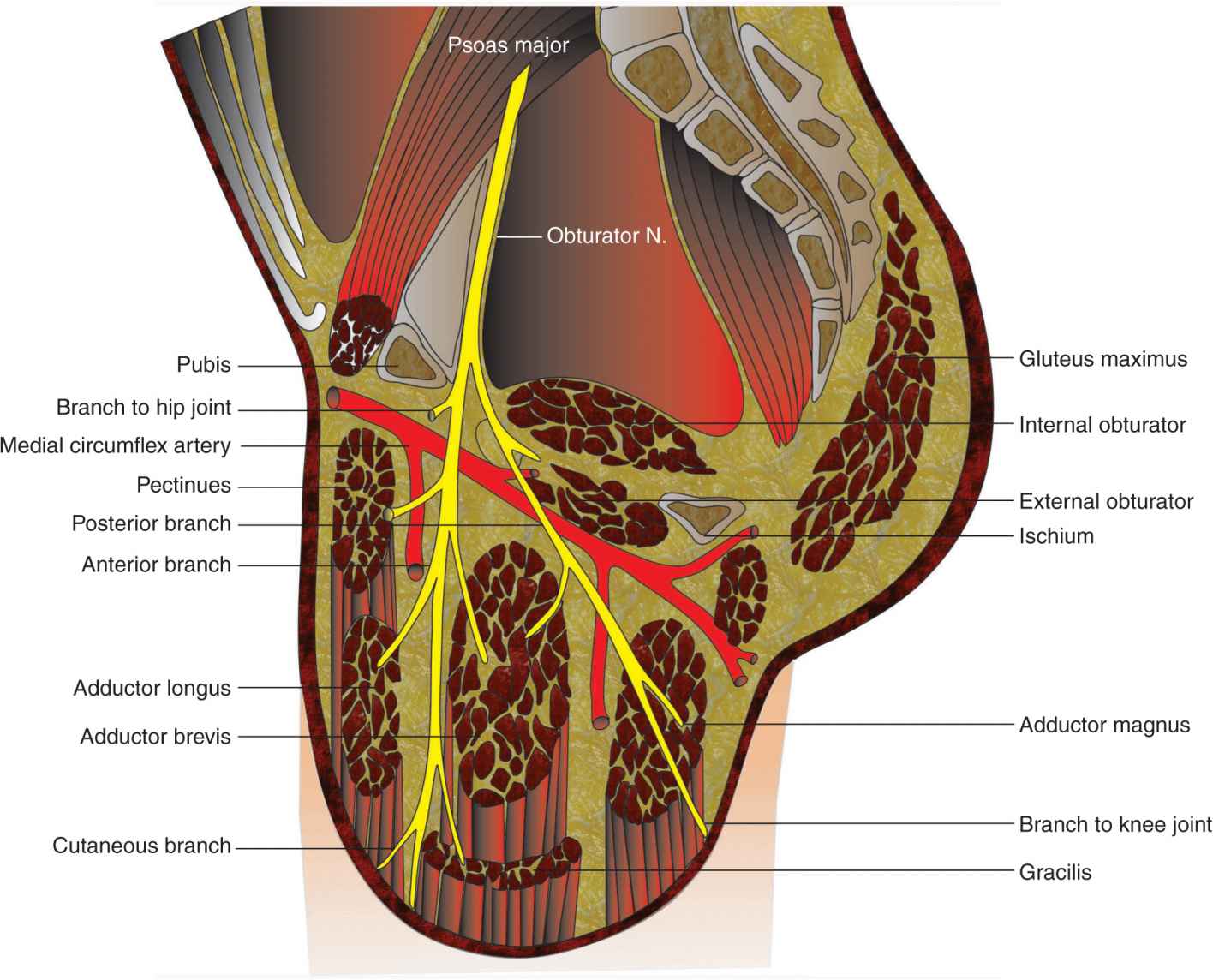
FIGURE 37-4. The course and divisions of the obturator nerve and their relationship to the adductor muscles.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


