Interscalene Brachial Plexus Block
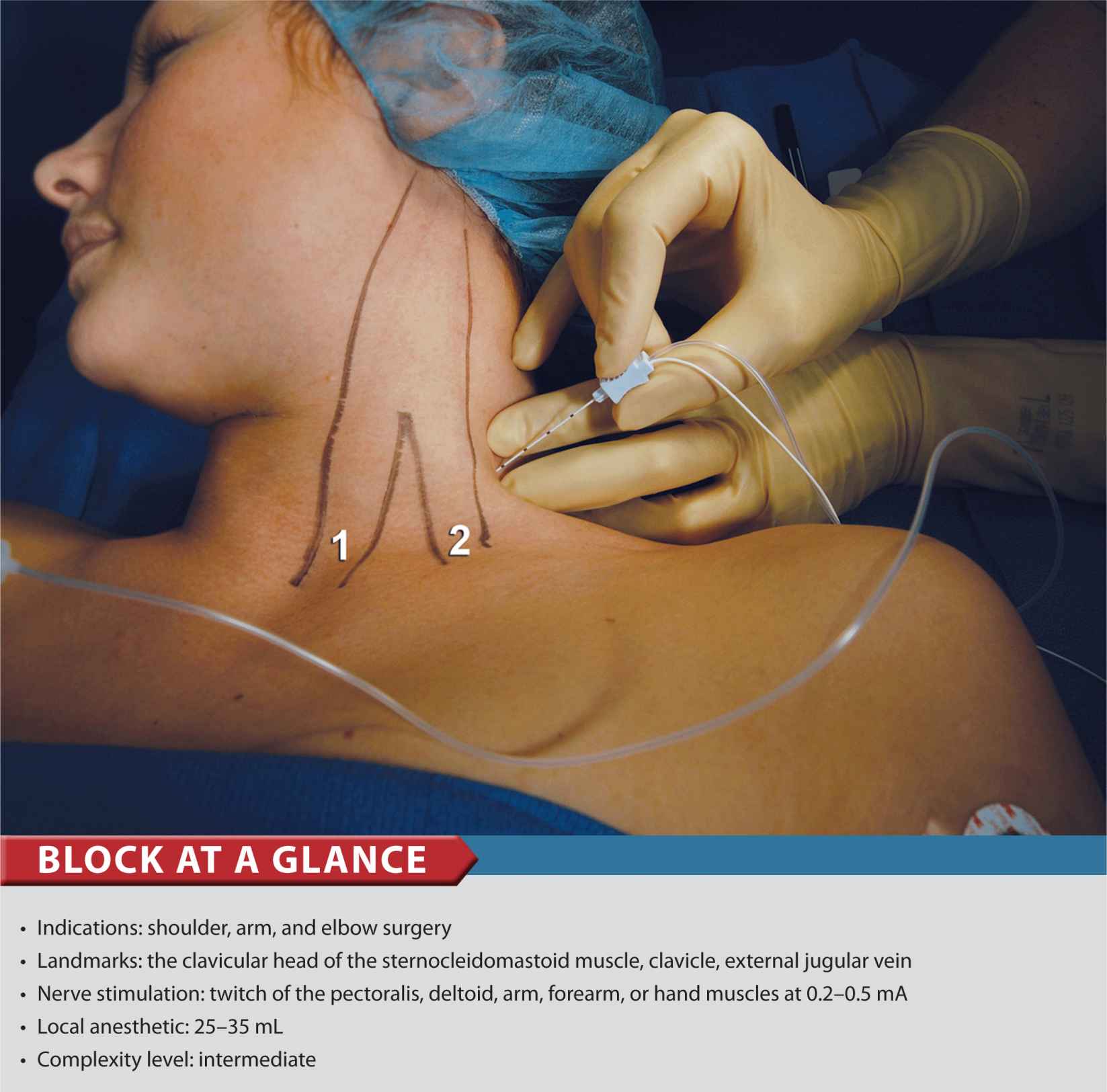
FIGURE 12-1. Needle insertion for interscalene brachial plexus block. The needle is inserted between palpating fingers that are positioned in the scalene groove (between anterior and middle scalene muscles). 1 = sternal head of the sternocleidomastoid muscle. 2 = clavicular head of the sternocleidomastoid muscle.
General Considerations
An interscalene block relies on the spread of a relatively large volume of local anesthetic within the interscalene groove to accomplish blockade of the brachial plexus. In our practice, we almost always use a low interscalene block technique, which consists of inserting the needle more caudally than in the commonly described procedure performed at the level of the cricoid cartilage. Our reasoning is that at the lower neck, the interscalene groove is more shallow and easier to identify, and the distribution of anesthesia is also adequate for elbow and forearm surgery. In addition, the needle insertion is more lateral, which makes puncture of the carotid artery less likely and performance of the block easier to master by trainees. Low approach to interscalene block is used in shoulder, arm, and forearm surgery. In our practice, the most common indications for this procedure are shoulder and humerus surgery and the insertion of an arteriovenous graft for hemodialysis.
Functional Anatomy
The brachial plexus supplies innervation to the upper limb and consists of a branching network of nerves derived from the anterior rami of the lower four cervical and the first thoracic spinal nerves. Starting from their origin and descending distally, the components of the plexus are named roots, trunks, divisions, cords, and, finally, terminal branches. The five roots of the cervical and the first thoracic spinal nerves (anterior rami) give rise to three trunks (superior, middle, and inferior) that emerge between the medial and anterior scalene muscles to lie on the floor of the posterior triangle of the neck (Figure 12-2). The roots of the plexus lie deep to the prevertebral fascia, whereas the trunks are covered by its lateral extension, the axillary sheath. Each trunk divides into an anterior and a posterior division behind the clavicle, at the apex of the axilla (Figure 12-3). The divisions combine to produce the three cords, which are named lateral, median, and posterior according to their relationship to the axillary artery. From this point on, individual nerves are formed as these neuronal elements descend distally (Figure 12-3 and Table 12-1).
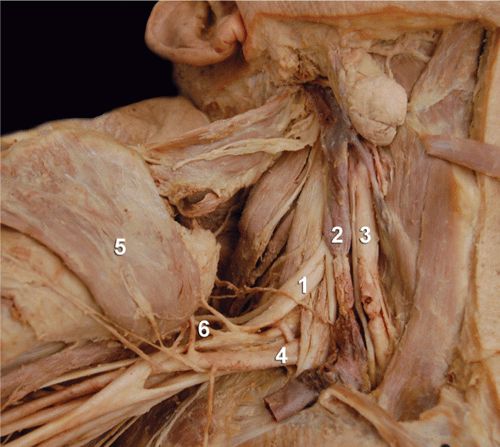
FIGURE 12-2. Anatomy of the brachial plexus. The sternocleidomastoid muscle is removed and the brachial plexus ![]() is seen emerging between the scalene muscles.
is seen emerging between the scalene muscles. ![]() internal jugular vein.
internal jugular vein. ![]() carotid artery.
carotid artery. ![]() subclavian artery.
subclavian artery. ![]() Retracted pectoralis muscle.
Retracted pectoralis muscle. ![]() medial and lateral pectoral nerves. The number “1” also indicates the approximate level at which the block is performed where the roots of the muscles are emerging between the scalene muscles.
medial and lateral pectoral nerves. The number “1” also indicates the approximate level at which the block is performed where the roots of the muscles are emerging between the scalene muscles.
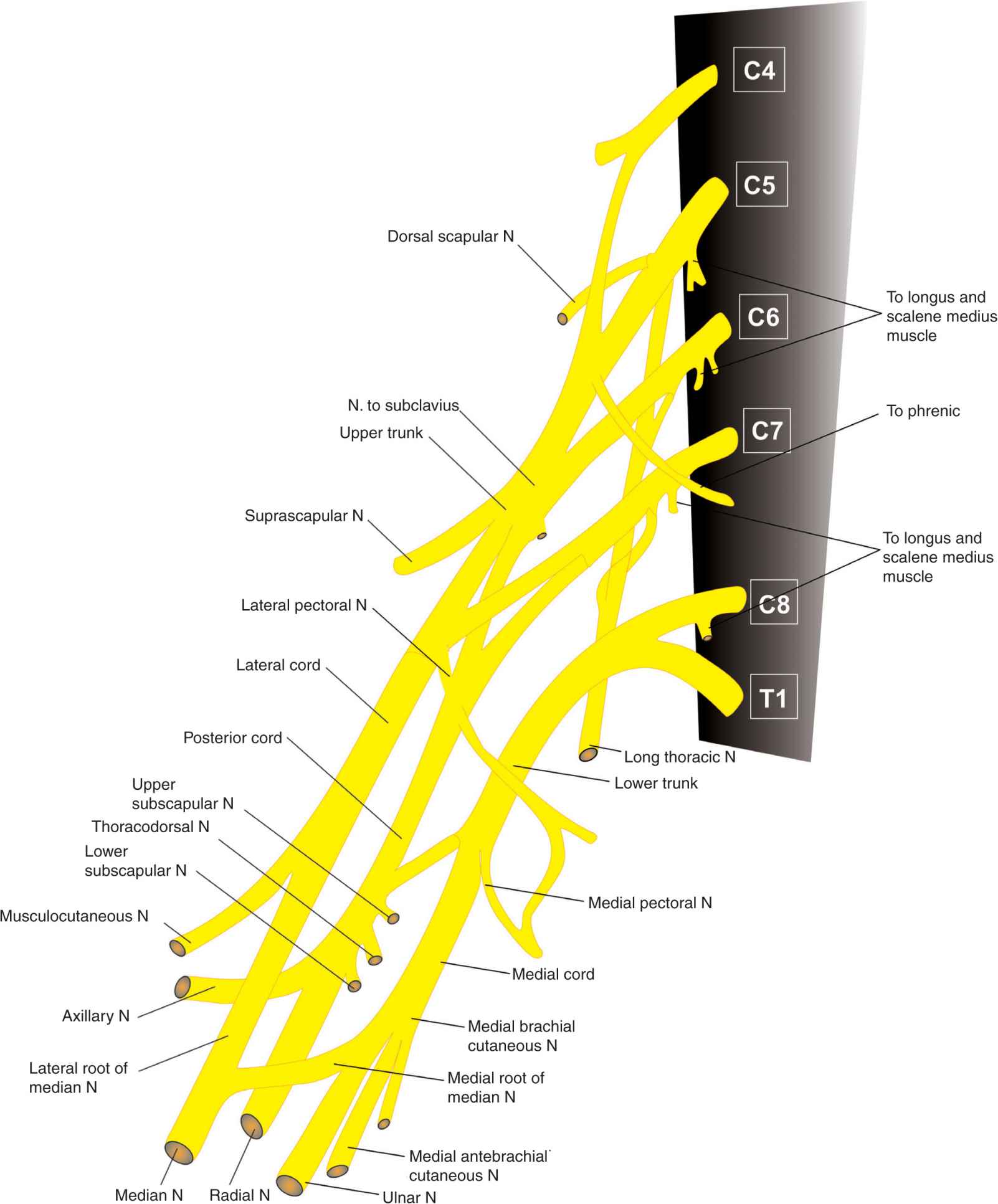
FIGURE 12-3. Functional organization of the brachial plexus and formation of the terminal nerves.
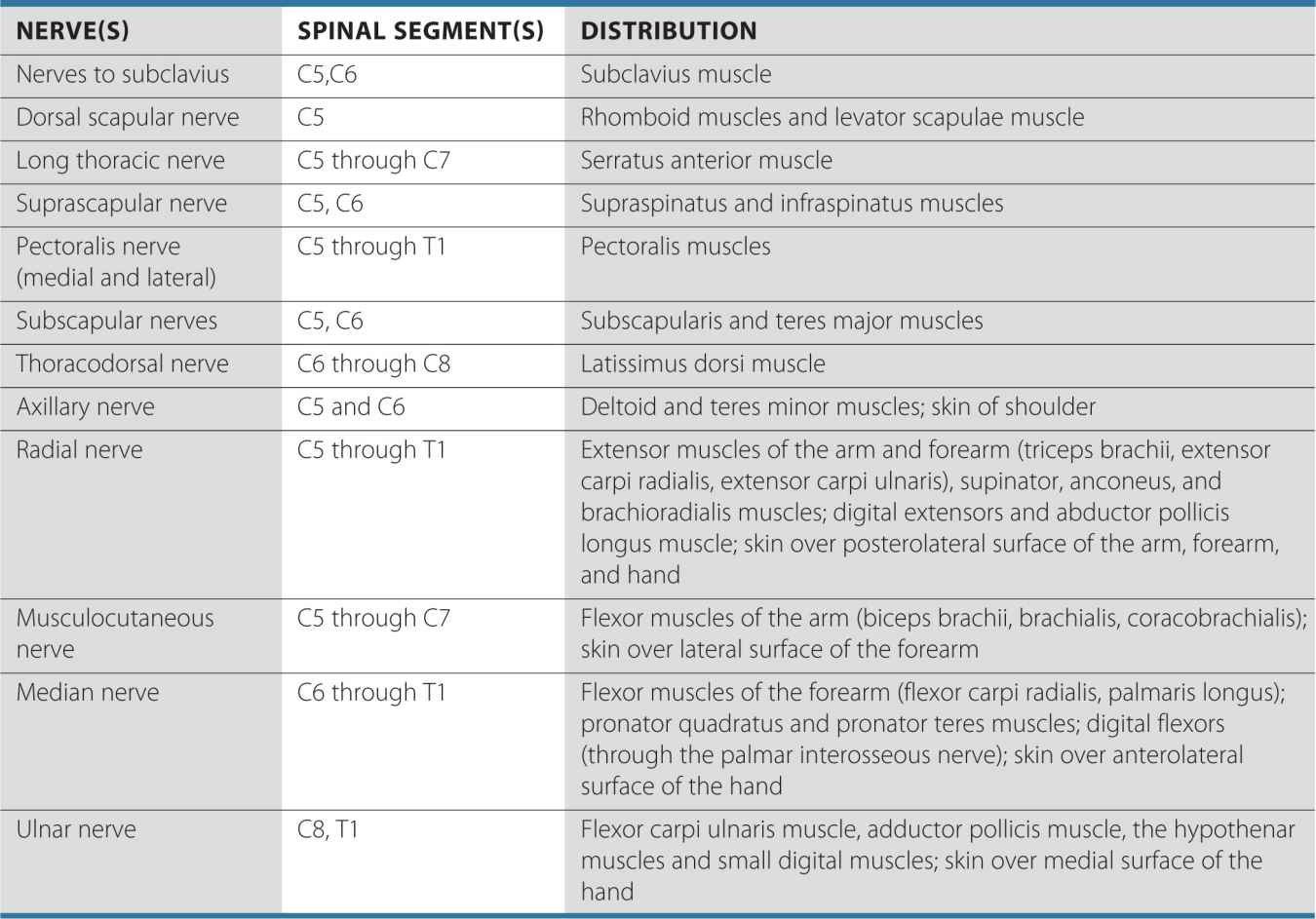
TABLE 12-1 Distribution of the Brachial Plexus
Distribution of Blockade
The interscalene approach to brachial plexus blockade results in anesthesia of the shoulder, arm, and elbow (Figure 12-4). Note that the skin over and medial to the acromion is supplied by the supraclavicular nerve, which is a branch of the cervical plexus. Supraclavicular nerves are usually blocked with the brachial plexus when an interscalene block is performed. This is because the local anesthetic invariably spills over from the interscalene space into the prevertebral fascia and blocks the branches of the cervical plexus. The classic interscalene block is not recommended for hand surgery due to potential sparing of the inferior trunk and the lack of blockade of the C8 and T1 roots.
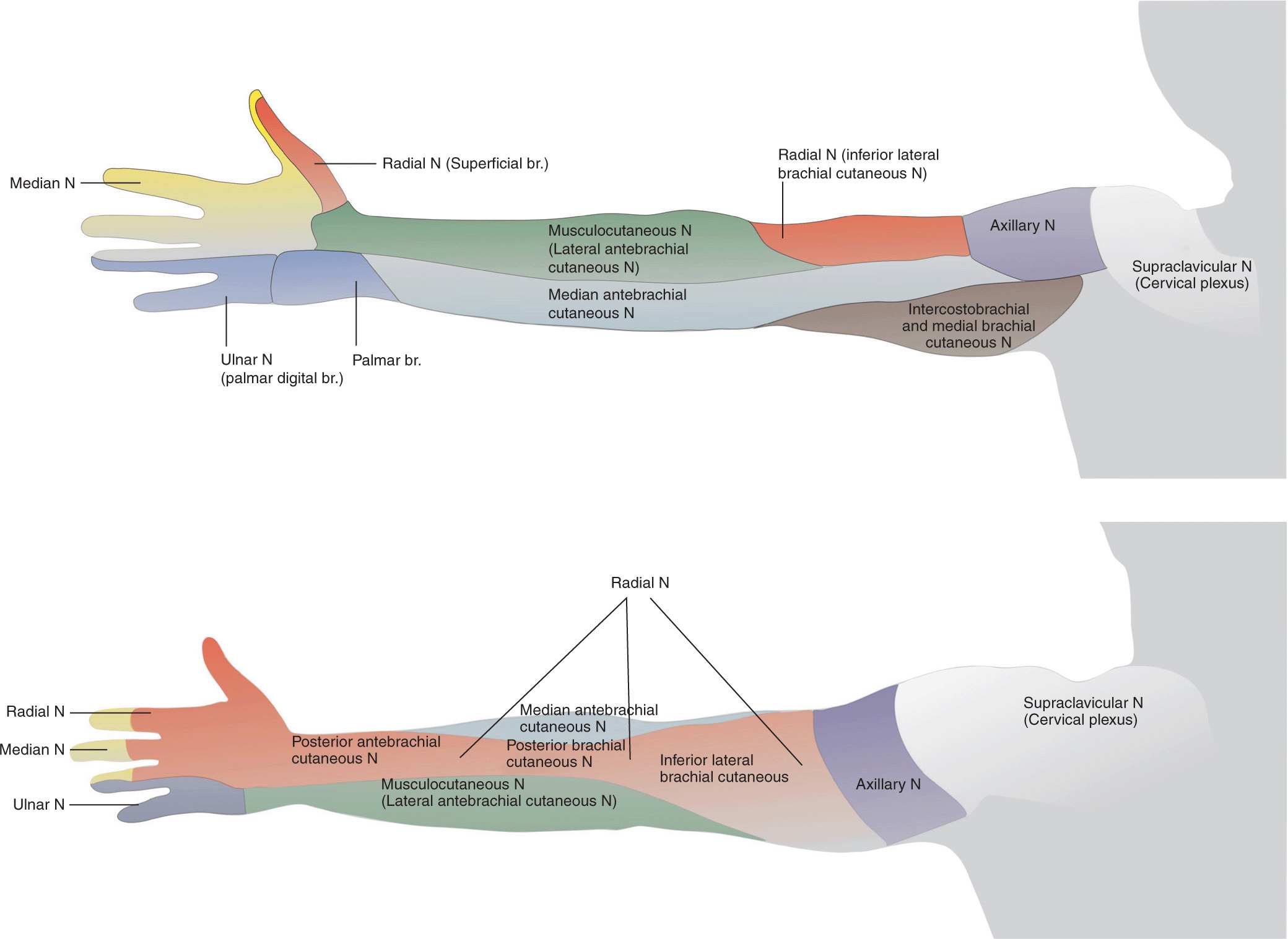
FIGURE 12-4. Sensory distribution of the brachial plexus. The innervation is shown for didactic purposes; the exact extent of anesthesia with interscalane block varies considerably and often spares the hand.
Single-Injection Interscalene Block
Equipment
A standard regional anesthesia tray is prepared with the following equipment:
• Sterile towels and gauze packs
• 2 × 20-mL syringes containing local anesthetic
• A 3-mL syringe and 25-gauge needle with local anesthetic for skin infiltration
• A 3.5-cm, 22-gauge, short-bevel insulated stimulating needle
• Peripheral nerve stimulator
• Sterile gloves; marking pen
Landmarks and Patient Positioning
The patient is in a supine or semi-sitting position with the head facing away from the side to be blocked (Figure 12-5). The arm should rest comfortably on the bed, abdomen, or arm-board to allow detection of responses to nerve stimulation. Removal of a cast (when present) can help to detect motor response, although removal is not essential because the responses to nerve stimulation are usually mixed (stimulation of trunks and divisions rather than specific nerves) and proximal motor response is adequate (e.g., deltoid, pectoralis).
FIGURE 12-5. Landmarks for the interscalene brachial plexus. White arrows: clavicle. Red arrows: posterior border of the sternocleidomastoid muscle. Blue arrow: external jugular vein. The palpating fingers are positioned lateral and posterior to the clavicular head of the sternocleidomastoid muscle in the space between anterior and middle scalene muscles. The scalene groove is often palpated just in front or behind the external jugular vein.
These are the primary landmarks for performing this block:
1. The clavicle
2. Posterior border of the clavicular head of the sternocleidomastoid muscle
3. External jugular vein (usually crosses the interscalene groove at the level of the trunks)
Maneuvers to Facilitate Landmark Identification
Identification of the interscalene groove can be made easier by performing the following steps:
• Ask the patient to reach for the ipsilateral knee with the limb to be blocked or passively pull the patient’s wrist inferiorly. This maneuver flattens the skin of the neck and helps identify both the scalene muscles and the external jugular vein.
• The sternocleidomastoid muscle can be accentuated by asking the patient to raise the head off the table (Figure 12-6).

FIGURE 12-6. Maneuver to extenuate the posterior border of the sternocleidomastoid muscle and external jugular vein by asking the patient to lift her head off of the table while looking away from the side to be blocked.
• The external jugular vein can be accentuated by asking the patient to perform a brief Valsalva maneuver.
• While palpating the interscalene groove, ask the patient to sniff forcefully. Sniffing tenses the scalene muscles, and the fingers of the palpating hand often fall into the interscalene groove.
The described landmarks should routinely be marked on the patient’s skin prior to performing the block.
Technique
After cleaning the skin with an antiseptic solution, 1 to 3 mL of local anesthetic is infiltrated subcutaneously at the determined needle insertion site.
The fingers of the palpating hand should be gently but firmly pressed between the anterior and middle scalene muscles to shorten the skin-brachial plexus distance. The skin over the neck can be very mobile, and care should be taken to stabilize the fingers as well as to stretch the skin gently between the two fingers to ensure accuracy in needle advancement and redirection. The palpating hand should not be allowed to move during the entire block procedure to allow for precise redirection of the needle when necessary.
The needle is inserted 3–4 cm (approximately 2 fingerbreadths) above the clavicle and advanced at an angle almost perpendicular to the skin plane (Figure 12-7). The needle must never be oriented cephalad; a slight caudal orientation reduces a chance for an inadvertent insertion of the needle into the cervical spinal cord. The nerve stimulator should be initially set to deliver 0.8 to 1.0 mA (2 Hz, 0.1 ms). The needle is advanced slowly until stimulation of the brachial plexus is obtained. This typically occurs at a depth of 1 to 2 cm in most all patients. Once appropriate twitches of the brachial plexus are elicited, 25 to 35 mL of local anesthetic are injected slowly with intermittent aspiration to rule out intravascular injection.

FIGURE 12-7. Needle insertion for interscalene brachial plexus block. The needle is inserted between fingers positioned in the interscalene groove with a slight caudad orientation to decrease the chance of entrance in the cervical spinal cord. White arrow: insertion of the sternal head of the sternocleidomastoid muscle. Red arrows: posterior border of the sternocleidomastoid muscle. Blue arrow: external jugular vein. The insertion point for the block is often immediately posterior to the external jugular vein.
This “low-interscalene” approach differs from the classic description of the interscalene block, which uses the cricoid cartilage as a landmark. The principal advantage to the low approach is that the brachial plexus is more compact at the lower levels, and reliable coverage of the upper, middle, and lower trunks can be achieved with a single injection (Figure 12-8). In contrast, the classic approach may spare the lower trunk, which limits its use for forearm and elbow surgery.
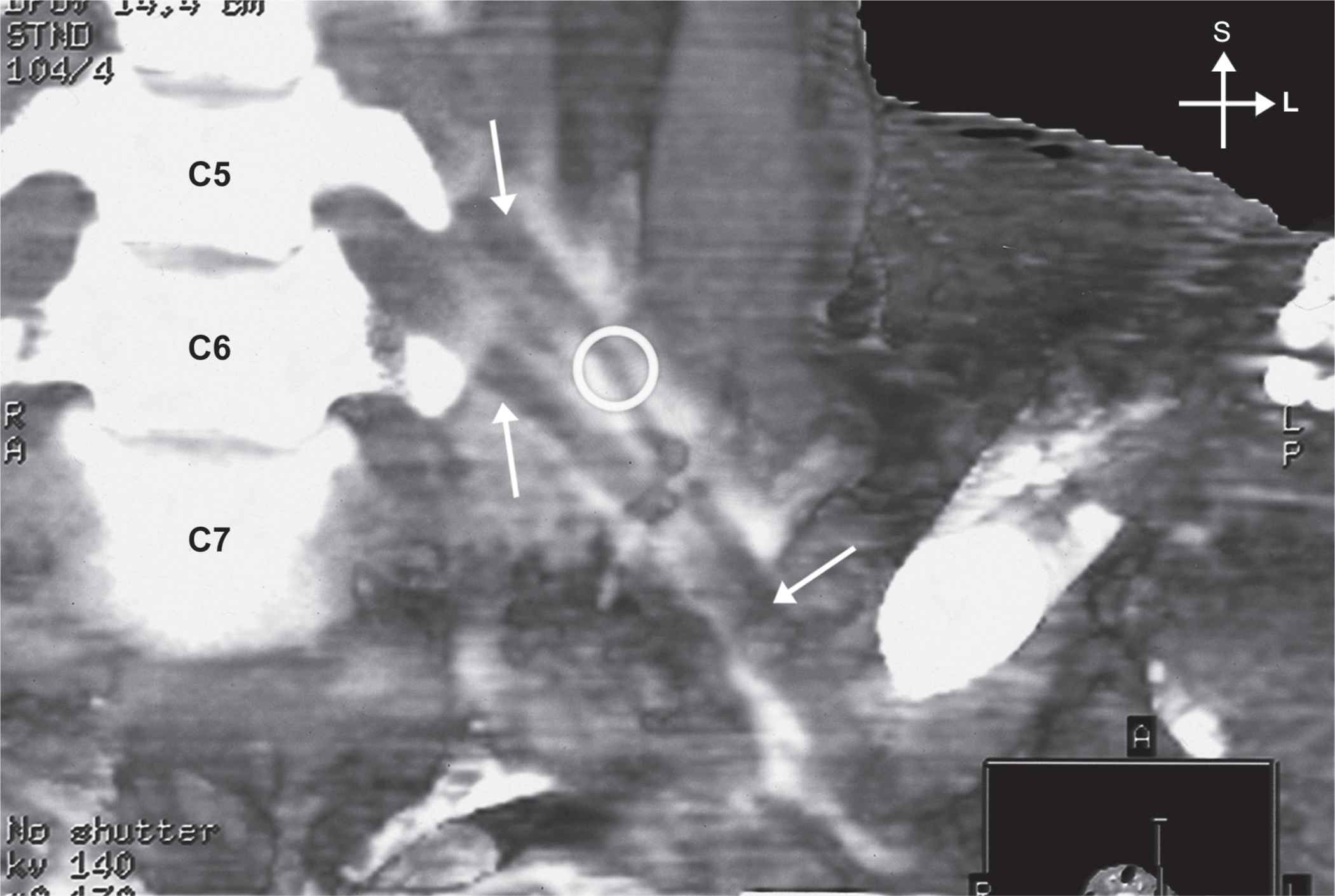
FIGURE 12-8. Distribution of the mixture of local anesthetic and a radiopaque contrast after an interscalene brachial plexus injection. The arrows and the circle indicate “negative” contrast image of the roots of the brachial plexus.
When insertion of the needle does not result in upper extremity muscle stimulation, the following maneuvers can be used (Figure 12-9):

FIGURE 12-9. Maneuvers to obtain a motor response of the brachial plexus during electric nerve localization. When the motor response is not obtained on the initial needle pass, the needle is redirected anteriorly or posteriorly to the original insertion plane as shown in the figure.
1. Keep the palpating hand in the same position and the skin between the fingers stretched.
2. Withdraw the needle to the skin level, redirect it 15° posteriorly, and repeat the needle advancement.
3. Withdraw the needle to the skin level, redirect it 15° anteriorly, and repeat the needle insertion.
Troubleshooting
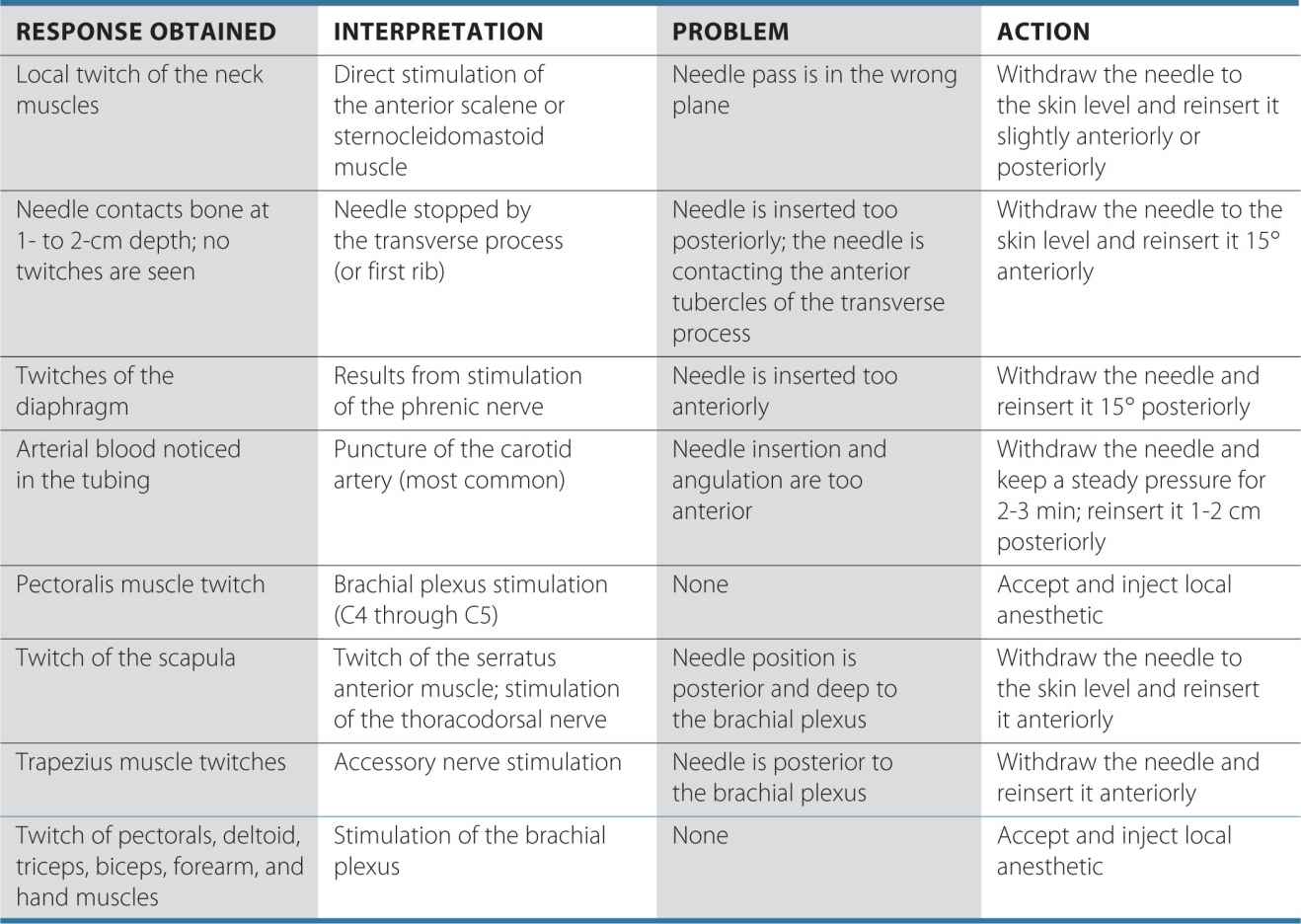
TABLE 12-2 Common Problems During Nerve Localization and the Corrective Action
Block Dynamics and Perioperative Management
When stimulation with a low-intensity current and slow needle advancement are used, interscalene brachial plexus block is associated with minor patient discomfort. Excessive sedation is not only unnecessary but also potentially disadvantageous because patient cooperation during landmark assessment and block performance is beneficial. The administration of benzodiazepines also may decrease the tone of the scalene and sternocleidomastoid muscles, making their recognition more difficult. We typically use small doses of midazolam (e.g., 1–2 mg) and/or short acting opioid (e.g., alfentanyl 250-500 mcg), so that the patient is comfortable and cooperative during nerve localization.
The onset time of this block is relatively short. The first sign of the blockade is typically a loss of coordination of the shoulder and arm muscles. This sign is seen sooner than the onset of a sensory blockade or a temperature change and, when observed within 1 to 2 minutes after injection, is highly predictive of a successful brachial plexus blockade. In patients undergoing shoulder arthroscopic procedures, it is important to note that the arthroscopic portals are often inserted outside the cutaneous distribution of the interscalene block. Local infiltration at the site of the incision by the surgeon is all that is needed because the entire shoulder joint and deep tissues are anesthetized with the interscalene block alone.
Education of the patient regarding block effects and side effects is important with interscalene block. Patients should be instructed to take prescribed oral analgesics and use ice packs before the block resolves. This regimen is of particular importance with ambulatory patients who may experience significant pain after discharge if they are unprepared.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


