FIGURE 34-1. Ultrasound-guided wrist block. Transducer and needle positions for (A) Median nerve block, (B) Ulnar nerve block, (C) Radial nerve block.
General Considerations
The wrist block is an effective method to provide anesthesia of the hand and fingers without the arm immobility that occurs with more proximal brachial plexus blocks. Traditional wrist block technique involves advancing needles using surface landmarks toward the three nerves that supply the hand, namely the median, ulnar, and radial nerves. The ultrasound-guided approach has the advantage of direct visualization of the needle and target nerve, which may decrease the incidence of needle-related trauma. In addition, because the needle can be placed with precision immediately adjacent to the nerve, smaller volumes of local anesthetic are required for successful blockade than with a blind technique. Since the nerves are located relatively close to the surface, this is a technically easy block to perform, but knowledge of the anatomy of the soft tissues of the wrist is essential for successful blockade with minimum patient discomfort.
Ultrasound Anatomy
Three individual nerves are involved:
Median Nerve
The median nerve crosses the elbow medial to the brachial artery and courses toward the wrist deep to the flexor digitorum superficialis in the center of the forearm. As the muscles taper toward tendons near the wrist, the nerve assumes an increasingly superficial position until it is located beneath the flexor retinaculum in the carpal tunnel with the tendons of flexor digitorum profundus, flexor digitorum superficialis, and flexor pollicis longus. A linear transducer placed transversely at the level of the wrist crease will reveal a cluster of oval hyperechoic structures, one of which is the median nerve (Figures 34-2A and B and 34-3A and B). At this location it is easy to confuse the tendons for the nerve, and vice versa; for this reason, it is recommended that the practitioner slides the transducer 5 to 10 cm up the volar side of the forearm, leaving the tendons more distally to confirm the location of the nerve. The tendons will have disappeared on the image, leaving just muscle and the solitary median nerve, which then can be carefully traced back to the wrist, if desired. In many instances, however, it is much simpler to perform a medianus block at the midforearm, where the nerve is easier to recognize.
FIGURE 34-2. (A) Ultrasound-guided block of the median nerve at the wrist. (B) Cross-sectional anatomy of the median nerve (MN) at the wrist.
FIGURE 34-3. (A) Cross-sectional ultrasound image of the median nerve (MN) at the wrist. (B) Needle (1) path to reach MN at the wrist and spread of local anesthetic to block the MN.
Ulnar Nerve
The ulnar nerve is located medial (ulnar side) to the ulnar artery from the level of the midforearm to the wrist. This provides a useful landmark. A linear transducer placed at the level of the wrist crease will show the hyperechoic anterior surface of the ulna with shadowing behind; just lateral to the bone and very superficial will be the triangular or oval hyperechoic ulnar nerve, with the pulsating ulnar artery immediately next to it (Figures 34-4A and B and 34-5A and B). Unlike the median nerve, there are fewer structures (tendons) in the immediate vicinity that can confuse identification; however, the same confirmation scanning technique can be applied. Sliding the transducer up and down the arm helps verify that the structure is the ulnar nerve by following the course of the ulnar artery and looking for the nerve on its ulnar side.
FIGURE 34-4. (A) Block of the ulnar nerve (UN) at the wrist. Transducer and needle position. (B) Transsectional anatomy of the UN at the wrist. UN is seen just medial to the ulnar artery (UA).
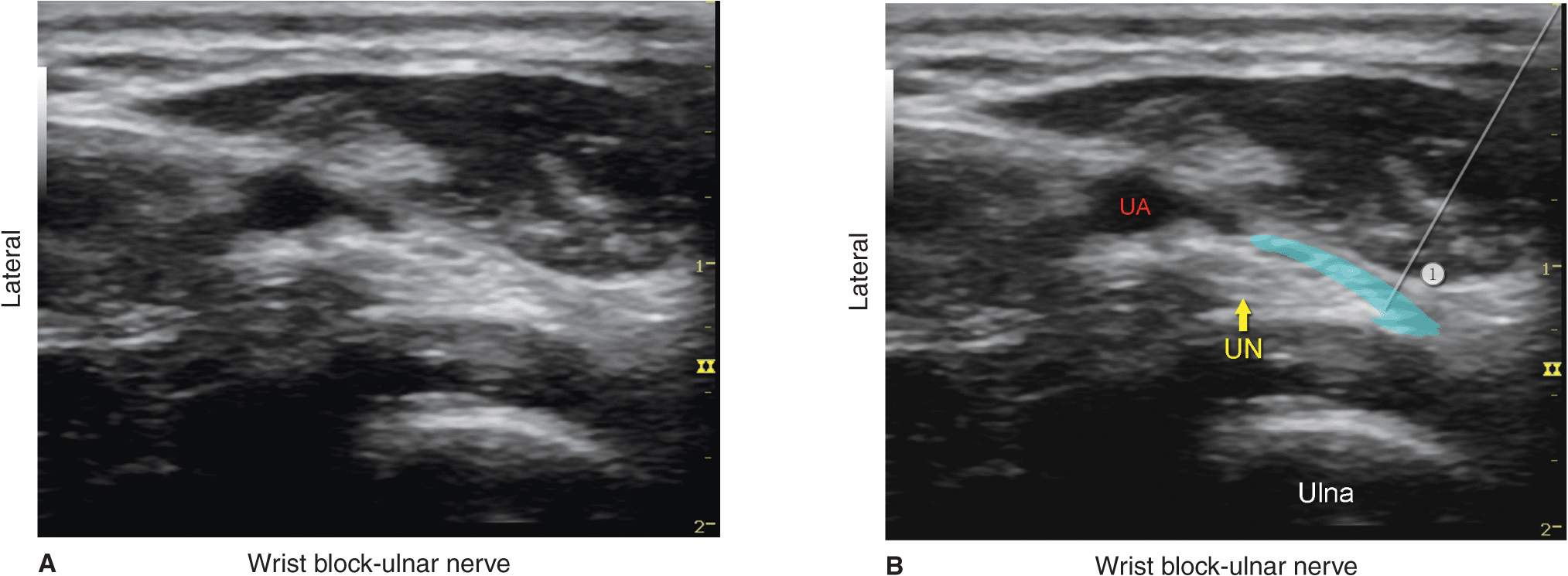
FIGURE 34-5. (A) Sonoanatomy of the ulnar nerve (UN) at the wrist. US, ulnar artery. (B) Needle path to reach the UN at the wrist and approximate spread of the local anesthetic (area shaded in blue) to anesthetize the UN.
Radial Nerve
The superficial branch of the radial nerve divides into terminal branches at the level of the wrist; for this reason, ultrasonography is not very useful for guidance for placement of the block at the level of the wrist. A subcutaneous field block around the area of the styloid process of the radius remains an easy method to perform an effective radial nerve block at the level of the wrist (refer to the wrist block in Chapter 16). However, ultrasonography can be used at the elbow level or in the midforearm. At the level of the elbow (slightly below the elbow), the nerve is easily identified as a hyperechoic oval or triangular structure in the layer between the brachialis (deep) and brachioradialis (superficial) muscles lateral to the radial artery (Figures 34-6A and B and 34-7A and B).
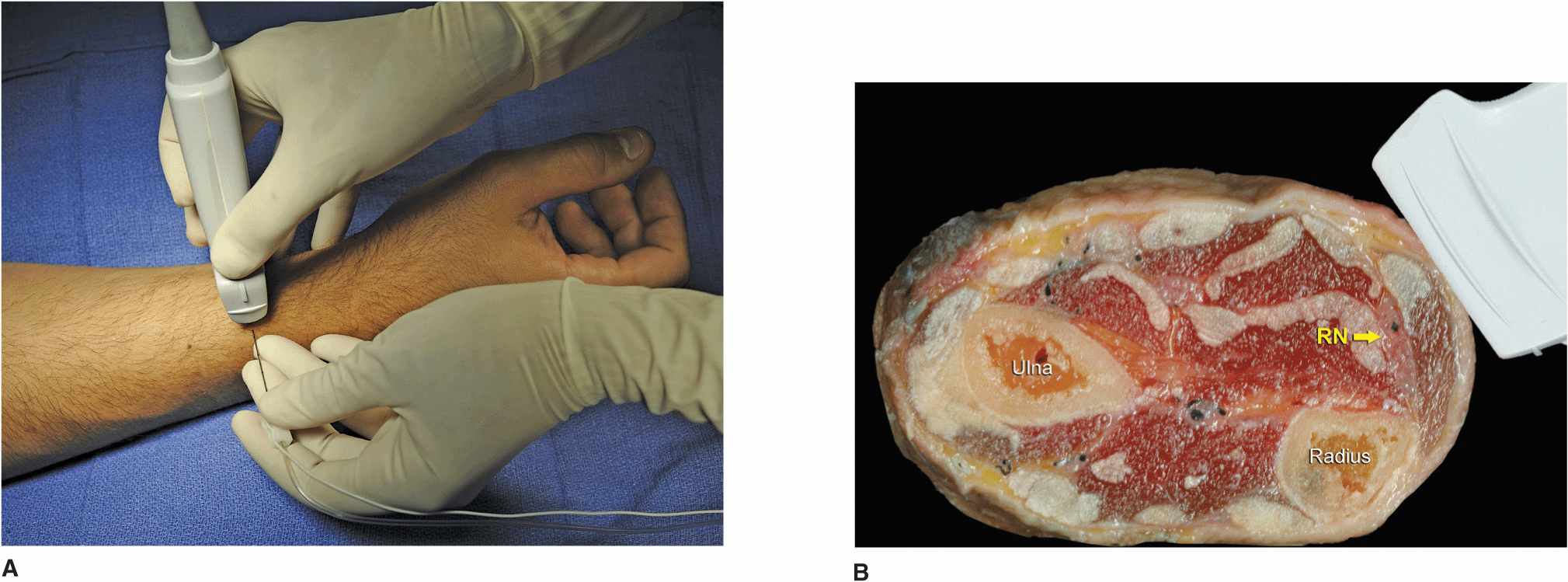
FIGURE 34-6. (A) Block of the radial nerve (RN) at the wrist. Transducer and needle position. (B) Cross-sectional anatomy of the RN at the wrist level. Superficial branches of the radial nerve are highly variable at this level in number, size, and depth. For that reason, block of the RN at the wrist is not an exact technique but rather infiltration of the local anesthetic in the subcutaneous tissue and underneath the superficial fascia.
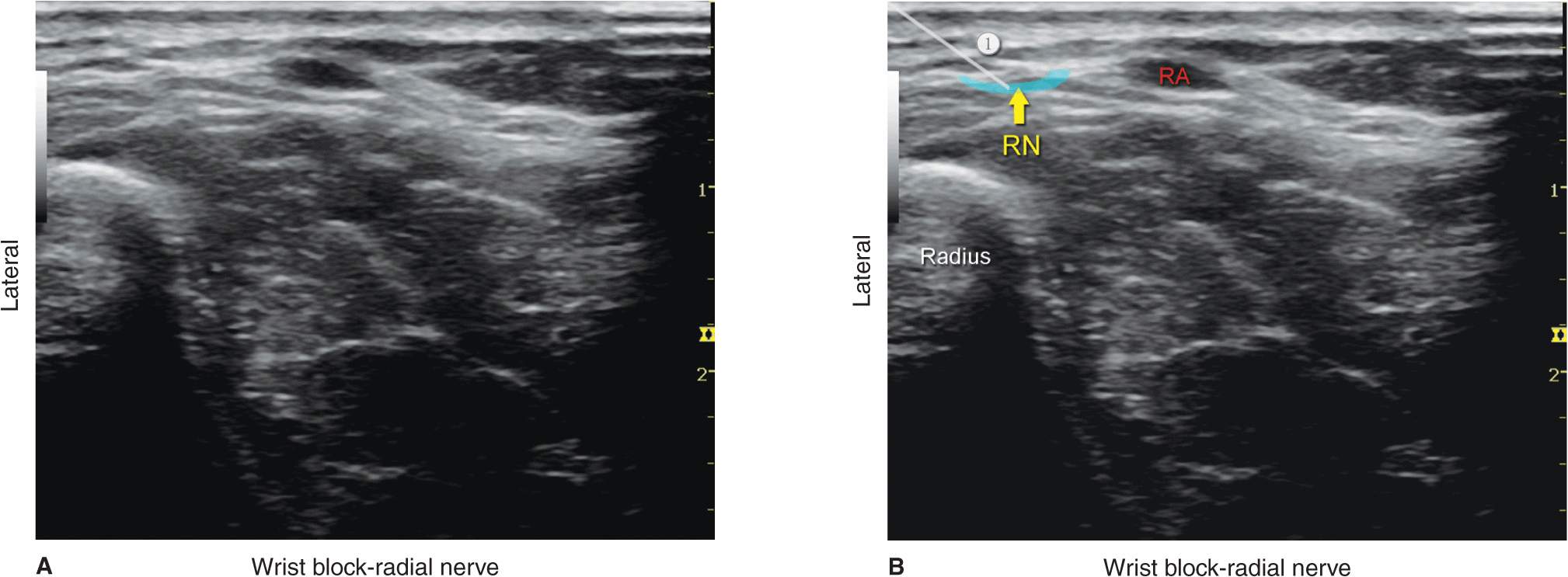
FIGURE 34-7. (A) Sonoanatomy of the radial nerve (RN) at the level of the wrist. (B) One branch of the RN at the wrist is shown lateral to the radial artery (RA), and the approximate needle path to reach a branch of the radial nerve is shown with an approximate spread of local anesthetic (area shaded in blue) to anesthetize it.
Distribution of Blockade
A wrist block results in anesthesia of the entire hand. For a more comprehensive review of the distribution of each terminal nerve, please see Chapter 1, Essential Regional Anesthesia Anatomy.
Equipment
Equipment needed includes the following:
• Ultrasound machine with linear transducer (8–14 MHz), sterile sleeve, and gel
• Standard nerve block tray (described in the equipment section)
• One 20-mL syringe containing local anesthetic
• A 1.5-in 22- to 25-gauge needle with low-volume extension tubing
• Sterile gloves
Landmarks and Patient Positioning
The wrist block is most easily performed with the patient in the supine position to allow for the volar surface of the wrist to be exposed. It is useful to remove splints and/or bandages on the hand to facilitate placement of the transducer and sterile preparation of the skin surface.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


