Ultrasound-Guided Saphenous Nerve Block
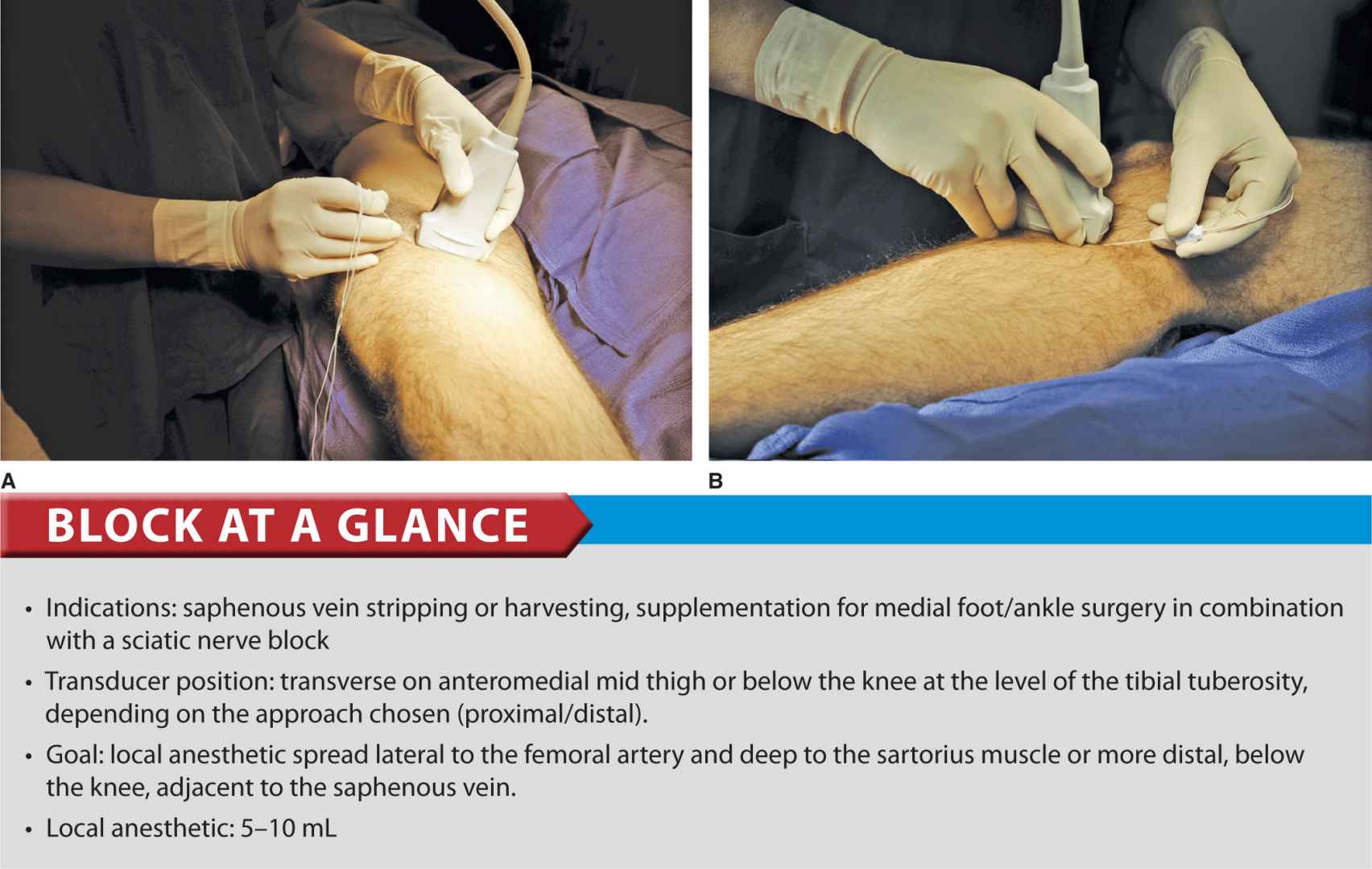
FIGURE 38-1. Needle insertion to block the saphenous nerve at the level of the mid thigh (A) or below the knee (B).
General Considerations
The saphenous nerve is the terminal sensory branch of the femoral nerve. It supplies innervation to the medial aspect of the leg down to the ankle and foot. Blockade of the nerve can be sufficient for superficial procedures in this area; however, it is most useful as a supplement to a sciatic block for foot and ankle procedures that involve the superficial structures in medial territory. The use of ultrasound guidance has improved the success rates of the saphenous blocks, compared with field blocks below the knee and blind transsartorial approaches. The ultrasound-guided techniques described here are relatively simple, quick to perform, and fairly reproducible.
Ultrasound Anatomy
The sartorius muscle forms a “roof” over the adductor canal in the lower half of the thigh in its descent laterally-to-medially across the anterior thigh. The muscle appears as an oval shape beneath the subcutaneous layer of adipose tissue. Often, the femoral artery, which passes beneath the muscle, can also be palpated. The sides of the triangular canal are formed by the vastus medialis laterally and adductor longus or magnus medially (depending on how proximal or distal the scan is). The saphenous nerve is infrequently seen on the ultrasound image; however, sometimes it is visualized as a small round hyperechoic structure medial to the artery. A femoral vein accompanies the artery and saphenous nerve, which are all typically visualized at 2 to 3 cm depth. When attempting to identify the saphenous nerve on ultrasound image, the following anatomic considerations should be kept in mind:
• Above the knee: The saphenous nerve pierces the fascia lata between the tendons of the sartorius and gracilis muscles before becoming a subcutaneous nerve.
• The saphenous nerve also may surface between the sartorius and vastus medialis muscles. (Figure 38-2 A, B, and C).
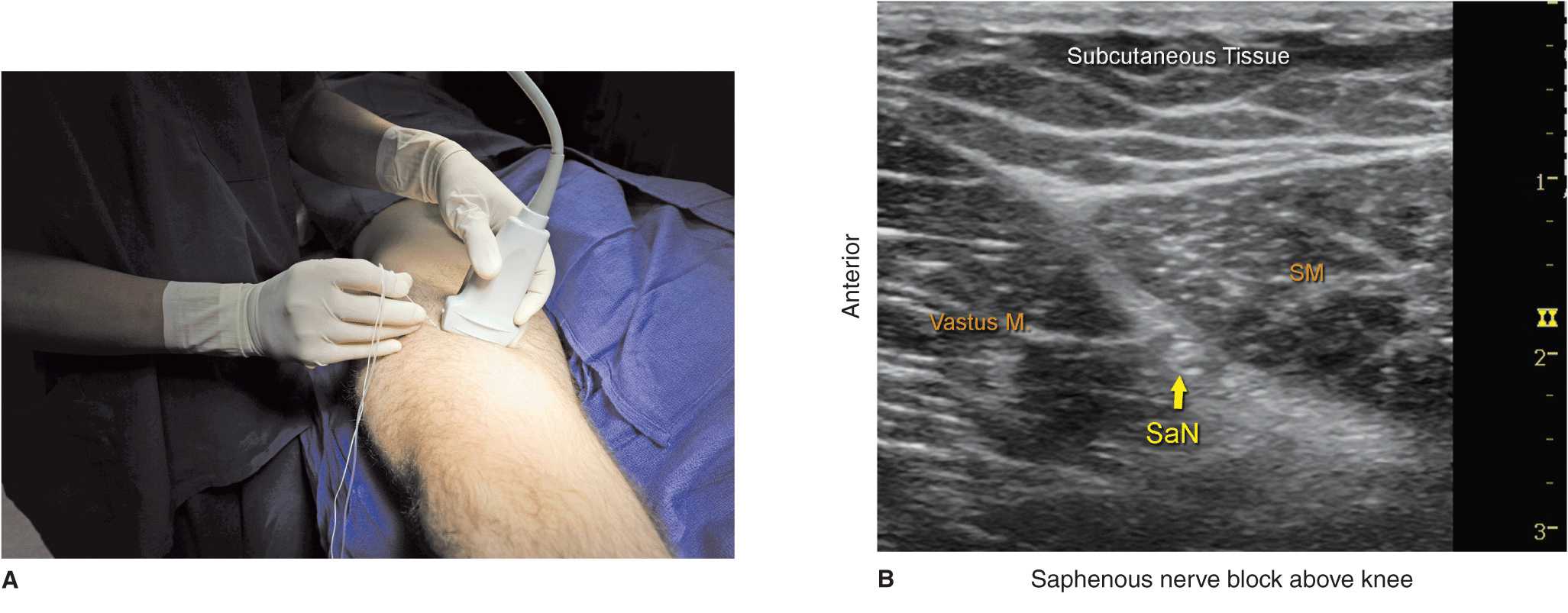
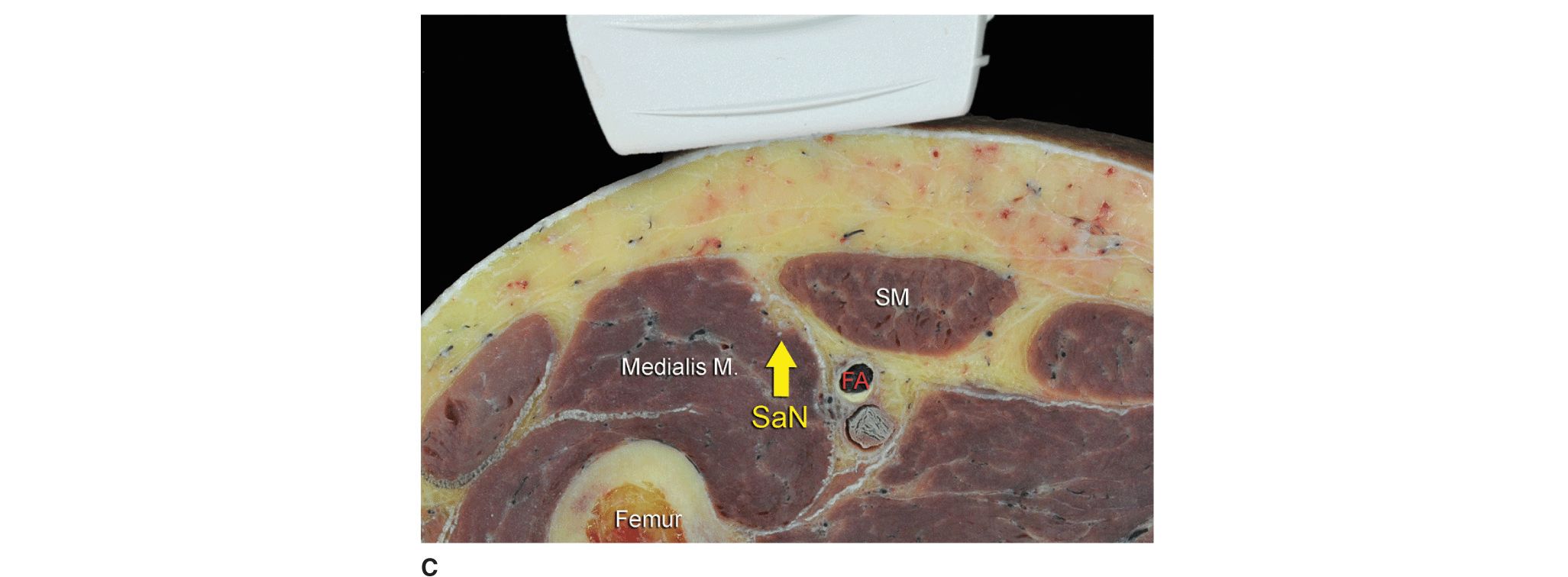
FIGURE 38-2. (A) Transducer and needle position for a saphenous nerve block at the level of the midthigh. (B) Ultrasound anatomy demonstrating saphenous nerve (SaN) in the tissue plane between the sartorius muscle (SM) and vastus medialis muscle. (C) Cross-sectional anatomy of the saphenous nerve at the level of the thigh. Saphenous nerve is shown positioned between the SM and the vastus medialis muscle. In this example the sartorius nerve is positioned superficially to the femoral artery (FA) and vein (unlabeled oval structure posterior to the FA).
• Below the knee, the nerve passes along the tibial side of the leg, adjacent to the great saphenous vein subcutaneously (Figure 38-3A, B, and C).
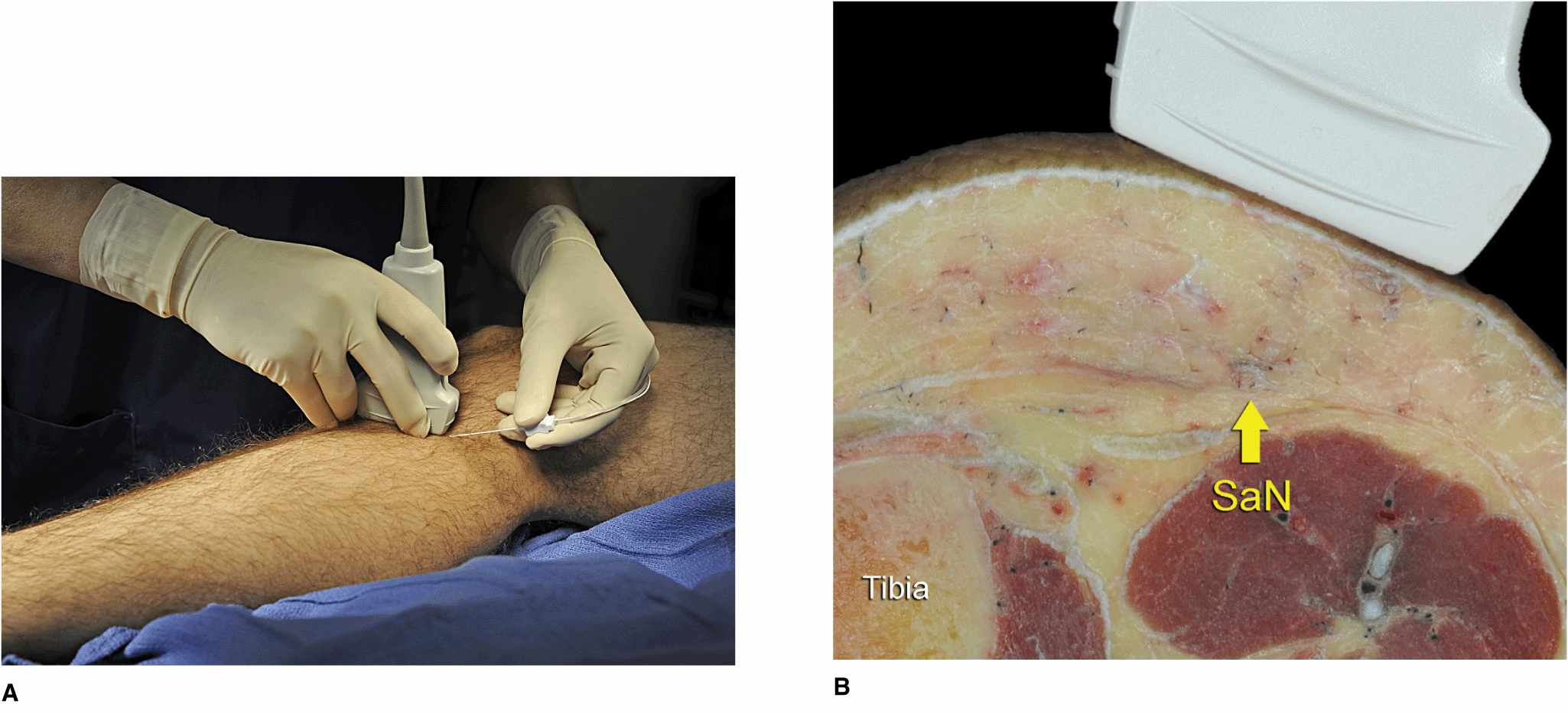
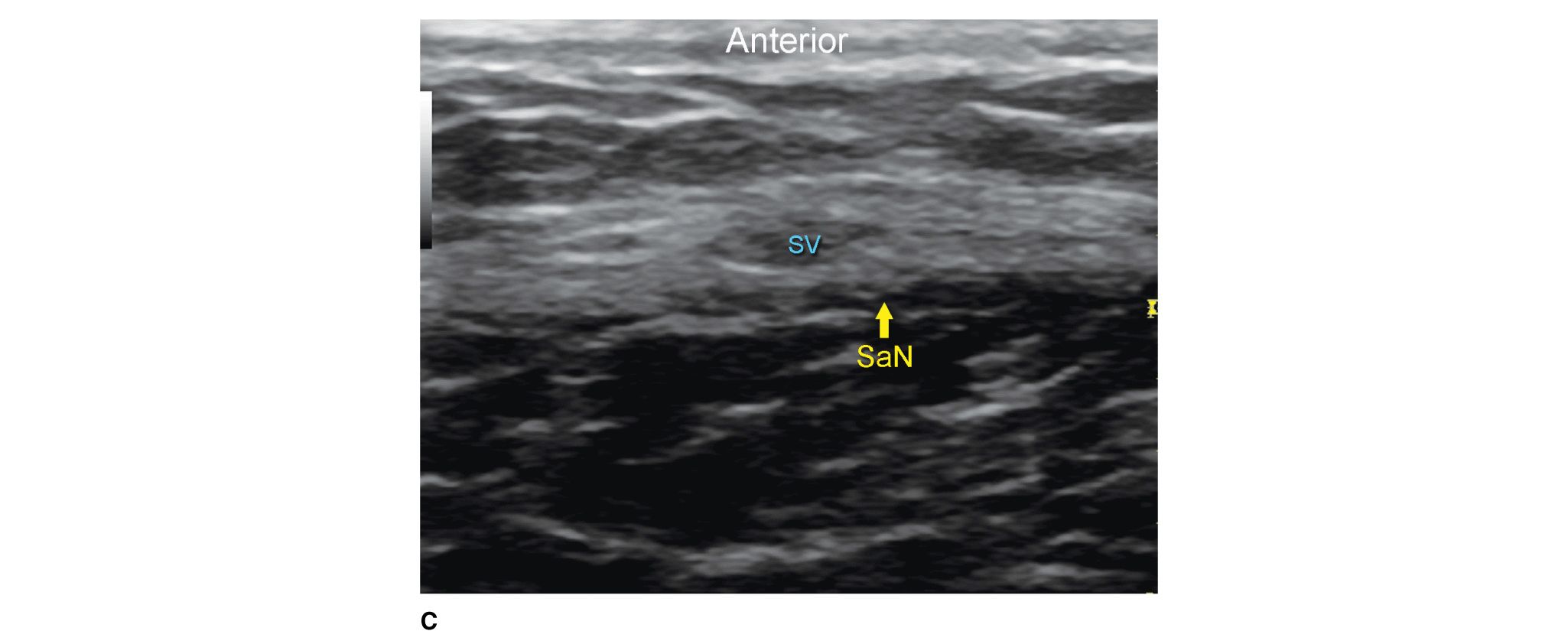
FIGURE 38-3. (A) Ultrasound transducer and needle insertion technique to block the saphenous nerve (SaN) at the level of the tibial tuberosity. (B) Cross-sectional anatomy of the SaN at the level of the tibial tuberosity. (C) Ultrasound image of the saphenous nerve (SaN) at the level below the knee. SaN is seen in the immediate vicinity of the saphenous vein (SV). Transducer should be applied lightly to avoid compression of the saphenous vein (SV) because the vein serves as an important landmark for technique.
• At the ankle, a branch of the nerve is located medially next to the subcutaneously positioned saphenous vein.
Distribution of Blockade
Saphenous nerve block results in anesthesia of a variable strip of skin on the medial leg and foot. For a more comprehensive review of the femoral and saphenous nerve distributions, see Chapter 1. Of note, although saphenous nerve is a strictly sensory block, an injection of the local anesthetic in the adductor canal can result in the partial motor block of the vastus medialis. For this reason, caution must be excercised when advising patients regarding the safety of unsupported ambulation after proximal saphenous block.
Equipment
Equipment needed is as follows:
• Ultrasound machine with linear transducer (8–14 MHz), sterile sleeve, and gel
• Standard nerve block tray (described in Chapter 3)
• One 10-mL syringe containing local anesthetic
• A 50-mm, 22-gauge short-bevel needle
• Peripheral nerve stimulator to elicit sensory sensation.
• Sterile gloves
Landmarks and Patient Positioning for Proximal Approach
The patient is placed in any position that allows for comfortable placement of the ultrasound transducer and needle advancement. Although prone and lateral approaches are possible, this block typically is performed with the patient in the supine position, with the thigh abducted and externally rotated to allow access to the medial thigh (Figure 38-2A). If difficulty confirming the sartorius muscle is encountered, exposure of the entire thigh in order to scan down from the anterosuperior iliac spine is useful.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


