A 73-year-old man with symptomatic benign prostatic hypertrophy is scheduled for transurethral resection of the prostate (TURP). His past medical history is significant for hypertension and a myocardial infarction 3 years ago, followed by a threevessel, coronary artery graft. The blood pressure is now well controlled with atenolol. He has occasional exertionrelated chest pain that responds to a single dose of nitroglycerin or rest. Transthoracic echocardiography revealed left ventricular wall hypokinesis and an ejection fraction of 42% with no other abnormalities.
Anesthesia is accomplished with a subarachnoid block using 12.5 mg bupivicaine with epinephrine 1:200,000 that achieves a dense block to T8. Small ephedrine boluses are used to support the blood pressure until surgical resection begins. The patient’s intraoperative course is uneventful and surgery, using a bipolar resectoscope with normal saline as irrigant, is completed in 75 minutes.
The level of anesthetic block on admission to the postanesthesia care unit (PACU) has receded to T10. A total of 1,600 mL of normal saline had been infused, and estimated blood loss was 50 mL. Initially, the patient does well, but over the ensuing hour, he develops progressive dyspnea and a lowering of his blood pressure. Physical examination reveals bilateral crackles, and chest radiograph demonstrates diffuse fluffy infiltrates bilaterally. The patient’s electrolytes are normal; specifically, the measured serum sodium is 143 mEq per L ([Na+] = 140 mEq per L, preoperatively). He denies vision changes and shows no signs of neurologic excitability. He is treated with a diuretic for the presumed congestive heart failure, diureses 800 mL, and is discharged to the ward 2 hours later. Without evidence of electrolyte changes or neurologic symptoms, would this still be considered an example of the TURP syndrome?
INTRODUCTION
Benign prostatic hypertrophy is a condition that ultimately affects more than 50% of elderly men.1 The prominent clinical features of the disease arise from progressive bladder outlet obstruction. Although improved medical and minimally invasive therapies have reduced the number of surgical interventions performed, TURP continues to be necessary and is performed more than 100,000 times annually in the United States (and 25,000 times annually in the United Kingdom).
Surgery performed through the urethra has a known profile of risks. These include hemorrhage, perforation, nerve injury, and later development of urethral strictures. The TURP syndrome has traditionally been associated most notably with the acute onset of hypervolemia, profound hyponatremia, neurologic excitability, seizures, hemodynamic changes, renal failure, blindness, and, occasionally, even death. This constellation of clinical findings stem from the surgical use and rapid intravascular absorption of electrolyte-free irrigation fluid.
Presenting signs and symptoms will depend both on the absorbed volume and the type of irrigant used. In general, more than 3 L of electrolyte-free, irrigating fluid needs to be absorbed to result in a severe form of this syndrome, whereas between 1 and 3 L is required to elicit a mild syndrome.2 The amount of normal saline absorbed that will elicit symptoms in this aged patient group is not known.
An answer to the question posed at the end of the case synopsis requires, first, that there is agreement on what constitutes the TURP syndrome. Historically, the syndrome is considered to represent a severe clinical situation with a large variety of symptoms affecting the circulatory and neurologic systems. Milder forms clearly exist.3,4 The diagnosis is usually made during or after surgery with a monopolar resectoscope. Evidence of acute serum electrolyte dilution, such as hyponatremia or an acute serum concentration rise of a compound contained only in the irrigation fluid, such as glycine or ethanol, must exist. However, newer surgical instruments and techniques that are touted to reduce the volume of absorbed irrigant or that allow use of physiologic isoosmolar solutions for irrigation will change this traditional presentation, eliminating the possibility of acute hyponatremia.
Minimally invasive—transurethral vaporization of the prostate, photoselective vaporization of the prostate with KTP laser, and Holmium-YAG laser resection of the prostate
Transurethral vaporization-resection of the prostate and
Techniques that utilize a bipolar resectoscope
Whichever of these newer treatment options ultimately prevail, it seems certain that variability to the presentation of TURP syndrome will narrow and that the frequency of its occurrence will diminish, or perhaps even disappear, as use of these techniques increase.1 In the future, it will be the sequelae of acute hypervolemia rather than acute hyponatremia, hyperglycinemia, hypoosmolality, and neurologic signs and symptoms that seal the diagnosis.
Until these newer surgical interventions for TURP are in broader use, however, there will remain an interest in recognizing the complications from TURP associated with use of the monopolar resectoscope, still considered by many as the “gold standard” instrument for TURP.5,6,7 This chapter will focus on the pathophysiologic basis of the TURP syndrome and discuss the prevailing opinion on the best anesthetic management practices.
How Is Transurethral Resection of the Prostate Accomplished?
Surgical features of TURP vary (see Table 33.1).4,8,9 The speed of prostatic resection averages approximately 0.6 g per minute, even when the newer bipolar resectoscopes are employed.9 The irrigation used ranges from distilled water to a variety of nonhemolytic glucose, urea, glycine, sorbitol, mannitol, and, with the bipolar resectoscopes, physiologic saline solutions.1
TABLE 33.1 Average and Extreme Statistics Reported with Transurethral Resection of the Prostate
aTrépanier CA, Lessard MR, Brochu J, et al. Another feature of TURP syndrome: Hyperglycaemia and lactic acidosis caused by massive absorption of sorbitol. Br J Anaesth. 2001;87:316.
bHurlbert BJ, Wingard DW. Water intoxication after 15 minutes of transurethral resection of the prostate. Anesthesiology. 1979;50:355.
cHjertberg H, Petterson B. The use of a bladder pressure warning device during transurethral prostatic resection decreases absorption of irrigating fluid. Br J Urol. 1992;69:56.
dNorlén H, Allgén LG, Vinnars E, et al. Glycine solution as an irrigating agent during transurethral prostatic resection. Scand J Urol Nephrol. 1986;20:19.
eNorlén H, Allgén LG, Wicksell B. Sorbitol concentrations in plasma in connection with transurethral resection of the prostate using sorbitol solution as an irrigating fluid. Scand J Urol Nephrol. 1986;20:9.
fMitnick PD, Bell S. Rhabdomyolysis associated with severe hyponatremia after prostatic surgery. Am J Kidney Dis. 1990;XVI:73.
TURP, transurethral resection of the prostate.
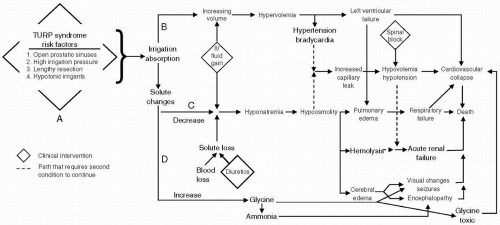
In the 1950s, the incidence of the TURP syndrome was as high as 10%.10 With modern surgical techniques and improved clinical awareness, this incidence has been reduced to no more than 4% among patients undergoing TURP,4 although occasionally the incidence is still reported much higher.11 These data show that, despite the advances that have been made, the TURP syndrome continues to occur with significant frequency. The diagnosis remains difficult to make because the syndrome can develop over multiple pathways and lacks a stereotypical presentation (see Fig. 33.1, Table 33.2).
Why Does Intravascular Volume Expansion Occur?
Absorption requires, as a first step, a path for entry of fluid into the body. Irrigation fluid gains direct intravascular access when the prostatic venous plexus is opened during resection near the prostatic capsule. Once the venous plexus is opened, whether recognized or not, further absorption is possible for the remainder of the procedure. Fluid can also be absorbed indirectly following an injury to the prostatic capsule or if the bladder neck is divided, whereupon irrigation fluid extravasates into the retroperitoneum or peritoneum, and intravascular absorption occurs only gradually.12,13
After fluid absorption by any route—the second step on the path to developing the TURP syndrome—is measurable in 34% (transurethral vaporization of the prostate) to 46% (TURP) of procedures.12,14 Extravasation of fluid may occur in 4% to 20% of patients having TURP.4,9 The force driving absorption by extravasation is the irrigation fluid pressure in the bladder. Intravesicular pressure may be related to the height of the irrigation bag above the prostatic sinuses and explains why surgeons have been admonished to raise the irrigation bag no more than 60 cm above the height of the bladder.15 For absorption to occur, the irrigation fluid pressure must exceed the receiving compartment pressure. Hence, intravascular absorption can occur when intravesicular pressure exceeds venous pressure, or approximately 15 cm H2O (1.5 kPa). For extravasation to occur through a perforated capsule or bladder neck, intravesicular pressure needs only to exceed the intra-abdominal pressure of approximately 5 cm H2O (0.5 kPa).16,17
FIGURE 33.1 The variety of mechanisms and pathways that lead to transurethral resection of the prostate (TURP) syndrome. The triggering event is the entry of irrigation solution into the intravascular compartment (A) which raises intravascular volume (B) with its sequelae and decreases (C) and/or increases (D) solute concentration. IV, intravenous.
TABLE 33.2 Checklist Used to Define and Score Symptoms in the TURP Syndrome. (Number and Severity of Symptoms Showed a Statistically Significant Increase as More Irrigating Fluid was Absorbed.)
Duration <10 min Duration <5 min Single instance Slight Duration <5 min Patient says so Mildly depressed Mild
Duration > 10 min Duration 5-120 min Repeatedly, <60 min Moderate Duration 5-60 min Objectively exhausted Somnolent <60 min Severe <60 min
Transient blindness Intense or >120 min Repeatedly, >60 min Intense Duration >60 min Exhausted for >120 min Needs ventilator Severe >60 min
TURP, transurethral resection of the prostate; HR, heart rate; SAP, systolic arterial pressure.
From: Hahn RG, Shemais H, Essén P. Glycine 1.0% versus glycine 1.5% as irrigating fluid during transurethral resection of the prostate. Br J Urol. 1997;79:394.
The mode of resectoscope use also plays a role in defining the intravesicular pressure. When the resectoscope is operated with continuous flow, as is favored by many surgeons, less pressure builds in the bladder than when resection is performed using intermittent flow. However, use of a continuous flow resectoscope is no guarantee that intravesicular pressure will remain low; an obstruction to outflow caused by blood clots or tissue chips will make intravesicular pressure rise. Therefore, although the height of the irrigation bag defines the maximum possible intravesicular pressure, no correlation between bag height and fluid absorption has been consistently demonstrated.18,19
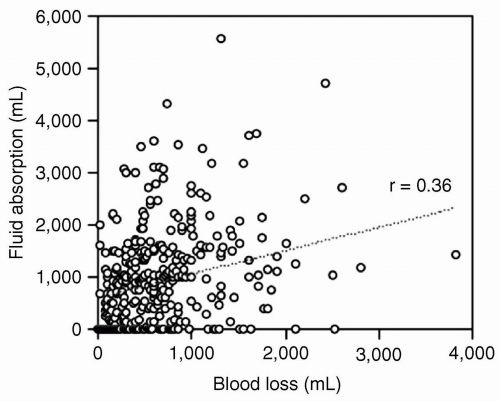
The risk of having fluid absorption during TURP increases slightly with increasing operating time, weight of prostate resected, and blood loss12 (see Fig. 33.2). Surprisingly, the experience of the surgeon has not been validated to be of importance.4,20 Smoking is the only patient factor associated with increased risk for high volume absorption.21 Moreover, antidiuretic hormone produced by the stress of surgery22 and increased renin and aldosterone secretion23 may also contribute to volume expansion by promoting water retention.
Plasma volume expansion from absorbed irrigant can occur rapidly (3.3 L in 20 minutes)24 during TURP and likely contributes to the hypertension and (reflex) bradycardia often seen.25 Absorption rates can reach 200 mL per minute.12 A patient with poor left ventricular function may develop pulmonary edema when challenged with such an acute circulatory volume overload.26 A report of five patients with severe TURP syndrome (two deaths, two seizures, and one ventricular arrhythmia) found “no significant variations” in serum osmolalities before and after TURP,27 suggesting that intravascular volume changes independent of osmolality can play an important role in the morbidity and mortality associated with the TURP syndrome.
FIGURE 33.2 Poor relationship between blood loss and fluid absorption in 817 patients undergoing TURP. The risk of having fluid absorption is increased in prolonged and bloody operations (data from Ekengren J, Hahn RG. Blood loss during transurethral resection of the prostate as measured by the HemoCue photometer. Scand J Urol Nephrol. 1993;27:501.), but the relationship is not very strong (unpublished data).
▪ DETECTION
Early detection of fluid absorption opens the possibility to arrest further absorption and avoid the TURP syndrome, either by stopping surgery or by keeping the fluid pressure low by applying a bladder pressure device. The earliest possible treatment of fluid absorption can also be started. Classically, an awake patient undergoing TURP with regional anesthesia serves as his own “miner’s canary” for early detection of absorption. The severity and number of complaints worsen as the absorbed volume increases. Complaints associated with increasing intravascular absorption include “feeling bad,” nausea, hypotension, and chest pain. Extravasated fluid in the retroperitoneal or peritoneal space provokes shoulder, back and chest pain, abdominal discomfort and distension, and shortness of breath. Altered mental status, irritability, bradycardia, and hypotension are more serious and are typically later signs of increasing absorption. These complaints and observations may emerge subtly or dramatically. Many mild forms of the TURP syndrome probably go unrecognized. Moderate-sized absorptions typically only give rise to symptoms 30 to 60 minutes after surgery.28 If patients are to be protected from the TURP syndrome, effective and early means of quantifying absorption in patients under general anesthesia and in awake, but asymptomatic, patients is required.
The TURP syndrome has been reported to occur as quickly as 15 minutes from surgical start.24,29 Reliable detection of such a rapid onset would be best achieved, ideally, with a continuous method for monitoring absorption. If only intermittent monitoring methods are available, sampling intervals should preferably not exceed 15 minutes during resection.
Serum Sodium
A common method for detection of acute volume gain of an electrolyte-free solution is serum sodium measurement.24 A decreased serum sodium concentration is indicative of the absorption of sodium-free irrigation fluid. This method has the advantage of being widely available. Its disadvantages are that it is cumbersome to obtain serial blood samples free of intravenous fluid contamination, and a delay between collecting a sample and receiving the laboratory results may result. Furthermore, because of its slow intravascular absorption, it may take 2 to 4 hours following extravasation of fluid before the decreased serum sodium concentration can be measured.30 At present, bedside testing is possible (i-STAT, Abbott Laboratories. Abbott Park, Illinois), and blood samples can be analyzed for serum sodium at intervals less than every 5 minutes, if desired. This approach will be useless for detecting absorption if an isotonic electrolyte irrigation solution is used, because no change in serum sodium would be expected, regardless of the volume of fluid absorbed.
Breath Alcohol Levels
Measurement of breath alcohol levels is an inexpensive and a simple method of monitoring irrigant absorption. Glycine 1.5% mixed with ethanol 1% is an irrigation solution (Baxter Healthcare Ltd, Thetford, Norfolk, England) made for this purpose, and is available in some countries.31 Ethanol has also been added to mannitol and sorbitol solutions32 and can be utilized in isotonic electrolyte solutions. The technique does require the use of a breathalyzer to intermittently (every 5 to 10 minutes) measure breath alcohol levels. Absorption has occurred when the breathalyzer detects any alcohol in the exhaled breath. This technique identifies intravascular absorption exceeding approximately 150 mL over 10 minutes. An estimate of the volume absorbed intravascularly can be made from the breathalyzer value by using a published nomogram.33 When fluid containing ethanol 1% is extravasated, a 15- to 20-minute delay can be expected before the breathalyzer measures any tracer.30 Although 2% ethanol is more sensitive for detecting absorption, its use increases the possibility of intoxication when larger volumes are absorbed. Ethanol, in any concentration, may not be the preferred absorption tracer if the patient is a recovering alcoholic. To avoid all potential toxicity and make the monitoring fully automatic, recent clinical trials have added tracer doses of nitrous oxide to irrigating fluid and closely monitored the patient’s breath.34
Volumetric Fluid Balance
Calculation of volumetric fluid balance31 is another method of assessing fluid absorption. Operating room staff track the volume of irrigant used and compare this to the volume recovered from the surgical field. The difference represents the maximum volume absorbed. The technique is simple but often inaccurate because of the incomplete recovery of irrigant, discrepancies in labeled and actual irrigant bag volumes, and inaccurate calibrations in the collection container. Estimates of blood and urine losses must also be added to the collected volume, which further compromise the accuracy of this method. The volumetric balance measures the sum of intravascular absorption and extravasation and does not make a distinction between them.
Gravimetry
Gravimetry follows the patient’s weight gain during the procedure.35,36 With an operating table capable of weighing the patient, weight gain can be used to measure volume gain (1 kg weight gain = 1 L fluid gain). However, sources of nonsurgical weight gain or loss, such as intravenous therapy or hemorrhage or tissue loss, must be estimated and decrease the accuracy of this method. Gravimetry and volumetric methods for measurement of absorbed fluid volume occur in real time and are not compromised or delayed by increasing the proportions of extravasated fluid.
Miscellaneous Techniques
Also described but never widely adopted has been monitoring the trends of the central venous pressure,37 plasma electrolyte concentrations (e.g., magnesium and calcium),38 irrigation solute concentration (glycine39,40 and sorbitol41), and transthoracic impedance.42
Prevention
The principal strategies for reducing the incidence and severity of the TURP syndrome focus on reducing the three factors generally believed to be the most significant variables influencing absorption: (i) The magnitude of the intravesicular fluid pressure; (ii) the number of prostatic venous and surgical perforation openings for fluid to gain entrance; and (iii) the duration of high-pressure fluid exposure to open veins or the retroperitoneal space.
Intravesicular pressure is generally lowest when a trocar, suprapubic drainage catheter, or a continuous flow resectoscope is in use. Limiting irrigation fluid height further defines the maximum intraoperative bladder pressure that can occur. Restricting surgery time to 1 hour and leaving a rim of tissue on the capsule until near the end of the procedure where it can either be left (if signs of TURP syndrome are evident) or removed all at once have been advocated as ways to reduce the time that a large number of prostatic sinuses are open and capable of absorbing fluid.10,43
Other efforts have attempted to limit the absorption of irrigation fluid or blood loss through pharmacologic means rather than further limiting absorption by redesigning instruments or procedural techniques. Vasopressin, a potent vasoconstrictor, injected into the prostate before TURP has been advocated as a possible way to limit absorption of the irrigant.44 These authors reported that insignificant absorption occurred among a series of 36 patients who, after transrectal injection of vasopressin (10 units) into the prostate, underwent TURP, with water as the irrigation fluid. Premedication for 4 weeks with chlormadinone acetate, an orally administered antiandrogen, or a 3-month course of finasteride, a 5-reductase inhibitor that lowers dihydrotestosterone and angiogenesis, have also been reported to significantly reduce the blood loss per gram of resected tissue.7
▪ INTRAVASCULAR VOLUME CONTRACTION
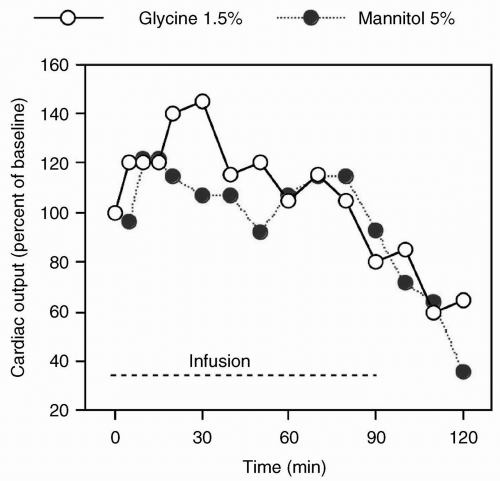
It is counterintuitive that a volume-overloaded condition will lead to hypotension. However, in the TURP syndrome, hypotension is a common feature and may even be the presenting symptom. Hahn reported 12 patients who had intravascular absorption of more than 1 L of isotonic irrigant during a TURP procedure.25 After the first 20 minutes of the procedure, the patients were hypervolemic and hypertensive, and central venous pressures had increased. After 30 to 35 minutes, when the rate of irrigant absorption slowed, flow from the plasma to the interstitium increased to an average of 75 mL per minute. Three patients then became suddenly hypotensive (systolic arterial blood pressure of 80 mm Hg or less) and, of these, two became hypotensive again after the procedure. Three other patients suddenly became hypotensive within the first postoperative hour. A similar effect has been demonstrated in animal studies45 (see Fig. 33.3).
There are several paths by which the acute fluid absorption and hypervolemia that initiate the syndrome can progress to a prolonged and potentially profound hypotension. Severe hyponatremia by itself does not account for the hypotension.46,47 However, hypervolemia, which produces a dilution of serum electrolytes and proteins that manifests as hyponatremia, hypocalcemia, and low serum osmolality, combined with hypertension, may lead to a dramatic water flux along osmotic and hydrostatic pressure gradients out of the intravascular space.28 Together, these factors may be sufficient to impair cardiac function. Moreover, studies in mice and pigs indicate that a severe volume overload damages the heart by causing severe interstitial dilatation, hypoxic changes, and disruption of the histoskeleton.45,48,49 Any cardiac compromise will only be further aggravated by other conditions that can accompany symptomatic fluid gain in a patient: High sympathetic blockade induced by regional anesthesia, liberation of cellular potassium, or acidosis. Pulmonary edema and hypovolemic shock develop when fluid translocates into the lungs and other tissues.
FIGURE 33.3 Hypokinetic circulation after prolonged administration of irrigating fluid. Cardiac output during and after a 90-minute intravenous infusion of 100 mL/kg/hour of either glycine 1.5% or mannitol 5% in 17 pigs (mean values). After the infusions, the mean arterial pressure decreased by 20%. (Data derived from: Sandfeldt L, Riddez L, Rajs J, et al. High-dose intravenous infusion of urological irrigating fluids containing glycine and mannitol in the pig. J Surg Res. 2001;95:114.)
The TURP syndrome may develop and progress over several hours, depending on the volume and distribution of fluid absorption between the intravascular spaces and intra- and retroperitoneal spaces. The rate of progression may be hastened by the release of prostatic endotoxins. Despite routine antibiotic prophylaxis and negative preoperative urine cultures, endotoxemia can develop in up to 45% of patients during TURP.50 Although usually manifesting postoperatively, signs of sepsis have presented intraoperatively.50,51 The recommendation is to treat patients with preoperative bacteria for several days before undertaking elective TURP.
Bleeding and red blood cell destruction are additional sources of volume and oxygen-carrying capacity losses that may further stress the heart. Absorption of distilled water during TURP can cause acute hypoosmolality with massive hemolysis.52 The hemoglobinemia that follows such hemolysis, coupled with hypotension, can cause acute renal failure, and even death.53,54 The same mechanism may also cause permanent renal damage in response to extravasation of distilled water.55 In general, extravasation has a higher tendency than direct intravascular absorption to cause arterial hypotension.2
▪ ELECTROLYTE-FREE IRRIGATION SOLUTIONS
Distilled Water
Distilled water was the original irrigation used for TURP.54 Without ionic solutes, distilled water provided the best viewing field and resectoscope performance. Electrolyte-free water did not disperse the electric cutting current of the resectoscope and produced the least optical refraction. Its osmolality of zero reduced turbidity and maintained a clear visual field by hemolyzing red cells that had bled into the bladder during resection.
Water is said to have several additional advantages over nonhemolytic solutions and may still enjoy a resurgence of popularity if the claims that new techniques reduce absorption are substantiated. Without dissolved solutes, water provides more stable hemodynamics by rapidly diffusing out of the intravascular compartment into the interstitial compartment and, by the same mechanism, produces less hyponatremia.56,57 The clinical validity of these “benefits” is dubious, as the consequences of diffusion of free water into brain and lungs, for example, are undesirable and serious. Hence, if distilled water must be used, it should be restricted for use with smaller resections or with techniques known not to cause massive absorption. However, where procedural costs are a significant concern, water remains the least expensive and perhaps the only choice.57 When water is to be used, the considerable risks to the patient need to be acknowledged and awareness of clinical events must not wane.58
Complications arising from intravascular absorption that included intravascular hemolysis, renal failure and death led to the introduction and wide acceptance of new nonhemolyzing irrigation solutions. Glycine, sorbitol, and mannitol are electrically nonconductive, but osmotically active solutes, that were added to irrigation fluids and reduced the occurrence of significant hemolysis and death by more than 50%.59,60
Nonhemolytic Irrigation Solutions
The nonhemolytic irrigation solutions (and calculated osmolalities) most often employed with the traditional monopolar resectoscopes include glycine 1.5% (200 mOsm per L), sorbitol 3% (165 mOsm per L or 170 mOsm per kg), sorbitol 2.5% with 0.54% mannitol (167 mOsm per L), sorbitol 5% and mannitol 5% (275 mOsm per L), and dextrose 5% (252 mOsm per L). The osmolality reported on the irrigant bag liners is calculated and assumes there are no interactions between solute particles. Because these interactions do occur, a solution’s measured osmolarity will be slightly lower (10 to 20 mOsm per L) than the calculated osmolarity value.
These osmolarities are generally hypotonic compared with lactated Ringer’s solution (273 mOsm per L) and 0.9% normal saline (308 mOsm per L) that are used with bipolar resectoscopes. Although the osmotic activity of the irrigation solutions is reported as osmolarity, a measure of the osmoles per liter of solution, it is conventional to refer to serum osmotic activity as osmolarity, a measure of the osmoles per kilogram of solvent (water). When the concentration of solute is very low, as is the case for electrolytes in serum, osmolarity and osmolality become nearly the same, and the terms are often used interchangeably.
What Are the Plasma Solute Effects Associated with the Transurethral Resection of the Prostate Syndrome?
Solute changes occurring during and after TURP may alter the patient’s condition and neurologic function independently of the volume-related effects (see Table 33.3). Most notably, central nervous system (CNS) symptoms associated with TURP have been attributed to the metabolic derangements of hyponatremia, hypoosmolality, hyperammonemia, and hyperglycinemia. The choices made for anesthetic interventions can further impair the neurologic status and complicate the diagnosis of TURP syndrome. The superimposition of centrally active drugs, such as propofol, benzodiazepines and narcotics,24 or a spinal anesthetic causing hypotension that leads to nausea and vomiting, can confuse the clinical picture and delay the diagnosis.
TABLE 33.3 Changes in Neurologic Function during TURP Can be Triggered by One or More of the Listed Factors
TURP, transurethral resection of the prostate; CNS, central nervous system.
▪ HYPONATREMIA
Profound hyponatremia with TURP has been implicated as the cause of visual aberrations, encephalopathy, pulmonary edema, cardiovascular collapse, seizure, and death.61,62 The rate of irrigant absorption ranges from 10 to 30 mL per minute of resection time.63 However, the intravascular absorption rate alone can exceed 200 mL per minute.12 The incidence of serum sodium concentration <125 mEq per L following TURP may reach 10%43 with a mortality of symptomatic hyponatremia (headache, nausea, vomiting) of approximately 40%.64 The intravascular absorption of irrigant from the perivesicular and retroperitoneal spaces may continue for up to 24 hours after surgery.13 The TURP syndrome may develop at any time while absorption continues.43,65,66,67
Dilutional hyponatremia may be aggravated by two other mechanisms. Electrolytes diffuse from the extracellular fluid space to any accumulation of extravasated nonelectrolyte fluid.2 If the patient is given diuretic medication, additional electrolytes will be lost in the urine.23,38,46,68,69 Diuretics have been implicated as factors for the rapid onset of hyponatremia.68 When used routinely or to treat hypervolemia following TURP, diuretics may worsen hypoosmolality and provoke hypotension42 (see Fig. 33.4). Diuretics acting on the ascending loop of Henle have an onset within 2 to 5 minutes. They inhibit chloride uptake, causing urinary sodium loss, and promote salt-wasting after TURP.15,23,38 Mannitol also wastes sodium during the first 12 hours following TURP.70 Therefore, if loop or other salt-wasting diuretics are used to treat hypervolemia, strong consideration should be given to a concomitant infusion of saline—even in the presence of near-normal serum sodium concentrations—during the first 12 postoperative hours.15,23
Only gold members can continue reading. Log In or Register to continue