A 64-year-old, 72-kg man is seen at the local emergency department for a 3-day history of hematemesis and dark stools. The patient has a past medical history of heavy alcohol intake and bleeding from esophageal varices. On arrival, the patient is noted to be mildly dehydrated, confused, markedly tachycardic, and hypotensive. He is also complaining of new onset of chest tightness associated with vomiting. A 12-lead electrocardiogram reveals marked ST depressions in the anterior lead and sinus tachycardia. During initial evaluation, approximately 250 mL of bright red blood emesis was noted. Hematocrit at this time was reported at 29%. A large bore intravenous site was accessed, and aggressive fluid resuscitation was begun by rapid infusion of 2 L of normal saline and 500 mL of 5% albumin. Elective endotracheal intubation was achieved for airway protection and impending endoscopic sclerotherapy. Hematocrit was noted to be 18% and platelet count 25,000 per mm3 following fluid resuscitation. Borderline hypotension and subtle ST changes persist in all anterior leads despite improving hypotension and tachycardia. The patient was transfused with three units of packed red blood cells (PRBCs) and one unit of platelets, with marked improvement in hemodynamic, electrocardiogram, and laboratory values. Following initial hemodynamic resuscitation, the patient underwent successful therapeutic endoscopy for definite treatment of active variceal hemorrhage under general endotracheal anesthesia. Cardiology workup revealed undiagnosed coronary artery disease, thereby explaining the ST changes in the presence of hypotension and severe acute anemia.
What Is Perioperative Anemia?
The occurrence of anemia in the surgical population has long attracted the interest of the anesthesia, surgical, and critical care communities. Its presence has been identified as an independent risk factor for infection, requirement for transfusion,1,2,3 and increased perioperative morbidity and mortality.4,5,6 However, the lack of a consistent and standard definition of what constitutes anemia has limited the interpretation and comparison of available data, and complicates the reporting of definitive anemia prevalence in the perioperative setting. An attempt to establish a numeric definition of the lower limit of normal hemoglobin was recently reported.7 The values are derived from two large, well documented databases—The Third US National Health (and Nutritional Examination Survey and the Scripps-Kaiser database) that allow the exclusion of individuals who are not “normal.” This analysis concludes that a hemoglobin level below 13.7 g per dL, in a white man between 20 and 60 years of age, has approximately a 5% chance of being a normal value. The corresponding value of hemoglobin in women of all ages is 12.2 g per dL (see Table 34.1). These values differ slightly from the widely accepted values proposed by the World Health Organization (WHO) that were published in 1968.8 The WHO defines anemia as a hemoglobin of <13 g per dL in adult males and <12 g per dL in adult nonpregnant females. These small but significant numeric discrepancies confound the true prevalence of anemia in the general population and suggest that a single numeric value to diagnose clinical anemia is difficult to establish. Therefore, a more individualized and physiologic approach to the management of anemia and hemoglobin levels in patient care is a reasonable goal.
TABLE 34.1 Proposed Lower Limits of Normal Hemoglobin Concentration of the Blood for White and Black Adults
Group
Hemoglobin (g/dL)
White Men
20-59 y
13.7
≥60 y
13.2
White Women
20-49 y
12.2
≥50 y
12.2
Black Men
20-59 y
12.9
≥60 y
12.7
Black Women
20-49 y
11.5
≥50 y
11.5
From: Beutler E, Waalen J. The definition of anemia: What is the lower limit of normal of the blood hemoglobin concentration? Blood. 2006;107:1747.
What Is the Clinical Definition of Acute Anemia?
The clinical definition of anemia has been widely accepted more as a functional than numeric definition. Because the oxygen-carrying capacity is determined by the mass of circulating red cells, anemia can be defined as a condition characterized by a decrease in the oxygen-carrying capacity of the blood resulting from decreased red blood cell (RBC) mass.9 Because RBC mass is not easily measured in the clinical setting, the clinical definition of anemia has been based on the determination of hematocrit and the hemoglobin concentration in whole blood. Normal values for hemoglobin and hematocrit vary dramatically with environmental conditions, age, and gender.
Examples of physiologic RBC mass variation can be appreciated in the neonatal period, where normal hemoglobin levels are between 14 and 20 g per dL. These hemoglobin concentrations decrease during the second to third month of life, to reach a nadir of 10 to 11 g per dL, and then rise to stabilize at approximately 12 g per dL. These changes represent a normal physiologic decrease in erythropoiesis and a decreased erythocyte lifespan during this period. In the geriatric population, anemia, as defined by the WHO, was found in 17% of women and in 28% of men aged 85 years and older.10 In this study, the authors concluded that the mortality risk was increased in this population and that anemia in the older person is due to disease and not to normal aging.
Therefore, perioperative anemia needs to be evaluated on an individual basis, taking into account the patient’s age, gender, medical condition, analysis of risk factors, and the current surgical scenario. The functional consequences of anemia are far more relevant in clinical anesthesia than the simplicity of a laboratory value.
Acute anemia may result from a sudden drop in the hemoglobin or hematocrit due to hemolysis, acute hemodilution, or acute blood loss. In all instances, the amount of plasma volume present in blood influences the hematocrit and hemoglobin concentration. It is possible for an individual to be severely anemic and yet have a normal hematocrit. This often occurs in the presence of acute hemorrhage, where rapid loss of intravascular volume entails the simultaneous loss of RBCs and plasma. Following a sudden loss of 20% of total blood volume, 20 to 60 hours are required to restore a normal blood volume by endogenous plasma replacement.11,12 The decrease in RBC mass, or anemia, does not become clinically apparent until fluid replacement therapy or endogenous compensatory mechanisms reestablish normal blood volume. On the contrary, it is also possible to have laboratory evidence of anemia without clinical evidence of disease; this is due to the ability of the body to compensate for decreased RBC mass in chronic situations.
What Is the Prevalence and Clinical Outcome of Perioperative Anemia?
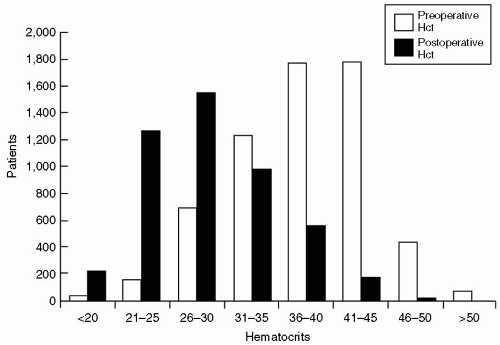
Anemia is a frequent finding in the surgical population. Clinical studies have consistently shown a relatively high prevalence of this condition in the perioperative surgical population.13 Dunne et al. reported preoperative anemia (hematocrit <36%) in 33.9% of patients, and postoperative anemia in 84.1% of patients in a very large sample size of 6,301 noncardiac surgical patients (see Fig. 34.1).4 They concluded that a low perioperative hematocrit and the use of blood transfusions were found to be significant independent predictors of postoperative pneumonia, increased hospital length of stay, and mortality.
In the perioperative situation, acute anemia is most commonly related to acute blood loss during surgery. The combination of hypovolemia and reduced oxygen-carrying capacity may induce anemic hypoxia and cellular hypoxia during acute blood loss. Certain risk factors are known to increase the risk of adverse consequences in the presence of anemia. Heart, lung, kidney, and cerebrovascular disease pose special considerations in the presence of surgical procedures with a high risk of blood loss. The inability to maintain or increase oxygen delivery in the face of increased demand may result in myocardial ischemia and congestive heart failure, renal failure, and central nervous system ischemia.
FIGURE 34.1 Population distribution of preoperative and postoperative hematocrits. Preoperative anemia was present in 2,127 (33.9%) patients. Postoperative anemia was more common and present in 4,016 (84.1%) patients. Hct, hematocrit. (From: Dunne JR, Malone D, Tracy JK, et al. Perioperative anemia: An independent risk factor for infection, mortality, and resource utilization in surgery. J Surg Res. 2002;102:237.)
The heart is exquisitely prone to injury in the presence of anemia. In the resting individual, the myocardial muscle extracts 70% to 75% of the oxygen delivered through the coronary circulation. Myocardial oxygen extraction cannot increase above resting levels in the presence of higher oxygen demand. Consequently, higher oxygen delivery must be achieved by increasing coronary blood flow.
Transient and asymptomatic changes in the electrocardiogram, reversible changes in cognition, and fatigue have been reported in normal individuals during induced isovolemic anemia with hemoglobin levels between 5 and 7 g per dL.14,15,16 Moreover, in older patients (>85 years) and critically ill patients, the presence of anemia is associated with an increased number of blood transfusions, diminished organ function, and increased mortality.10,17
What Are the Causes and Differential Diagnosis of Anemia?
Assuming that the circulatory system is intact, a decrease in RBC mass, or anemia, results from an imbalance in the mechanisms responsible for RBC production and destruction. The degree to which the signs and symptoms of anemia are manifest depends upon the magnitude and speed of the reduction in RBC mass, volume of fluid loss, if any, and the individual’s ability to compensate. Table 34.2 provides a classification of the causes of acute and chronic anemia.
Normal RBC survival is approximately 120 days. Erythrocytes progress from blast precursors in the bone marrow over a period of 5 days. They are then released into the circulation in the form of reticulocytes (immature erythrocytes), maturing in 1 day and circulating for an average of 120 days before being destroyed by the reticuloendothelial system. All the by-products of the catabolism of RBCs remain available for reutilization in cases of physiologic destruction or hemolytic anemia, as contrasted with acute blood loss in which RBCs are lost as a whole.
Mechanisms responsible for acute anemia are limited to those related to excessive red cell destruction (hemolytic anemia), acute blood loss, and iatrogenic dilutional anemia. There are disorders such as iron deficiency anemia, which results from inadequate iron intake or chronic bleeding, and deficiency of vitamin B12 and folic acid that manifest as a chronic inability of the bone marrow to increase red cell production beyond the rate of red cell destruction. However, because of the time that it takes for chronic anemia to develop, compensatory mechanisms such as increases in 2,3-diphosphoglycerate (2,3-DPG) in the RBCs facilitate oxygen unloading in the tissue and mask clinical symptoms. On the contrary, acute anemias such as hemolytic anemia, acute hemorrhage, and acute hemodilution rapidly trigger a reflex sympathetic response that augments (cardiac output) CO and forces a blood flow redistribution in the body until more chronic and effective compensatory mechanisms become established.
Acute anemia related to blood loss is common in the perioperative setting. The clinical response to decreased blood volume becomes more notorious as blood loss becomes more severe. During severe hemorrhage, the restoration of intravascular volume with colloids or crystalloids outweighs the physiologic importance of decreased red cell mass. Once the intravascular volume has normalized, signs of acute dilutional anemia may present.
TABLE 34.2 Causes of Anemia
Hemorrhagic
Acute Blood Loss
External
Internal
Chronic Blood Loss
Hemolytic
Acute Hemolysis
(Inherited or Acquired)
Extravascular
Intravascular
Chronic Hemolysis
Membrane defects
Metabolic defects
Hemoglobin disorders
Environmental causes
Impaired
Red Cell Maturation Disorders
Production
Cytoplastic defects
Severe iron deficiency
Thalassemia
Sideroblastic anemia
Nuclear defects
Folate deficiency
Vitamin B12 deficiency
Other marrow diseases
Hypoproliferative Disorders
Iron deficiency
Inflammation
Reduced erythropoietin
Marrow damage
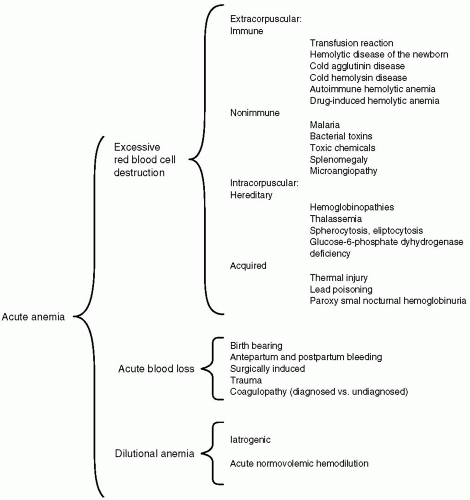
Acute anemia resulting from excessive red cell destruction can occur by one of two mechanisms: Abnormalities within the RBC and/or its membrane (intracorpuscular) or abnormalities in the environment of the RBC (extracorpuscular). Therapeutic strategies and morbidity differ, depending on the etiology. All hemoglobinopathies, hereditary or acquired, cause intracorpuscular hemolysis. Extracorpuscular hemolytic disorders may be classified as immune or nonimmune, depending on the circumstance or agent that triggers the hemolytic reaction. Nonimmune causes of hemolytic anemia are diverse and include drugs, bacterial toxins, chemicals, parasites, and a long list of diseases responsible for microangipathic hemolytic anemia. Figure 34.2 details the causes of acute anemia.
What Are the Clinical Manifestations of Acute Anemia?
Acute anemia is often difficult to diagnose. Signs and symptoms related to decreased RBC mass may become evident when the hematocrit falls rapidly below 35% or in the presence of acute blood loss. Clinical signs of acute blood loss correlate well with the percentage of total-body blood volume loss (see Table 34.3).18 A normal individual can rapidly lose 10% to 20% of blood volume without signs or symptoms of anemia. However, a rapid blood loss of more than 50% of total blood volume presents with clinical signs of severe hypovolemic shock and death.
In patients with slow, chronic blood loss, compensatory mechanisms allow for more dramatic losses of RBCs with minimal clinical signs of anemia. Chronic reestablishment and maintenance of intravascular volume limit the cardiovascular response to hypovolemia. However, signs of decreased total RBC mass may ensue.
In general, clinical signs of blood loss anemia are tachycardia, orthostatic and resting hypotension, and evidence of reduced end organ perfusion, manifested by altered mental status and decreased urine output. In healthy subjects, symptoms produced by bleeding may become apparent when the hematocrit falls below 35%. These symptoms include mild fatigue, palpitations, dyspnea, excessive sweating with exercise, and a requirement for an increased amount of sleep.11
In the case of acute anemia due to hemolysis, intravascular volume is intact and the clinical signs and symptoms are directly related to anemia. Clinical signs of hemolytic anemia are pallor, jaundice, tachycardia, a new systolic ejection murmur, and dark colored urine. Symptoms include marked fatigue, dizziness, and palpitations.
What Is the Body’s Response to Acute Anemia?
In acute anemia, a variety of physiologic adjustments attempt to maintain tissue oxygen delivery despite a decrease in oxygen-carrying capacity. The basic adjustments include an increase in CO in direct proportion to the severity of anemia under normovolemic conditions, and inversely related to the percentage of total blood loss in acute blood loss anemia. Other important adaptive changes include a shift in the oxyhemoglobin dissociation curve to the right and a reduction in blood viscosity, thereby improving microcirculatory mechanics.
The cardiovascular adjustments that take place during acute blood loss anemia are the result of an increase in sympathetic nervous activity and a decrease in blood viscosity. The absolute loss of intravascular volume produces a fall in systemic arterial blood pressure and systemic venous return—as a consequence, end-diastolic volume and CO drop. These changes increase reflex sympathetic nerve activity and elicit an increase in heart rate and contractility that elevate CO towards normal. When blood loss exceeds 30% to 40% of the blood volume, there is a distinct fall of CO and the onset of shock. In this situation, the increased sympathetic tone diverts the limited CO away from the splanchnic, skeletal, and cutaneous circulation toward the more vital coronary and cerebral circulations. This manifests as refractory hypotension, acute renal failure, changes in mental status, and myocardial ischemia. The rate at which the blood loss occurs heavily influences the magnitude of the compensatory mechanism in acute blood loss anemia.
FIGURE 34.2 Causes of acute anemia.
With acute blood loss, an absolute decrease in the RBC count will occur; however, hematocrit or hemoglobin will not immediately reflect the quantity of blood loss. With more subtle and chronic blood loss, sufficient restoration of plasma volume ensues and a marked decrease in RBC count is seen in the face of minimal cardiovascular response due to maintenance of intravascular volume.
CO also increases with increasing degrees of normovolemic anemia. In fact, an inverse relation has been established between hemoglobin level and CO during normovolemic anemia.19,20 The main mechanisms responsible for increases in CO during normovolemic anemia are reduced blood viscosity and increased sympathetic stimulation.21 In this condition, the increase in CO is primarily the result of an increase in stroke volume rather than an increase in heart rate. The latter is responsible for the increase in CO associated with hypovolemic anemia. The reduction in the blood viscosity seen at the postcapillary venule with moderate normovolemic anemia results in increased venous return to the heart and increased CO. Early canine studies demonstrated that lowering blood viscosity with a colloid exchange-transfusion to a target of half the normal hematocrit dramatically increased CO, compared to dogs whose effective hemoglobin was halved by exchange-transfusion with RBCs containing methemoglobin.22 This explains the increase of total and local blood flow as a compensatory response to preserve oxygen delivery as long as normovolemia is preserved.
In the presence of low hemoglobin/hematocrit and stable hemodynamics, optimal oxygen delivery and uptake are of primary concern. There is a unique relation between oxygen consumption ([V with dot above]O2), tissue blood flow, and the extraction of oxygen from the blood (arterial-venous oxygen difference). The Fick principle states that oxygen consumption ([V with dot above]O2) is equal to the product of flow and the arteriovenous oxygen content difference (CaO2 – CvO2).
TABLE 34.3 Signs and Symptoms of Acute Blood Loss of Increasing Severity
Percentage of Total Blood Volume
mL in 70-kg Man
Clinical Signs
10
500
None; rare vasovagal syncope
20
1,000
Usually none at rest; slight orthostatic hypotension and tachycardia with activity
30
1,500
Anxiety and restlessness; flat neck veins; tachycardia and resting hypotension possible
40
2,000
Cold, clammy skin; rapid, thready pulse; air hunger possible; CVP, cardiac output, and arterial blood pressure below normal at rest
50
2,500
Hypovolemic shock; diaphoresis; disorientation or decreased consciousness; death
CVP, central venous pressure.
Data from: Hillman RS, Hershko C. Acute blood loss anemia. In: Beutler E, Lichtman MA, Coller BS, et al. eds. Williams hematology, 6th ed. Philadelphia: McGraw-Hill; 2001:677.
Only gold members can continue reading. Log In or Register to continue