A 55-year-old, 80 kg, intravenous drug user was scheduled for an incision and drainage of a right shoulder abscess. He had a longstanding history of asthma and had been hospitalized several times in the past for acute exacerbations of his asthma. He had a small meal 3 hours before the surgery. He received an intravenous dose of hydrocortisone and nebulized albuterol in the emergency department.
On physical examination, he was sitting upright, had sternal retractions and dyspnea with bilateral diffuse wheezing. His right arm, including the axilla and upper chest, were swollen and inflamed. Laboratory tests showed a serum bicarbonate of 35 mmol per L and a normal electrolyte panel. A chest radiograph showed subcutaneous air in the distribution of the abscess and hyperinflated lung fields bilaterally.
A rapid sequence induction was performed using ketamine and vecuronium. The trachea was intubated and the lungs ventilated with 4% sevoflurane in oxygen, with a tidal volume of 600 mL and an inspiratory to expiratory time ratio (I:E) of 1:4. Bilateral diffuse wheezing was unchanged. His peak inspiratory pressure was 36 cm H2O, and the end-tidal CO2 was 48, with a prolonged upslope on the capnograph. Shortly thereafter, the peak inspiratory pressure increased to 60 cm H2O with concomitant hypotension. Auscultation revealed a silent chest. Intravenous boluses of ephedrine were titrated to restore the blood pressure, while anesthesia was deepened with boluses of ketamine, 40 mg. Sevoflurane was continued in an inspired concentration of 3% to 4%. The bronchospasm resolved during the next few minutes.
At the end of the procedure, glycopyrrolate and neostigmine were administered slowly over 15 minutes while the patient was deeply anesthetized. A large bore gastric tube was then passed, and stomach contents were suctioned out. The trachea was extubated and the patient observed in a left lateral position, applying cricoid pressure until he was conscious. Intravenous hydrocortisone and albuterol nebulizers were continued postoperatively and tapered over the next few days. He was discharged 4 days later.
What Baseline Knowledge Is Relevant?
▪ PHYSIOLOGY OF BRONCHOMOTOR TONE
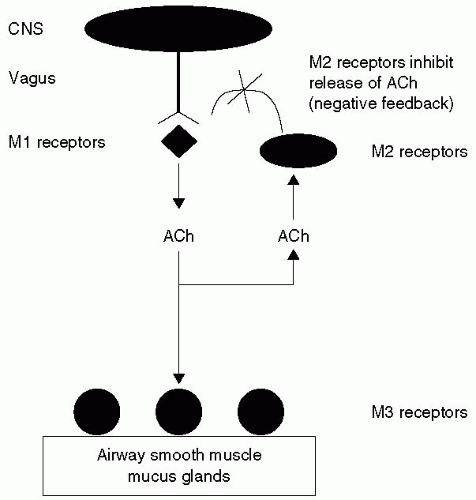
The walls of bronchi and bronchioles are composed mainly of smooth muscle and cartilage plates. The smooth muscle bundles encircle the airways obliquely from the trachea down to the alveolar ducts. Contraction of these results in both narrowing and shortening of the airway. The parasympathetic nervous system is the dominant neuronal pathway that controls the airway smooth muscle tone. Postganglionic parasympathetic fibers innervate the airway smooth muscle down to the level of the terminal bronchioles. Stimulation of the cholinergic nerves causes bronchoconstriction, mucus secretion, and bronchial vasodilation. Irritant receptors are found just beneath the tight junctions of the epithelial lining of the airway. The afferent and efferent connections of these receptors travel through the vagus nerve. Acetylcholine administered exogenously or released from parasympathetic postganglionic nerves induces airway constriction by activating M3 muscarinic receptors on airway smooth muscle (see Fig. 9.1). At rest, the normal human airways have a mild baseline constriction due to vagal activity, which can be blocked by anticholinergic agents such as atropine, glycopyrrolate, or ipratropium.1,2 This resting bronchomotor tone is believed to serve three different purposes: (i) To provide a balance between anatomic dead space and airway resistance, and hence optimize the work of breathing and gas exchange;3 (ii) prevent collapse of the larger cartilaginous bronchi during coughing; and, (iii) minimize the collapse of smaller noncartilaginous bronchi at low lung volumes. Sympathetic nerves may control tracheobronchial blood vessels, but no sympathetic innervation of human airway smooth muscle has been demonstrated. β-Adrenergic receptors, however, are abundantly expressed on human airway smooth muscle, and activation of these receptors causes bronchodilation. Although circulating β2 active endogenous catecholamines can activate the receptors, the physiological role of the β-adrenergic receptors is unclear.4 Inhibitory, nonadrenergic noncholinergic (NANC) nerves containing vasoactive intestinal peptide and nitric oxide may be the only neural bronchodilator pathway in the human airways.
FIGURE 9.1 Muscarinic receptors (M1, M2, M3) in the respiratory system. CNS, central nervous system; Ach, Acetylcholine.
▪ PATHOPHYSIOLOGY OF REACTIVE AIRWAY DISEASE
Although abnormalities of the cholinergic system have been suggested in asthma, thus far, the evidence for cholinergic dysfunction in asthmatic subjects is not convincing.4 Although the dysfunction of inhibitory NANC nerves has also been proposed in asthma, no NANC abnormalities have been demonstrated in asthmatics. In animal studies, stimulation of excitatory NANC nerves caused bronchoconstriction, mucus secretion, vascular hyperpermeability, cough, and vasodilation; a process called neurogenic inflammation.4 Excitatory NANC nerves, extensively studied in animal airways, have also been detected in human airways. Recent studies have demonstrated an interaction between the excitatory NANC nervous system and inflammatory cells. The functional relevance of the excitatory NANC nervous system and its interaction with the immune system in asthma still remains to be elucidated.
What Are the Differences Between Chronic Obstructive Pulmonary Disease and Asthma?
Perioperative bronchospasm is frequently, but not exclusively, encountered in patients with reactive airway disease, most of which include those with asthma, chronic obstructive pulmonary disease (COPD), and bronchopulmonary dysphasia. Although varying degrees of expiratory airflow limitation and bronchospasm are features of asthma and COPD, there are some fundamental pathophysiologic and clinical differences between the two. These are summarized in Table 9.1 and briefly discussed in the following text.
▪ ASTHMA
Asthma affects 5% to 10% of the population in the United States. The prevalence rate of exercise-induced asthma is 12% to 15% of the general population. Up to 50% to 90% of asthmatics may experience exercise-induced symptoms. Recent data suggest an increase in both the prevalence and morbidity associated with asthma, especially in children younger than 6 years. Factors responsible include urbanization, air pollution, passive smoking, and change in exposure to environmental allergens.
The pathophysiology of asthma is complex and involves the following components: (i) Airway inflammation, (ii) intermittent airflow obstruction, and (iii) bronchial hyperresponsiveness. Airway edema, mucus secretion, smooth muscle hyperplasia, acute bronchoconstriction, and airway remodeling also contribute to airflow obstruction and bronchial reactivity. The presence of airway hyperresponsiveness in asthma is an exaggerated response to numerous exogenous and endogenous stimuli. The mechanisms involved include direct stimulation of airway smooth muscle and indirect stimulation by pharmacologically active substances from mediator-secreting cells, such as mast cells or nonmyelinated sensory neurons.
The pathogenesis of exercise-induced asthma is poorly understood. It may be mediated by either water loss or heat loss from the airway, or a combination of both. The upper airway normally humidifies and warms the inspired air to 100% humidity and body temperature. The nose is unable to heat and humidify the increased amount of air required for exercise, particularly in athletes who mouth-breathe. The abnormal heat and water fluxes in the tracheobronchial tree result in bronchoconstriction, occurring within minutes of completing exercise. Results from bronchoalveolar lavage studies have not demonstrated an increase in inflammatory mediators.
There are no published studies on exercise-induced asthma as a risk factor for perioperative bronchospasm, but it seems safe to assume that these patients are likely at increased risk.
TABLE 9.1 Differences Between Chronic Obstructive Pulmonary Disease (COPD) and Asthma
Asthma
COPD
Characteristic
Age at onset
Younger (often during childhood)
Older (age >40 y)
Allergic etiology
Allergies present in >50% of patients
None
Smoking status
Nonsmokers affected
Usually history of heavy smoking
Treatment Response
Bronchodilators
Reversible
Partial reversibility
Corticosteroids
Good
Poor
Airflow limitation (FEV1)
Can normalize after resolution of episode
Cannot normalize; always reduced; deterioriates with advancing disease
Pathology
Airways
All
Central (bronchitis)
Peripheral (emphysema)
Parenchyma
Not involved
Destruction
Airway hyperresponsiveness
Present
May or may not be present
Bronchial smooth muscle
Enlarged mass in large airways
Enlarged mass in small airways
Epithelium
Shedding
Metaplasia
Mucus secretion
Present
Present, heavy
Goals of Therapy
Risk factors
Reduce exposure
Reduce exposure
Symptoms
Control
Relief
Pulmonary function/airflow limitation
Maintain normal or close-to-normal pulmonary function; prevent development of irreversible airflow limitation
Prevent progression of pulmonary dysfunction
Activity and exercise
Maintain normal levels of activity and exercise
Improve exercise tolerance (strength, endurance)
Exacerbations
Prevent and treat
Prevent and treat
Drug related adverse event
Avoid
Avoid
Disease related mortality
Prevent
Reduce
FEV1, forced expiratory volume in 1 s. Data from Workshop Report, Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease, September 2005. Global Initiative for Chronic Obstructive Lung Disease. Available at: http://www.goldcopd.org/Guidelineitem.asp?l1=2&l2=1&intld=989. Last accessed November 14, 2005. and Global strategy for asthma management and prevention, 2005. Available at: http://www.ginasthma.org/Guidelineitem.asp??l1=2&l2=1&intld=60. Last accessed November 15, 2005.
▪ CHRONIC OBSTRUCTIVE PULMONARY DISEASE
COPD is defined as a disease state characterized by the presence of airflow obstruction due to chronic bronchitis or emphysema that is generally progressive—and not fully reversible—and may be accompanied by airway hyperreactivity and an abnormal inflammatory response of the lungs.5 COPD, generally, is secondary to tobacco use; less frequently, cystic fibrosis, α-1 antitrypsin deficiency, and bronchiectasis cause similar conditions. Chronic bronchitis is defined clinically as the presence of a chronic productive cough for 3 months during each of 2 consecutive years (other causes of cough being excluded). Emphysema is defined as an abnormal, permanent enlargement of the air spaces distal to the terminal bronchioles, accompanied by destruction of their walls and without obvious fibrosis. In the United States, roughly 14.2 million people have COPD, of whom 12.5 million have chronic bronchitis and 1.7 million have emphysema. It has been estimated that the prevalence of chronic airflow obstruction in the United States is 8% to 17% for men and 10% to 19% for women.
Pathophysiologic changes characteristic of COPD include mucus hypersecretion, ciliary dysfunction, airflow limitation, pulmonary hyperinflation, gas exchange abnormalities, pulmonary hypertension, and cor pulmonale—and they usually develop in this order over the course of the disease.5 The airflow limitation characteristic of COPD is that it is primarily irreversible, with a small reversible component. The irreversible component of airflow limitation is primarily because of remodeling—that is, fibrosis and narrowing—of the small airways that produces fixed airways obstruction and a consequent increase in airways resistance. The sites of airflow limitation in COPD are the smaller conducting airways, including bronchi and bronchioles <2 mm in internal diameter. Loss of elastic recoil and alveolar support to maintain the patency of small airways, secondary to alveolar parenchymal destruction, also contributes to the irreversible airflow obstruction. More importantly for the anesthesiologist, airway smooth muscle contraction, ongoing airway inflammation, and intraluminal accumulation of mucus and plasma exudate may be responsible for the small part of airflow limitation that is reversible with treatment, especially during acute exacerbations.
The role of hypoxic pulmonary drive is often overemphasized in patients with severe COPD. Oxygen therapy is generally safe in patients with COPD. Although oxygen toxicity from high-inspired concentrations (Fio2 >0.6) is well recognized, little is known about the long-term effects of low flow oxygen. The British Medical Research Council (MRC) study and the National Heart, Lung, Blood Institutes Nocturnal Oxygen Therapy Trial (NOTT) study found that long-term oxygen therapy improves survival in patients with hypoxemia and COPD twofold or more.6 Hypoxemia in these trials was defined as a Pao2 of <55 mm Hg, or Sao2 <90%. Supplemental oxygen was used from 15 to 19 hours per day. The increased survival and quality-of-life benefits of long-term oxygen therapy outweigh the possible risks. The increase in PACO2 in patients with COPD who are on oxygen therapy is more likely a consequence of ventilation/perfusion mismatching rather than respiratory center depression. Although respiratory center depression as a result of blunting of hypoxic ventilatory drive with oxygen therapy is not common, it is best avoided by titration of oxygen delivery to maintain a PaO2 at 60 to 75 mm Hg or SaO2 in the 90% to 94% range.
Patients with COPD may present for COPD-related surgical procedures such as bullectomy, lung volume reduction, lung transplantation, or elective or emergency procedures that are not related to COPD.
Which Pharmacological Agents Are Relevant for the Treatment of Reactive Airway Disease?
▪ β AGONISTS
The predominant airway smooth muscle receptor is the β2-adrenergic receptor. β Agonists combine with the receptors and cause an increase in intracellular cyclic adenosine3′, 5′—monophosphate (cAMP)—which activates protein kinases, decreases intracellular levels of calcium, and, in turn, causes airway smooth muscle relaxation and inhibits the release of mediators from the mast cells.
Intravenous β agonists such as isoproterenol can cause serious ventricular arrhythmias and myocardial damage when administered intravenously. Selective β2-adrenergic agents, such as terbutaline or albuterol, are equally effective when administered by inhaled or intravenous routes, and some studies suggest greater efficacy by the inhaled route.
Albuterol is the most commonly used β2 agonist. It is occasionally administered orally as a 2 to 4 mg per dose, every 6 to 8 hours; but more commonly by a metered dose inhaler that delivers approximately 100 μg per puff. The usual dose is one to two puffs every 4 to 6 hours, not to exceed 12 puffs per 24 hours; it can also be wet-nebulized in a dose of 2.5 to 5 mg every 4 to 6 hours. Albuterol and terbutaline are short-acting β2 agonists with a duration of action of 4 to 6 hours, whereas long-acting agents such as salmeterol and formoterol have a duration of action exceeding 12 hours. The longer-acting drugs are used primarily for prophylaxis rather than rescue therapy.
▪ STEROIDS
Anti-inflammatory medication remains the preferred treatment for chronic asthma and prevention of acute exacerbations of asthma. The mechanism of action of steroids is not fully understood but is dependent on the binding of the steroids to cytosolic receptors that translocate to the nucleus to affect gene transcription/translation. Hence, any beneficial effects have a typical lag time of at least 6 to 8 hours. The anti-inflammatory effects of glucocorticoids include decreased inflammatory cell influx, a reduction in the release of mast cell mediators (and reduced mast cell numbers), and decreased microvascular leakage, and hence airway edema. Inhaled corticosteroids used in asthma include beclomethasone, budesonide, flunisolide, fluticasone, and triamcinolone. Although intravenous hydrocortisone (4 mg per kg) may be used in an urgent setting, such as in the patient discussed in our case summary, elective preoperative patients may benefit from a course of methylprednisone started 3 to 5 days before surgery.
Given the low morbidity of a short course of steroids, it is prudent to ensure that asthmatics who are not fully controlled receive a burst of steroids preoperatively. Similarly, any suggestion of intraoperative or postoperative wheezing may justify their use.
▪ MAST CELL STABILIZERS
Cromolyn inhibits the degranulation of sensitized mast cells following exposure to specific antigens. It attenuates the bronchospasm caused by exercise, cold air, aspirin, and environmental pollutants, but is of little use for acute episodes of bronchoconstriction.
▪ ANTICHOLINERGICS
Anticholinergic drugs compete with acetylcholine for postganglionic muscarinic receptors, thereby inhibiting cholinergically mediated bronchomotor tone, resulting in bronchodilatation. They block vagally mediated reflex arcs that cause bronchoconstriction. Treatment with aerosolized anticholinergic agents (e.g., ipratropium bromide and tiotropium) may be more effective than a β2 agonist in patients with COPD. Ipratropium bromide has bronchodilatory activity with minimal adverse effects and is administered by a metered dose inhaler. Studies in patients with stable COPD have shown that ipratropium bromide has equivalent or superior activity when compared with a β2 agonist. In combination with a β2 agonist, an additional 20% to 40% bronchodilation occurs. Ipratropium has a slower onset (e.g., 30 to 60 minutes) and longer duration than a β2 agonist and is less suitable for use on an as-needed basis.
▪ METHYLXANTHINES
Aminophylline and theophylline were extensively used in the 1970s and 1980s for their bronchodilating properties. The popularity of methylxanthines has decreased during the last decade because of the narrow therapeutic range, large variation in interindividual pharmacokinetics, and frequent toxicity. The mechanisms of beneficial action may involve increased intracellular calcium transport, adenosine antagonism, and prostaglandin E2 inhibition. Additionally, methylxanthines may improve diaphragm muscle contractility. The target blood level is 10 μg per mL, and toxic concentration is >20 μg per mL. Many drugs, including alcohol, β-blockers, cimetidine, and macrolide antibiotics and quinolones (including erythromycin, clarithromycin, ciprofloxacin) decrease aminophylline clearance, thereby raising serum levels and the potential for increased toxicity. Other agents such as phenytoin, rifampicin, and tobacco and marijuana smoking may increase the clearance of aminophylline, thereby decreasing serum concentrations, risking subtherapeutic dosing. Toxicity may present in the form of cardiovascular manifestations such as tachycardia, palpitations, extrasystole, flushing, hypotension, circulatory failure, atrial and ventricular arrhythmia, or central nervous system (CNS) manifestations such as headache, irritability, anxiety, tremor, dizziness, hyperexcitability, and seizures (our patient presented with toxic serum levels, atrial fibrillation and seizures).
There is no evidence that outcome from an acute asthmatic attack is improved if theophylline is added to a regimen of β agonists and steroids, and the potential toxicity is significant.
▪ INTRAVENOUS ANESTHETIC AGENTS
Among anesthetic induction agents, considerable experimental evidence suggests that ketamine has both direct and indirect relaxant effects on airway smooth muscle through non-β-receptor mechanisms.7 However, the clinical data supporting the use of ketamine for the prevention or treatment of bronchospasm is largely anecdotal, and in more rigorous trials, unimpressive.8 This could be due to the reluctance to routinely use ketamine at the high doses needed to produce bronchodilatation because of side effects such as dysphoria, hallucinations, increased secretions, and sympathetic stimulation), rather than a lack of benefit of the drug.
Propofol, midazolam, and etomidate all relax airway smooth muscle in vitro,9,10 whereas barbiturates may have direct bronchoconstricting effects.9 Propofol may also have indirect effects on airway constriction, perhaps through inhibition of vagal tone. Clinically, propofol has been shown to be superior to the barbiturates and etomidate in reducing wheezing and airway resistance in both asthmatic and nonasthmatic subjects.11,12,13 In asthmatics induced with either thiopental, methohexital, or propofol at equipotent doses, none wheezed following tracheal intubation when propofol was used, whereas both of the barbiturates resulted in a significant incidence of wheezing.13 In the patient described in this chapter, ketamine had the advantage of vasomotor stability in the presence of intravascular volume depletion.
▪ HALOGENATED HYDROCARBONS (VOLATILE ANESTHETICS)
All of the volatile anesthetics have direct, and perhaps indirect, relaxant effects on airway smooth muscle in experimental models.14 Although differences in the potency of these agents are present in vitro, the clinical importance of these differences is unclear. Sevoflurane is more effective than isoflurane, desflurane, and halothane in reducing airway resistance after endotracheal intubation in patients,15 but does not prevent an increase in airway resistance after intubation of asthmatic children.16 A study showed that while sevoflurane and isoflurane cause a dose-dependent bronchodilatation, desflurane decreases airway resistance at 1 MAC, but causes an increase in airway resistance at 2 MAC.17 There are no prospective, controlled studies comparing deep inhalation anesthesia to intravenous induction with bronchoprotective agents such as ketamine or propofol in high-risk patients.
Only gold members can continue reading. Log In or Register to continue