I. INDICATIONS FOR TRANSFUSION THERAPY. Blood component transfusion is usually performed because of decreased production, increased utilization/destruction or loss, or dysfunction of a specific blood component (red cells, platelets, or coagulation factors).
A. Anemia
1. Red cell mass. The primary reason for red blood cell transfusion is to maintain an adequate oxygen-carrying capacity of the blood. Healthy individuals or individuals with chronic anemia can usually tolerate a hematocrtit (Hct) of 20% to 25%, assuming normal intravascular volume. The Hct assumes red blood cell normocytosis and appropriate hemoglobin (Hgb) content. A patient with hypochromic normocytic anemia may have an Hct within normal range but a decreased oxygen-carrying capacity. For this reason, many institutions use Hgb (g/dL) in lieu of Hct (%) as an indicator of red blood cell mass. Modern techniques assay total red cell Hgb and the red blood cell count to calculate the Hct instead of measuring the packed cell volume by centrifugation.
2. Anemia may be caused by decreased production (marrow suppression), increased loss (hemorrhage), or destruction (hemolysis). Acute blood loss generally does not change the relative concentration of red blood cells immediately (as other intravascular volume is lost at the same rate), but the infusion of intravenous fluid may contribute to a dilutional effect.
3. Anemia in critically ill adults is common. The exact Hgb level that should prompt red blood cell transfusion may be different for various scenarios, but even among a homogenous population remains controversial. Results from the two largest randomized controlled trials of critically ill patients suggest that a “restrictive” transfusion policy improves hospital survival when compared with a more liberal transfusion strategy (maintaining Hgb 7–9 g/dL vs. 10–12 g/dL in one study, Hct ≥24% vs. ≥30% in the other). Another large randomized trial of patients after hip fracture with a history of or risk factors for cardiovascular disease showed no reduction in death or functional outcome with a Hb target of >10 versus >8 g/dL.
4. Estimating the volume of blood to transfuse can be calculated as follows:
Volume to transfuse = (Hctdesired – Hctpresent) × BV/Hcttransfused bood
where BV is blood volume, which may be estimated at 70 mL/kg actual body weight in male adults and 65 mL/kg in female adults. Higher values may be used in infants (80 mL/kg) and neonates (85 mL/kg). The Hct of transfused blood is approximately 70 ± 5%.
B. Thrombocytopenia. Spontaneous bleeding is unusual with platelet counts more than 5,000 to 10,000 per µL, but in the immediate postoperative period, platelet counts of more than 20,000 to 50,000 are sometimes recommended. Thrombocytopenia may be due to decreased bone marrow production (e.g., chemotherapy, tumor infiltration, or alcoholism) or increased consumption (e.g., trauma, sepsis, drug effects like histamine-2 antagonists or ticarcillin, or immune-mediated reactions like idiopathic thrombocytopenic purpura or heparin-induced thrombocytopenia). A relative deficiency of platelets may also be caused by large volume intravenous infusions or red blood cell transfusions.
II. BLOOD TYPING AND CROSS-MATCHING
Donor blood and recipient blood are typed in the red cell surface ABO and Rh systems and screened for antibodies to other cell antigens. Cross-matching involves directly mixing the patient’s plasma with the donor’s red cells to establish that hemolysis does not occur from any undetected antibodies.
A. An individual’s red cells have either A, B, both (type AB), or neither (type O) ABO-type surface antigens. If a person’s red cells are lacking either A or B surface antigen, then antibodies will be produced against it. Consequently, a person with type B red blood cells will have anti-A antibodies in the serum, while a type O individual, that is, a person having neither A nor B surface antigens will have circulating anti-A and anti-B antibodies. Conversely, a person who has type AB red blood cells will not have antibodies to either A or B, thus can receive red blood cells from a person of any blood type (universal recipient). Type O blood has neither A nor B surface antigens, and a person with this blood type is a universal red cell donor.
B. Rh Surface Antigens are either present (Rh-positive) or absent (Rh-negative). Individuals who are Rh-negative will develop antibodies to the Rh factor when exposed to Rh-positive blood. This is not a problem with the initial exposure, but hemolysis will occur due to the circulating antibodies with subsequent exposures. This can be particularly problematic during pregnancy. The anti-Rh antibodies are immunoglobulin (IgG) and freely cross the placenta. In Rh-negative mothers who have developed Rh antibodies, these antibodies are transmitted to the fetus. If the fetus is Rh-positive, massive hemolysis will occur, termed hemolytic disease of the newborn. Rh-immune globulin, an Rh-blocking antibody, prevents the Rh-negative patient from developing anti-Rh antibodies. Rh-immune globulin is routinely administered to Rh-negative women when possible exposure to Rh surface antigens occurs (e.g., disruption of the placenta with an Rh-positive fetus). Rh-immune globulin should be considered for all Rh-negative individuals who receive Rh-positive blood, especially women of childbearing age. The recommendation is one dose (approximately 300 µg/vial) for every 15 mL of Rh-positive blood transfused.
III. BLOOD COMPONENT THERAPY
A. Whole Blood
1. Whole blood has been largely replaced by component therapy because of storage impediments and no demonstrable superiority of the former. The exceptions may be for children younger than 2 years undergoing complicated cardiovascular surgery, exchange transfusions, where whole blood may have an outcome benefit in reduced transfusions, and during warfare due to limited storage capacity and availability of healthy donors.
2. Whole blood must be ABO and Rh identical because transfusion includes antibodies from the donor.
B. Red Blood Cells
1. Packed red blood cells (pRBCs) contain concentrated ABO-specific red blood cells from a single donor. One unit (typically containing 250–300 mL) can be expected to raise the Hb of a euvolemic adult by approximately 1 g/dL once equilibration has taken place.
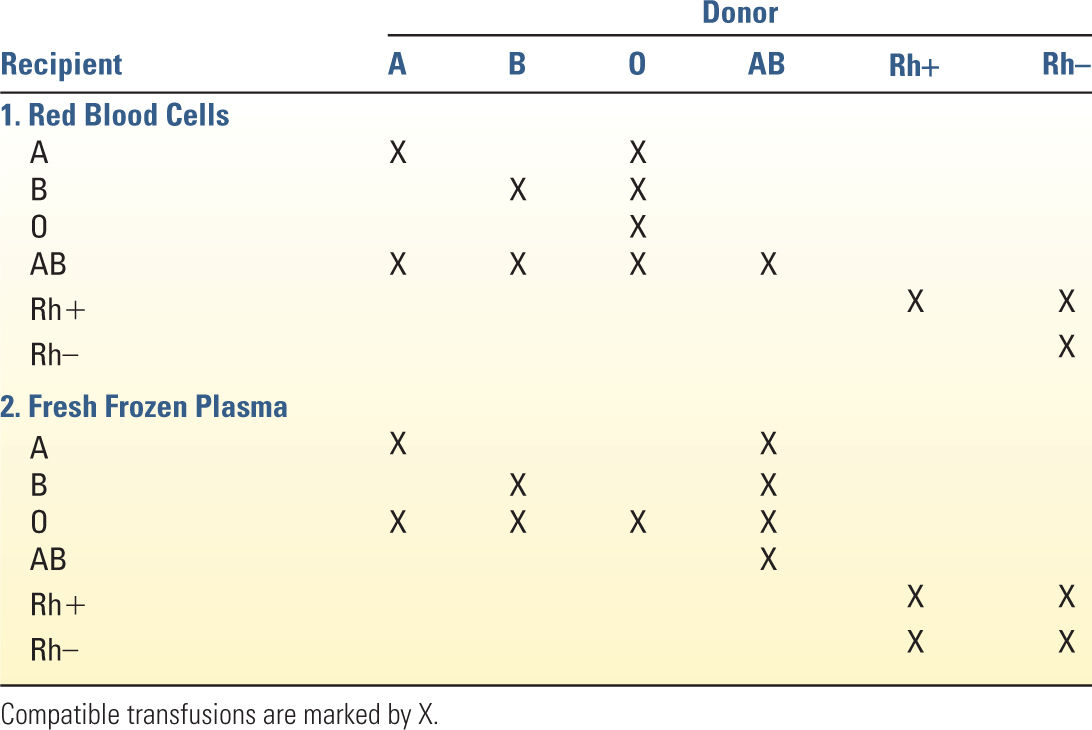
2. pRBCs must be ABO compatible (Table 35.1). If an emergency blood transfusion is needed, type-specific (ABO) red cells can usually be obtained within minutes if the patient’s blood type is known. If type-specific blood is unavailable, type O red cells may be transfused. Rh-positive blood may be transfused to Rh-negative individuals in some situations and may be accompanied by Rh-immune globulin. Type-specific blood should be substituted as soon as possible to conserve resources and minimize the amount of type O plasma (containing anti-A and anti-B antibodies) transfused.
C. Platelets
1. One unit of random donor platelets contains approximately 1011 platelets and 60 mL of plasma from a single donor. These are typically grouped into “pools” of 4 to 6 units (often called a “6-pack”), from random or single donors. Each unit of platelets is expected to increase the platelet count by 5,000 to 10,000 per µL. If thrombocytopenia is due to increased destruction (e.g., due to the presence of antiplatelet antibodies), platelet transfusions will be less efficacious. A posttransfusion platelet count drawn 10 minutes after completion of platelet transfusion confirms platelet refractoriness if the count fails to increase by 5,000/µL for each unit transfused (30,000 µL for a 6-unit pool).
2. ABO-compatible platelets are not required for transfusion, although they may provide a better response as measured by the posttransfusion platelet count. Single-donor platelets are obtained from one individual by platelet pheresis. Single-donor platelets may be used to reduce exposure to multiple donors or in cases of poor response to random donor platelets where destruction is suspected. In cases where alloimmunization causes platelet refractoriness, HLA-matched platelets may be required for effective platelet transfusion. Rh-negative women of childbearing age should receive Rh-negative platelets if possible because some RBCs and plasma are transfused with platelets. If this is impossible, Rh-immune globulin may be considered.
D. Fresh Frozen Plasma (FFP) is the liquid portion of blood after the red blood cells and platelets have been removed. It contains primarily coagulation factors and immunoglobulins and is generally filtered to remove white blood cells. One unit is approximately 220 to 250 mL.
1. Factors V and VIII are most labile and quickly become depleted in thawed FFP. A typical dose of 10 to 20 mL/kg will increase plasma coagulation factors by about 20%. Fibrinogen levels increase by 1 mg/mL of plasma transfused.
2. Acute reversal of warfarin generally requires 5 to 8 mL/kg of FFP. It is important to note that the International Normalized Ratio (INR) of FFP is approximately 1.6, so infusion of FFP alone is unlikely to lower a patient’s INR below this level.
3. ABO-compatible FFP transfusion is required (Table 35.1), but Rh-negative patients may receive Rh-positive FFP.
4. Six units of platelets (one pool) contain the equivalent of one unit of FFP.
E. Cryoprecipitate is formed by cold precipitation and centrifugation of FFP. Each unit is approximately 15 mL and is typically provided in pools of 6 to 10 units.
1. Each unit of cryoprecipitate typically contains 80 units of factor VIII and approximately 200 to 300 mg of fibrinogen. It also contains factor XIII, von Willebrand factor, and fibronectin.
2. Indications for cryoprecipitate include hypofibrinogenemia, von Willebrand disease, hemophilia A (when factor VIII is unavailable), and preparation of fibrin glue (although commercially available virally inactivated concentrates have a higher fibrinogen concentration and are preferred for this purpose). One unit/7–10 kg raises the plasma fibrinogen concentration by approximately 50 mg/dL in a patient without massive bleeding.
3. ABO compatibility is not required for transfusion of cryoprecipitate, but it is preferred because of the presence of 10 to 20 mL of plasma per unit.
F. Factor Concentrates. Individual coagulation factors are available for patients with discrete factor deficiencies. These may be derived from pooled human plasma or synthesized by recombinant gene technology.
1. Activated recombinant factor VII (rFVIIa) was originally developed to control bleeding in patients with hemophilia A or B who had developed circulating inhibitors to factors VIII and IX. Subsequently, rFVIIa has been used to treat hemorrhage related to trauma, disseminated intravascular coagulation (DIC), intracranial hemorrhage, and perioperative bleeding. rFVIIa is thought to facilitate local coagulation by complexing with a tissue factor after endothelial injury and subsequent stimulation of the coagulation cascade. It has a half-life of approximately 2 hours and is very expensive. Current evidence supports only a very limited role for factor VIIa in massively bleeding patients. It should be considered only in carefully selected patients with diffuse coagulopathy (as opposed to a surgically correctable source of hemorrhage) who fail to respond to conventional component therapy, and its administration should be governed by an institutional protocol.
G. Technical Considerations
1. Compatible infusions. Many transfusion guidelines recommend avoiding coinfusion of pRBC with solutions other than normal saline. Dextrose-containing solutions may contribute to hemolysis, although this has not been demonstrated (Keir, 2014). Infusion with lactated Ringer’s (LR) carries a theoretical concern of inappropriately activating clotting, but this has not been demonstrated either (Lorenzo 1998). Sodium chloride, albumin, and FFP are all compatible with pRBC.
2. Blood filters (80 µm) should be used for all blood components except platelets to remove debris and microaggregates. Leukocyte filters may be used to remove white blood cells to prevent transmission of cytomegalovirus in the immunocompromised, to prevent alloimmunization to foreign leukocyte antigens, and to diminish the incidence of febrile reactions. Platelets should be transfused through a 170-µm blood filter.
IV. SYNTHETIC BLOOD SUBSTITUTES
Blood product availability is limited and stored products maintain their integrity for a limited time. They continue to carry risks for infection and other adverse events (see Section VII), and some cultures have an aversion to homologous blood transfusion (e.g., Jehovah’s Witnesses). Oxygen-carrying blood substitutes are being developed, and used in other countries, with some success. Primarily, these materials are hemoglobin-based oxygen carriers (HBOC) and perfluorocarbon-based oxygen carriers (PFBOC). Unfortunately, none are able to completely replicate the complex functions and efficiency of human red blood cells, but they may serve as a useful adjunct, particularly in areas with limited resources.
There are several products in clinical trials in the United States and Europe, a few available for veterinary use, but none currently available for clinical use in humans in the United States.
V. PHARMACOLOGIC THERAPY
A. Erythropoietin is an endogenous hormone that stimulates proliferation and development of erythroid precursor cells. Exogenous administration has been used to correct anemia in patients with chronic renal failure and to increase red cell mass prior to preoperative autologous donation. Current evidence does not support the routine administration of erythropoietin for critically ill patients. It may be considered for the severely anemic patient who refuses blood transfusion. Iron and folate supplementation are also recommended for patients receiving erythropoietin. Initial recommended doses in renal failure patients range from 50 to 100 units/kg IV or SQ three times a week.
B. Granulocyte Colony-Stimulating Factor (GCSF) and Granulocyte-Macrophage Colony-Stimulating Factor (GMCSF) are myeloid growth factors useful for shortening the duration of neutropenia induced by chemotherapy. GCSF is specific for neutrophils, and GMCSF increases production of neutrophils, macrophages, and eosinophils. Administration of these drugs enhances both neutrophil count and function. As such, they are frequently used for the treatment of febrile neutropenia. Treatment results in an initial brief decrease in the neutrophil count (due to endothelial adherence), then a rapid (usually after 24 hours) sustained leukocytosis that is dose dependent. Recommended doses are GCSF 5 µg/kg/d or GMCSF 250 µg/m2/d until absolute neutrophil count is more than 10,000 mm3.
C. Other interventions to enhance hemostasis are discussed in Chapter 25.
VI. BLOOD CONSERVATION AND SALVAGE TECHNIQUES. Blood transfusion of critically ill patients is common, with approximately 40% of patients being transfused during an ICU stay. Those patients who are older and stay longer in the ICU are more likely to receive a transfusion. Increasing evidence supporting the deleterious effects of homologous blood transfusion in critically ill patients reinforces the importance of techniques to diminish or eliminate the need for blood transfusion.
A. Phlebotomy Losses from critically ill patients can be significant, ranging from 40 to 400 mL/d, with higher losses in surgical units versus medical units. Patients with more severe illness and a greater number of dysfunctional organs suffer higher phlebotomy losses due to a greater number of blood draws. Techniques demonstrated to reduce phlebotomy losses include (a) a “closed” system of blood sampling where the initial aspirated blood is reinjected into the patient instead of discarded, (b) use of small-volume phlebotomy tubes, and (c) “point-of-care” testing at the bedside, which frequently requires less blood than the clinical laboratory. Finally, the presence of both arterial and central venous catheters in critically ill patients is correlated with higher phlebotomy losses, suggesting another reason to repeatedly evaluate the need for such catheters with respect to hemodynamic monitoring or medication/nutritional support administration.
B. Surgical Drain Salvage Devices allow the reinfusion of shed blood. Most commonly used in patients with blood collected from chest tubes, these are useful for reducing homologous transfusions in the immediate postoperative period. Use of these devices requires skilled nursing for proper administration and sterile technique. They are contraindicated in conditions where the drained cavity is infected. A potential danger is hyperkalemia from reinfusion of hemolyzed cells, which may be life threatening.
VII. COMPLICATIONS OF BLOOD TRANSFUSION THERAPY
A. Transfusion Reactions
1. Acute hemolytic transfusion reactions are estimated to occur in 1 in 250,000 transfusions and are usually due to clerical errors. Symptoms include anxiety, agitation, chest pain, flank pain, headache, dyspnea, and chills. Nonspecific signs include fever, hypotension (or cardiovascular collapse), unexplained bleeding (or DIC), and hemoglobinuria (or renal failure). Fatal reactions are estimated at 1 in 1,250,000 units. Table 35.2 describes the steps to be taken if a transfusion reaction is suspected.
2. Nonhemolytic transfusion reactions are usually due to antibodies against donor white cells or plasma proteins. These patients may complain of anxiety, pruritus, or mild dyspnea. Signs include fever, flushing, hives, tachycardia, and mild hypotension. The transfusion should be stopped and a hemolytic transfusion reaction considered (see above).
a. If the reaction is only urticaria, the transfusion should be slowed and antihistamines (diphenhydramine, 25–50 mg IV) or glucocorticoids (hydrocortisone, 50–100 mg IV) may be administered.
b. In patients with known febrile or allergic transfusion reactions, leukocyte-poor red cells (leukocytes removed by filtration or centrifugation) may be given and the patient pretreated with antipyretics (acetaminophen, 650–975 mg) and an antihistamine.
| Treatment of Suspected Acute Hemolytic Transfusion Reaction | |
1. Stop transfusion
2. Send remaining donor blood and fresh patient sample to blood bank for re–cross-match
3. Send patient sample to laboratory for free hemoglobin, haptoglobin, Coombs’ test, DIC screen
4. Treat hypotension with fluids and/or vasopressors as necessary
5. Consider use of corticosteroids
6. Consider measures to preserve renal function and maintain brisk urine output (intravenous fluid, furosemide, mannitol)
7. Monitor patient for DIC
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


