I. INTRODUCTION
A. Overdose, poisonings, and adverse drug reactions are common diagnoses treated by intensivists. According to the Centers for Disease Control (CDC), there was a 102% increase in fatalities from overdoses from 1999 to 2010 in the United States. Many of these poisonings rapidly deteriorate requiring intensive care unit (ICU) admission.
B. The initial approach to a patient with an overdose, poisoning, or adverse drug reaction varies. The American Association of Poison Control Centers is available 24 hours a day to assist—1-800-222-1222. There are also local poison control centers (PCC) that can be called as well. In addition to a thorough history and physical (including tests such as a basic metabolic panel, complete blood count, bedside blood glucose, liver panel, substance specific blood levels, urine toxicological screens, and an electrocardiogram), it is imperative to know the following:
1. What substance, or substances, was used?
2. What time and amount of the substance was taken?
3. What was the route of intake (e.g., ingestion, inhalation, injection, etc.)?
4. What treatment has already been rendered at home by the emergency medical services (EMS) and the emergency department (ED)?
C. While the answers to these questions are being sought, supportive care and stabilization should be initiated. Once the substance and its effects have been identified, additional treatment such as administration of an antidote, enhancing elimination, or decreasing absorption should begin. Activated charcoal in doses of 25 to 100 g for adults (1–2 g/kg) is effective if given within the first hour of ingestion, except when hydrocarbons, metals, and alcohols are ingested. Traditional treatment methods designed to minimize absorption through the GI tract, such as inducing emesis with syrup of ipecac or whole bowel irrigation, are no longer recommended except in specific situations. Similarly, gastric lavage is now out of favor, but can be considered when a known lethal dose of a substance, that does not have an antidote or bind activated charcoal, was ingested within an hour of presentation.
II. DRUG OVERDOSE
A. Drug overdoses can present in a variety of settings, from intentional (e.g., suicide), to unintentional (e.g., child ingesting pills), iatrogenic (e.g., unintentional overdose of acetaminophen from multiple products), and work related (chemical plant exposures).
B. Acetaminophen (APAP) is the leading cause of acute liver failure (ALF) in the United States and was associated with 401 overdose deaths as recently as 2009. As of 2008, because of timely administration of N-acetylcystiene (NAC), the nontransplanted survival rate has increased to 66%.
1. In overdose of APAP, less than 10% of the total dose is needed to develop liver injury. Damage occurs when CYP2E1 metabolizes APAP to the active metabolite, N-acetyl-p-benzoquinone-imine (NAPQI). NAPQI is normally neutralized by glutathione; however, toxicity ensues when NAPQI concentration exceeds that of glutathione. Excess NAPQI binds hepatocyte mitochondrial proteins, which inhibits cellular respiration. This leads to necrosis and apoptosis, ultimately causing ALF.
2. Patients may present without obvious illness, but then rapidly deteriorate to fulminant liver failure within 24 to 96 hours of ingestion, including profound encephalopathy, coagulopathy, hepatorenal syndrome, and metabolic acidosis. Cerebral edema typically develops within 2 weeks, leading to uncal herniation and death. The King’s College Criteria can be used to help predict the need for liver transplantation among patients with ALF from both APAP overdoses, as well as non-APAP ALF as shown in Table 32.1. Please note that there is a modified King’s College Criteria that incorporates lactate to increase the sensitivity (not shown).
3. To determine the severity risk, serum APAP levels are plotted on the Rumack-Matthew nomogram (see Fig 32.1). Ideally, the Tylenol level should be taken and plotted at exactly 4 hours postingestion.
a. NAC should be administered in any of the following circumstances: (1) confirmed lethal toxicity by the Rumack-Matthew nomogram; (2) a confirmed lethal dose of APAP is ingested (>150 mg/kg); (3) the patient is at risk for hepatic injury; or (4) the ingestion time and amount is unknown. Error should be on overtreating with NAC as it is very efficacious with few side effects. Ideally, NAC should be started within 8 hours of ingestion as NAC has a close to 100% success rate in eliminating the need for liver transplantation among APAP overdoses if given within 8 hours. For example, the obtunded overdose patient that had access to Tylenol, but without anyone to corroborate history, should be started on NAC as soon as possible. Though there is an intravenous (IV) form available, NAC is usually administered enterally often via a nasogastric tube. Dosing can be found in Table 32.2.
C. Salicylates are widely available for overdose as it is one of the most popular over-the-counter analgesics and also used routinely in both primary and secondary prevention of cardiovascular disease.
1. Absorption is variable, depending on the amount ingested and if the formulation was enteric coated. Salicylates are absorbed in an ionized form through the stomach and upper intestine and then undergo hydrolysis in the liver, intestinal wall, and erythrocytes before being excreted by the kidneys. The half-life is 2 to 4 hours, but is prolonged to up to 20 hours or longer in high doses or enteric-coated formulation. Levels >30 mg/dL are toxic while >75 mg/dL are lethal causing cerebral edema and cardiac and renal failure.
| King’s College Criteria for Need for Liver Transplantation | |
Tylenol-Associated Acute Liver Failure | Other Causes of Acute Liver Failure |
pH <7.3 | INR >6.5 |
or all of the following: INR >6.5 Creatinine >3.4 mg/dL Grade III–IV encephalopathy | or three of the following: Age <10 or >40 y Non-A or non-B hepatitis or drug reaction >7 d of jaundice before encephalopathy INR >3.5 Serum bilirubin >17.5 mg/dL |
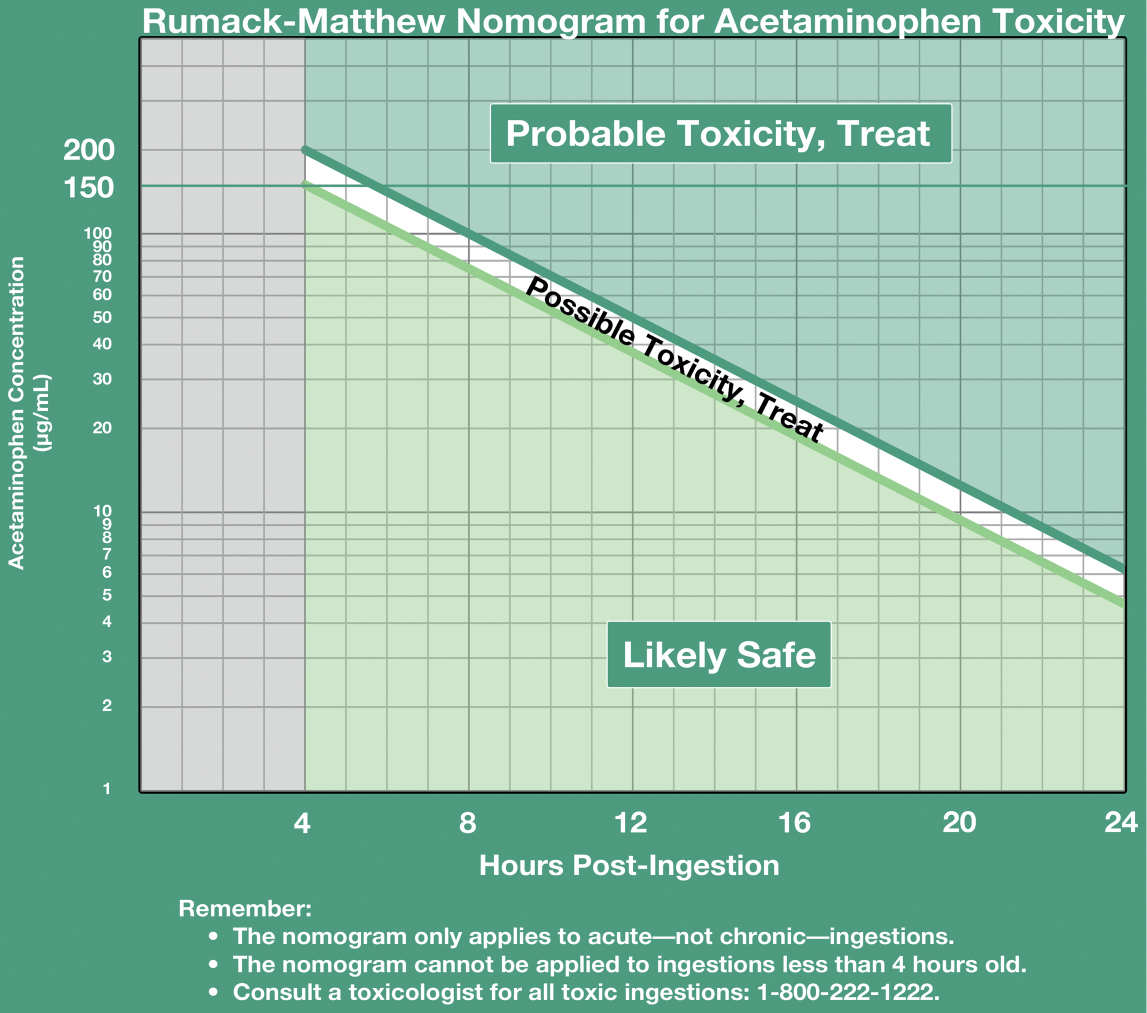
FIGURE 32.1 The Rumack-Matthew nomogram is designed to help determine the risk of hepatotoxicity based on hours since ingestion (x-axis) versus the serum acetaminophen level in mcg/mL (y-axis). Any acetaminophen level greater than the “150-line” at any time since ingestion should be treated with NAC. (Courtesy Graham Walker, MD, Emergency Physician, Kaiser San Francisco, Assistant Clinical Professor, UCSF and MDCalc.com)
| Dosing Regimen for N-acetylcystiene | |
Route | Loading Dose | Additional Doses |
Oral | 140 mg/kg | 70 mg/kg q4h × 17 doses |
Intravenous | 150 mg/kg over 15 min | 50 mg/kg in 4 h, then 100 mg/kg over 16 h |
2. Salicylate toxicity presents with respiratory alkalosis due to CNS excitation, accompanied by tinnitus. Later, metabolic acidosis develops due to uncoupling of oxidative phosphorylation and inhibition of the tricarboxylic acid cycle in the liver. Stupor, coma, and gastrointestinal (GI) bleeding may also be seen.
3. Treatment is primarily supportive. Removal of salicylates is the most important aspect, either through aggressive gastric decontamination and/or early hemodialysis (HD). Indications for HD include severe metabolic acidosis, end-organ damage including seizures, pulmonary edema, acute renal failure, and a serum salicylate level >100 mg/dL. Alkalinization of both the serum and urine has also been shown to improve outcomes. Alkalinizing the serum decreases central nervous system penetration, while alkalinization of the urine improves renal excretion.
D. Cardiovascular drug overdoses, including β-blockers (BB), calcium-channel blockers (CCB), and cardiac glycosides (e.g., digoxin), generated over 50,000 calls to PCC nationally in 2012 and was the second most frequent cause of single-substance-exposure death. With an aging population and the associated increases in prescriptions for cardiovascular drugs, overdoses of these medications are expected to increase in the United States.
1. BB are used for a variety of medical conditions. They work by blocking β-adrenergic receptors, thus decreasing cAMP and decreasing catecholamine effects. This class of medications varies on its specificity for adrenergic receptors. Drugs blocking β1 receptors reduce the inotropic and chronotropic effects on the heart, while drugs blocking β2 receptors reduce bronchodilatation and gluconeogenesis. Drugs such as labetalol and carvedilol also block α1 receptors, which are involved in vasoconstriction.
a. Overdose can result in severe decreases in blood pressure and heart rate as well as hypoglycemia, atrioventricular (AV) block, bronchospasm, and seizures. In overdose, β-selectivity is often lost. If no symptoms are present 6 hours after ingestion, then the patient is cleared; however, sotalol requires a 12-hour period of observation.
b. Initial treatment in overdose includes charcoal, IV fluids, and supporting the heart rate with use of atropine or electrical pacing. Additionally, glucagon, in doses of 50 to 150 mcg/kg bolus followed by a continuous infusion of 2 to 5 mg/h, should be started. Glucagon works by activating adenylate cyclase through direct G-protein stimulation in cardiac tissue. Though less successful, other modalities include direct β agonist such as isoproterenol or amiodarone. Lastly, high-dose insulin therapy has been effective in case reports and is currently under evaluation in animal studies.
2. CCB are commonly used for hypertension, angina, supraventricular arrhythmias, and migraines. CCBs act at voltage-gated calcium channels in myocardial cells, smooth muscle cells, and β-islet cells in the pancreas during phase 2 of the action potential, thus reducing calcium entry. Dihydropyridines (e.g., amlodipine and nicardipine), act peripherally and reduce afterload, while nondihydropyridines (e.g., verapamil and diltiazem) act within the heart, reducing inotropy and chronotropy. In the pancreas, they decrease insulin secretion.
a. Overdose presents with hypotension, sinus bradycardia, AV block, and hyperglycemia. Hyperglycemia and decreased insulin secretion causes the body to convert to fatty acid oxidation, ultimately leading to metabolic acidosis.
b. Like with BB overdose, initial treatment aims at elimination through charcoal therapy, IV fluids, and cardiovascular support. Previous treatment modalities have included calcium, glucagon, epinephrine, and amiodarone. High-dose insulin therapy is also showing promise due to improved carbohydrate metabolism, which leads to improved cardiac function. Initial insulin dosing is 0.5 to 1 unit/kg/h. Insulin should be administered with a dextrose-containing fluid, an epinephrine infusion starting at 1 µg/min, and calcium supplementation.
3. Digoxin is still used for the treatment of atrial fibrillation and congestive heart failure. While overall use is declining, there is still an incidence rate of 48 digoxin-related admissions per 100,000 prescriptions. Digoxin is a sodium–potassium ATPase that increases intracellular sodium, leading to increased calcium and improved inotropy. Toxicity can occur with normal serum digoxin levels in the setting of hypokalemia, hypomagnesemia, or hypothyroidism. Conversely, serum digoxin levels can increase while on a stable dose if drugs such as amiodarone, verapamil, or erythromycin are coadministered.
a. Toxicity leads to increased automaticity and dysrhythmias, including frequent premature ventricular contractions (PVCs), atrial fibrillation with slow ventricular response, or complete AV block. The classic “Salvadore Dali mustache” finding on ECG (ST depression) may be seen, but is not indicative of overdose. Other symptoms include gastric distress, anorexia, and visual halos.
b.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


