A 21-year-old, 95-kg, pharmacy student falls from the third floor balcony of his apartment house while trying to retrieve his neighbor’s keys. When the Emergency Medical Services personnel respond to his residence, he is found to be awake and alert, but unable to move his arms and legs. Oxygen by face mask is applied, and he is carefully placed on a “spine board” with a cervical collar and transported via ambulance. In the emergency department, he is noted to have complete motor and sensory loss below C5, a blood pressure of 85/50 mmHg, heart rate of 46 beats per minute, respiratory rate of 22 breaths per minute, and O2 saturation reading of 95% by pulse oximetry. A 30 mg per kg intravenous bolus of methylprednisolone is initiated, followed by an infusion of 5.4 mg/kg/hour for 23 hours. Cervical spine radiographs reveal subluxation of C5 on C6 with ligamentous instability. The patient is placed in 10 lb of traction that reduces the misalignment of the spinal elements. He is admitted to the intensive care unit (ICU) and receives supplemental oxygen. Forced vital capacity measurements are performed three times daily, and he is scheduled in the operating room for cervical spine stabilization the following day. In the operating room, he is cooperative and receives careful sedation and topicalization for an awake fiberoptic intubation. An arterial line is placed in his radial artery, and the intraoperative mean arterial pressure is maintained at 85 to 90 mmHg. The patient is extubated following the procedure, and returns to the ICU for additional monitoring. He is transferred to a rehabilitation center 5 days after his initial injury.
What Baseline Knowledge Is Relevant?
▪ TRAUMATIC SPINAL CORD INJURY
The average age of a patient with an acute spinal cord injury (SCI) is 32.3 years, and the typical victim is a young, adult man involved in a motor vehicle accident or fall. The most frequent level of traumatic injury in adults is C5-C6, corresponding to the area of greatest cervical spine mobility. Upper cervical spine injuries and the problem of a severe ligamentous injury without radiographic abnormalities (SCIWORA) are more likely in young children.1 The incidence of SCI in patients who are older than 60 years is rising, and falls are the most likely mechanisms of injury in this population. Nontraumatic SCI may result from degenerative spine disease, ischemia, demyelination, inflammation, and extrinsic neoplastic, hemorrhagic or pyogenic masses.
Pathophysiology
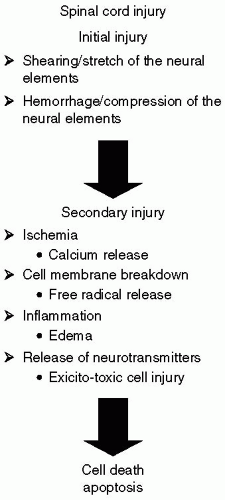
Most experimental studies of SCI have been performed in animal models subjected to spinal cord trauma because this is the most common mechanism of injury in the human population. In most cases, traumatic injury to the spinal cord is limited to stretching or shearing of the neural elements and/or compression manifested by damage to spinal intramedullary blood vessels and hemorrhage into the central gray matter of the cord.2 The critical contributions of secondary mechanisms of injury to the ultimate outcome following acute SCI have been recognized, and therapy is targeted to limit secondary injury. At the time of injury, the initial disruption of spinal cord blood vessels causes a loss of autoregulation and altered autonomic tone. Subsequent hypotension and probable neuronal hypoxia contribute to the release of calcium within the neurons, which causes an uncoupling of oxidative phosphorylation, vasospasm, and activation of membrane phospholipases. These chemicals, in turn, produce a breakdown of the cell membrane and the release of free radicals. Inflammatory processes are also important acutely and over the next several days, as demyelination has been linked to the attraction of neutrophils and macrophages to the traumatized area. Excitatory amino acids (EAAs) such as glutamate are released and bind to N-methyl-D-aspartate receptors, causing receptor-gated channels to open and a further increase in calcium flux. Nitric oxide synthetase is activated. Delayed neuronal cell death, also referred to as apoptosis, may appear remote from the immediate time of injury, although this process is likely to have been initiated through RNA and protein synthesis within minutes of injury (see Fig. 28.1).
FIGURE 28.1 Schematic of spinal cord injury.
In 1990, results from the second National Acute Spinal Cord Injury Study (NASCIS-2) demonstrated that patients achieve improvement in motor function, as well as pin and touch sensation at 6 weeks, 6 months, and a year following treatment with methylprednisolone.3 Steroids have several theoretical beneficial effects, including suppression of vasogenic edema by restoration of the blood: Central nervous system (CNS) barrier, enhancement of spinal cord blood flow, stabilization of lysosomal membranes, inhibition of pituitary endorphin release, alteration of electrolyte concentrations in injured tissue, and attenuation of the inflammatory response. Methylprednisolone is administered as an initial bolus of 30 mg per kg intravenously, followed by an infusion of 5.4 mg per kg for 23 hours. It is crucial that the methylprednisolone be initiated within 8 hours of injury. The NASCIS-3 further refined the time period of treatment so that if a patient receives methylprednisolone treatment within 3 hours of injury, they should be maintained on the treatment protocol for 24 hours.4 Patients initiating steroid therapy 3 to 8 hours after injury should have the maintenance dose extended for 48 hours.5
In recent years, the administration of high dose methylprednisolone for acute SCI has become controversial. Concerns have been voiced over the side effects of the drug, including an increased incidence of pneumonia, pressure sores, wound infection, delayed healing, gastrointestinal bleeding, deep venous thrombosis, acute adrenal insufficiency, and the small beneficial neurologic effects that have been reported utilizing posthoc data analysis in the clinical trials.6 Indeed, the Guidelines Committee of the American Association of Neurological Surgeons (AANS) and the Congress of Neurological Surgeons (CoNS) Joint Section on Disorders of the Spine and Peripheral Nerves concluded that the use of methylprednisolone in the treatment of acute human SCI is recommended as an option that should be undertaken with the knowledge that the evidence suggesting harmful side effects is more consistent than the suggestions of clinical benefit.7 Initiating methylprednisolone in the event of an acute SCI should be a multidisciplinary decision incorporating a high index of suspicion for side effects, careful glucose control, and the appropriate utilization of critical care.8
Multiple experimental models of SCI demonstrate that autoregulation and carbon dioxide responsiveness are lost acutely on injury. Clearly, maintenance of spinal cord perfusion and normocarbia should be priorities in the acute management of the patient with SCI. Additionally, hyperglycemia has been associated with poor neurologic outcome in experimental models following spinal cord ischemia.
What Are the Important Considerations for Acute Care of the Spinal Injury Patient?
▪ CRITICAL CARE
“Spinal shock” is characterized by flaccid paralysis of extremities below the level of the lesion, and absent tendon and patellar reflexes. The hemodynamic consequences of “spinal shock” have been more recently characterized as “neurogenic shock.”9 Systemic vascular resistance is decreased and venous capacitance is increased. If the spinal cord lesion is above T5, interruption of sympathetic outflow to the heart (T1-T5) causes unopposed parasympathetic tone. Very often, patients manifest persistent bradycardia for several weeks following a severe cervical cord injury. Transient external stimuli such as tracheal suctioning or passive movement in patients may further exacerbate bradycardia, which is responsive to therapy with atropine.
In the patient with a cervical spine injury, the respiratory system becomes a focus of intensive care. The diaphragm, the principal muscle responsible for inspiration, accounts for more than 60% of the air exchange during quiet breathing. Innervation is through elements of the cervical spinal cord from C3 to C5. Therefore, if no other injuries are involved, patients with an intact C5 innervation may not require ventilatory support acutely, but have the potential for deterioration at any time in the early phases of injury. Loss of expiratory function is to be expected in those patients who have lost thoracic input from the spinal cord, and gradual deterioration often occurs up to 5 days after injury in the absence of aspiration or pulmonary edema. The development of a left-sided pneumonia is also common, as it is difficult to clear secretions.10 Elective intubation to temporarily support ventilatory function is indicated, as many acutely quadriplegic patients will increase vital capacity over a 5-week period to at least double that measured on admission. This improvement often correlates with the onset of the spastic phase of SCI when chest muscles become contracted and better able to support ventilatory mechanics.
With neurogenic shock, peripheral vascular resistance is decreased, and mean arterial blood pressure may require support. Certain centers have been extremely aggressive in support of cardiac output, such that the therapeutic aim has been a mean arterial pressure of 85 mmHg or above, achieved with combinations of intravenous fluids, colloids, vasopressors, and monitoring utilizing a pulmonary artery catheter. Retrospective reviews have demonstrated results that, when compared to historical controls, are encouraging; however, no randomized prospective trials with hemodynamic controls have been initiated to date. The Guidelines Committee of the AANS and CoNS Joint Section on Disorders of the Spine and Peripheral Nerves state that “Class III evidence from the literature suggests that maintenance of mean arterial pressure at 85 to 90 mmHg after acute SCI for 7 days is safe and may improve spinal cord perfusion, and ultimately, neurologic outcome.”11 Fluid titration utilizing changes in cardiac output and filling pressures is recommended because of concern over the disruption of the pulmonary-capillary endothelium and noncardiac edema, which has been reported even in relatively young patients following cervical SCI. Efforts to increase cardiac output and systemic oxygen delivery are based in theory on experimental data which show that shortly after spinal cord trauma, there is a significant diminution of spinal cord blood flow, and vasospasm in the central gray matter, provoking further ischemic insults. If a vasopressor is necessary, an agent with both α-adrenergic and β-adrenergic action, such as dopamine or epinephrine, should be utilized to counter the loss of sympathetic tone and provide chronotropic support to the heart.
The state of neurogenic shock generally persists from 1 to 3 weeks after injury and resolves with recovery of spinal reflexes. Recovery from spinal shock indicates that nonsynaptic neurotransmission is occurring and, in this phase, some patients may be hypersensitive when neuroactive substances such as vasopressors are administered. Receptors and synapses on the surface of partially denervated spinal cord cells may be upregulated through a denervation supersensitivity mechanism.12
▪ ANESTHETIC MANAGEMENT
Following a traumatic SCI, the exact timing of surgery to stabilize the spinal column is a matter of debate within neurosurgical and orthopedic circles. However, realignment of the spinal elements to prevent additional spinal instability allows the initiation of rehabilitation in patients with neurologically completed injuries. In patients with incomplete injuries, any compression of the spinal cord noted on magnetic resonance imaging (MRI) generally impels the surgical team toward early operative intervention, especially if neurologic deficits are progressive. Often, these procedures are planned while the patient is still within the neurogenic shock phase of injury.13
Many factors related to surgery and anesthesia such as positioning, positive-pressure ventilation, relative hypovolemia, and myocardial depression or vasodilatation caused by anesthetic agents have the potential to exacerbate the neurogenic shock syndrome and cause deterioration of spinal cord perfusion. Additionally, hypothermia may aggravate circulatory instability. In those patients who manifest circulatory instability, intraoperative monitoring should include an intra-arterial catheter and a central venous, pulmonary artery catheter or transesophageal echocardiograph to provide ongoing assessments to maximize systemic and spinal cord perfusion.
Electrophysiologic monitoring, such as somatosensory evoked potential (SSEP) monitoring, or transcranial motor evoked potentials (tMEP) may be requested intraoperatively. Injury to the cord may disrupt the SSEP signals and cause signal derangements in the case of a partial SCI, making interpretation difficult. Before surgery, obtaining an adequate baseline tracing may be impossible. If SSEP monitoring is planned, a total intravenous anesthetic technique utilizing continuous infusions of narcotics and propofol improves the ability to obtain reliable SSEP signals.
Goals for optimal anesthetic management of the patient should include minimal spine manipulation, maintenance of adequate spinal cord perfusion and normocarbia, facilitation of intraoperative monitoring, and a goal of neurologic assessment of the patient as rapidly as possible at the conclusion of the operative procedure. Assuming that the patient is reasonably cooperative, a controlled, awake fiberoptic technique to secure the airway in the patient with a cervical cord injury would be most often utilized, while succinylcholine is avoided following the first 24 hours after injury due to the proliferation of extrajunctional myoneural receptors and associated hyperkalemia following succinylcholine depolarization of these receptors. If clinical signs indicate that extubation is not desirable immediately following surgery because of instability in the cardiovascular or respiratory status of the patient, it is extremely useful for the patient to be managed such that repeated neurologic examinations can be performed. Recurrent compression may occur owing to vertebral malalignment, hematoma, swelling, or delayed abscess formation. Rapid identification of such compression and operative interventions are necessary.
What Do You Need to Know About Assessing the Cervical Spine?
▪ PATHOPHYSIOLOGY AND DIAGNOSIS
In a patient with trauma, failure to identify preoperative cervical instability may result in devastating neurologic injury. Complete spinal cord transection at a high cervical level (C1) results in pentaplegia: Paralysis of the lower cranial nerves, the diaphragm, and loss of sensation and motor function of all four extremities. Quadriplegia refers to injuries at C3-C5, which results in the loss of sensation and motor function of all four extremities, as well as impairment of the diaphragm, while the cranial nerves and sensation to the face and neck and accessory muscles of the neck are spared. Tetraplegia refers to injuries involving C5 and C6, in which diaphragmatic function is retained as well as some movement of the upper extremity, but there is a total loss of function of the lower extremities. Paraplegia refers to injuries below T1, resulting in loss of function of the lower extremities.14
Anterior spinal artery insufficiency; odontoid fracture; retropulsed intervertebral disk
Ipsilateral pain and motor loss, contralateral pain and temperature loss, intact position and vibratory sense
Posterior cord
Tabes dorsalis; posterior spinal cord tumor
Loss of position and vibratory sense, preserved motor function
Central cord
Hyperextension injuries, particularly in the elderly, with anterior cord compression by osteophytes with concurrent posterior cord compression by a buckled ligamentum flavum; syringomyelia
Upper extremity weakness greater than lower extremity, more distal than proximal weakness, pain and temperature sensation may be impaired
Brown-Sequard
Stabbing injuries
Ipsilateral paralysis, vibratory, and proprioception loss, contralateral pain and temperature loss
Incomplete SCI syndromes are listed in Table 28.1. Of these, the central cord syndrome is the most common. These patients frequently require surgery, either for spinal stability or an associated injury, presenting the anesthesiologist with the quandary of managing a patient with a potential cervical spine injury. Because of the potential for catastrophic neurologic injury, nearly every blunt trauma victim is routinely subjected to a plain film radiographic cervical spine series. A complete series must minimally include a lateral cross-table cervical spine, an anterior-posterior view, and an open-mouth odontoid view. The occipitocervical junction and all seven cervical vertebrae, including the C7-T1 junction, must be viewed.
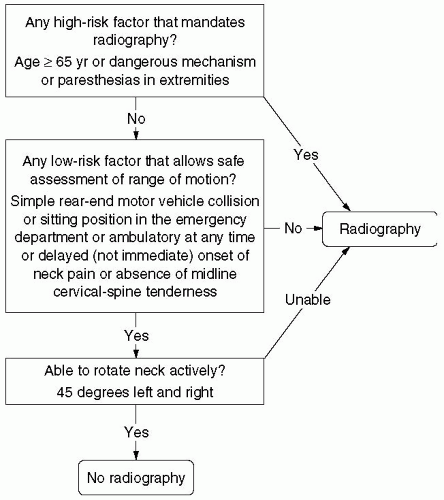
To better delineate those emergency department patients who may be at low risk for cervical spine injury, Hoffman et al. embarked upon the National Emergency X-Radiography Utilization Study (NEXUS) in an attempt to better define those patients requiring radiographic cervical spine evaluation.15 More than 34,000 patients were enrolled at 21 medical centers across the United States.16 The NEXUS low-risk criteria (see Table 28.2) were found to be 99.6% sensitive and 12.9% specific for cervical spine injury. In addition, Stiell et al. formulated the Canadian Cervical Spine Rule (see Fig. 28.2) which encompasses criteria similar to the NEXUS low risk criteria and additionally requires the patient to rotate his head.17 This large, multicenter study of 8,283 patients yielded a sensitivity of 99.4% and specificity of 45.1%. Although a contentious debate as to the superiority of one criterion versus the other continues, both studies suggest that many patients are needlessly radiographed, and that many cervical spines may be “cleared” in the emergency department based on clinical factors.
TABLE 28.2 National Emergency X-Radiography Utilization Study (NEXUS) Low-Risk Criteria
1.
No posterior cervical tenderness with palpation of the midline of the neck from the nuchal ridge to the first thoracic vertebra
2.
No evidence of intoxication
3.
Normal alertness
4.
No focal neurologic deficits
5.
No painful injuries that may distract the patient from cervical pain
FIGURE 28.2 Canadian Cervical Spine Rule. (Reproduced with permission from Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. N Engl J Med. 2003;349:2510-2518. [Figure 1, page 2512].)
TABLE 28.3 Magnetic Resonance Imaging (MRI) Findings in Patients with Severe Ligamentous Injury without Radiographic Abnormalities
Number of Patients with Finding (%) (N = 27)
MRI Finding
25 (93%)
Spinal cord edema or contusion
13 (48%)
Central or paramedian disc herniation
11 (41%)
Spinal stenosis
Data from Hendey GW, Wolfson AB, Mower WR, et al. Spinal cord injury without radiographic abnormality: Results of the National Emergency X-Radiography Utilization Study in blunt cervical trauma. J Trauma. 2002;53:1. (Table 2, page 2)
Unfortunately, radiographic examination of the spine may not detect an uncommon SCI. Hendey et al. evaluated the data provided by the NEXUS study to better determine the incidence of SCIWORA.18 SCIWORA is defined as SCI demonstrated by MRI when complete and adequate cervical spine plain radiographs revealed no injury. A total of 34,069 patients were entered into the NEXUS database; 818 (2.4%) had cervical spine injury. Twenty-seven (0.08%) were patients with SCIWORA with a variety of MRI findings (see Table 28.3). Of note, all 27 patients were found to have at least one documented clinical finding which did not meet the low-risk NEXUS criteria, and all were evaluated with plain radiograph films upon initial presentation.
The NEXUS study revealed a typical distribution of cervical fractures (C2 23.9%, C6 20.25%, C7 19.08%, C5 14.98%) and subluxations (C5-6 25.11%, C6-7 23.77%, C4-5 16.96%) (15). Of most importance is the recognition of those fractures that result in an unstable neck (see Table 28.4), as those patients are at greatest risk of suffering permanent neurologic injury. In summary, trauma patients, particularly those who do not meet the NEXUS or Canadian low-risk criteria, should be treated as if they have an unstable spine. Figures 28.3 and 28.4 are the radiographs of a trauma patient who sustained a C6-7 subluxation, resulting in quadriplegia. Although the plain radiograph clearly demonstrates the C6-7 subluxation, the computed tomography (CT) reconstruction presents fine detail of the bony architecture.
Only gold members can continue reading. Log In or Register to continue