CHAPTER 25

OPHTHALMIC INJURY
Hippocrates was the first person to record the association between facial trauma and blindness.1 Trauma is responsible for bilateral blindness in more than one million people worldwide; unilateral blinding injuries have an estimated incidence of 500,000 cases each year.2 It is estimated that ocular trauma represents 3% of all emergency department visits in the United States.3 In the United States alone, there are approximately 900,000 cases of occupation-related eye injury each year.4 The majority of patients are male (75%–83%) and young (median age of 27–31-years old)5–7 The most common cause of orbital fractures is motor vehicle accidents and assaults. Sports-related injury, especially basketball and baseball, is also a common cause of ocular trauma.8 While many eye injuries are minor in nature, some require urgent evaluation and management and even immediate surgical intervention to preserve sight (Table 25.1).
TABLE 25.1
EMERGENT AND URGENT OPHTHALMOLOGIC INJURIES
HISTORY
A thorough history should be obtained, including the timing and specific events surrounding the injury. A history of grinding or hammering raises the risk for the presence of a foreign body. Important questions regarding ocular history include past visual acuity, need for corrective glasses or contact lenses, and history of glaucoma or cataracts. Specifically inquire about visual symptoms, including change in vision, floaters, flashing lights, pain, discharge, or diplopia.3 Previous ophthalmic surgery (i.e., radial keratotomy and lens implant) may make the eye more susceptible to injury. A past medical history of hematologic disorders (i.e., sickle-cell disease or trait), coagulopathy or use of anticoagulation medications (i.e., warfarin and enoxaparin) increases the risk of bleeding complications, especially in hyphema and retrobulbar hemorrhage. Tetanus immunization status and medication allergies should be elicited.
PHYSICAL EXAMINATION
External Exam and Motility Exam
A general observation should be made for overt abnormalities or defects of the periorbital region and lids. Any evidence of enophthalmos (one eye appearing further back than the other) or proptosis (one eye more anterior than the other) should be noted, as this may indicate damage to the bony orbits. Eyelid position and function, along with any evidence of damage such as lacerations, contusions, or edema should be noted. Pay special attention to any injury that may involve the canalicular region (medially). An observation of the entire ocular surface can be performed by holding the lids open while asking the patient to look up, down, left, and right. The bony structures should be palpated to help identify fractures. Examine for any sign of hemorrhage or foreign body on the surface of the globe. Do not place pressure on the globe if a perforating injury is suspected (see Fig. 25.1).
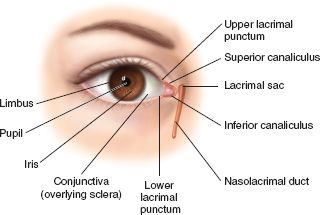
FIGURE 25.1. Ocular anatomy as seen when examining a patient.
Assess extraocular movements by having the patient look in all eight cardinal positions, noting eye alignment and smoothness of pursuit, while asking the patient to report any diplopia or pain. Abnormalities may be indicative of muscle entrapment or orbital hemorrhage, which may require urgent intervention.
Visual Acuity
The traditional way to test visual acuity is to have the patient read the Snellen chart at 20 feet. Each eye should be tested individually and then together. If eye pain is present, placing a drop or two of topical ophthalmic anesthetic can greatly facilitate obtaining an accurate visual acuity. See Table 25.2 for the list of medications. Each eye is then assigned a two-digit score (i.e., 20/50).9 The first number is the distance between the patient and the chart; the second number refers to the smallest line the patient is able to read. If the patient wears corrective lenses, they should be allowed to use them (but document it). For patients who do not have their corrective lenses or their vision is altered, visual acuity should be tested using a pinhole. A pinhole corrects for most refractive errors by ensuring that only light striking the lens perpendicularly reaches the retina.10 If the visual acuity corrects with a pinhole, the problem is likely due to refractive error. If it does not correct, the problem is usually more serious.10
TABLE 25.2
COMMONLY USED MEDICATION IN OPHTHALMOLOGY
Adapted from Ehlers JP, Shah CP, Fenton GL, et al. The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease. 5th ed. Philadelphia, PA: Lippincot Williams & Wilkins; 2008 with permission
For patients who cannot read English, a tumbling E chart may be used, in which the patient identifies the orientation of the letter E (i.e., facing right, facing up).9 For patients confined to the supine position, a near-vision card can be used, held 14 inches from the patient’s face.9 For patients who cannot read the Snellen chart or near-vision card, the patient should be asked to count the examiner’s fingers at a distance of 2 feet. If the patient is unable to count fingers, assess the patient’s ability to detect hand motion from a distance of 1–2 feet. Finally, if unable to detect hand motion, test for light perception. Turn off all lights in the room, completely cover the eye, and test for light perception.9,11 If the patient is unable to detect light, then that eye is considered completely blind.
Pupils
First, perform a general observation of the pupils in ambient room light, noting the shape and size of each pupil while having the patient focus on a distant target. With room lights dim, re-examine the pupils using as little light as possible, noting: shape, size, symmetry, and direct and consensual reaction to light. A relative afferent pupillary defect (RAPD) can be assessed with a rapid swinging light technique while observing the pupils. If the lids are swollen, it may be necessary to have an assistant gently hold the lids open to assist in the examination. A RAPD indicates damage to the anterior visual pathways (optic nerve or retina).
Slit Lamp Examination
The slit lamp is a three-part machine, consisting of a table-mounted binocular microscope with an attached special adjustable light source and a patient headrest.12 Magnification can be adjusted from 6× to 16×. For the examination, the patient is seated, and the chin is placed on a padded rest with the forehead pressed firmly against the forehead bar. The chin rest should be adjusted, so that the patient’s eyes rest at the level of the marker on the vertical poles of the slit lamp.10 The height of the slit lamp is adjusted, so that the light beam is centered on the patient’s eyes. The light source has several adjustments, which allow the beam to be varied from a narrow slit to a wide beam, from short to long, and from dim to bright.12 Most slit lamps allow for changing the filter on the beam, from neutral to cobalt blue (for evaluation of flourescein staining) and red free.10
The examiner should adjust the diopter rings on the ocular piece to account for their individual refractive error and accomodation.10 It is the examiner’s choice to wear their corrective lenses. The patient should be asked to focus on a fixed object (i.e., examiner’s ear). The light beam should be at 45 degree from the patient–clinician axis, using a low-voltage, wide beam. Using the lowest magnification level, the joystick is used to move the device on the chassis until focused.10 Once the eye is in focus, the examiner should conduct a systematic examination of the individual structures. Typically, start with the most external structures (i.e., eyelids and eyelashes) and work deeper, culminating in examination of the anterior chamber (looking for blood, cells, flare, etc.). Magnification can be modified as needed.
Flourescein Staining
Flourescein staining should be performed in all patients with ocular trauma. The only absolute contraindication is flourescein allergy.10 To do this, the eye should be anesthetized first, and then a few drops of sterile saline placed in the eye to moisten it. The fluorescein strip is then placed on the conjunctiva of the eye, and the patient is asked to blink several times to distribute the dye in a thin film over the entire eye.10 The lights should be turned low/off, and the eye examined with a cobalt blue light (i.e., hand-held, Wood’s lamp, or using the slit-lamp). Injured epithelium (i.e., abrasion) will appear yellow green. The location of the abrasion should be documented, normally using the clock method (i.e., 3-mm linear abrasion at 7 O’clock). A variation of this, called the Seidel test, can be performed when a full thickness corneal disruption or open-globe injury is suspected. For this test, a large amount of flourescein dye is placed on the eye, causing the entire eye to appear orange. Then, with the lights out, the globe is examined for a dark stream interrupting the flourescein, indicating leakage of aqueous humor and a globe rupture.10
For this to be best observed, the patient needs to be in an upright (i.e., seated) position (see Fig. 25.2).
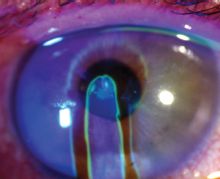
FIGURE 25.2. A positive Seidel test in a patient with a full-thickness corneal laceration.Note the downward streaming of aqueous humor. (Reprinted with permission from Ehlers JP, Shah CP, Fenton GL, et al. The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease. 5th ed. Philadelphia, PA: Lippincot Williams & Wilkins; 2008.)
.
Tonometry
Tonometry is the measurement of intraocular pressure (IOP). Normal IOP is between 10 and 20 mm Hg. The most common condition for low IOP in the setting of trauma is perforating globe injury with loss of aqueous fluid. However, if a perforated globe is suspected, tonometry should not be performed because of the possibility of causing further extrusion of intraocular contents. High IOP (i.e., >30 mm Hg) in the setting of orbital trauma is commonly observed in hyphema, anterior lens dislocation, or retrobulbar hemorrhage. A baseline IOP should be measured in all patients with blunt orbital trauma, except in the case of suspected globe rupture or perforating globe injury.
The most common tools used for performing tonometry are a portable hand-held device (i.e., Tonopen) or the older Schiotz tonometer. The hand-held device is digital, has good interexaminer reliability, and can be used with the patient in any position. The Schiotz tonometer requires the patient to be in the supine position. Both methods determine IOP by measuring the amount of corneal indentation produced by a certain amount of force. Both methods also require the eye to be anesthetized and the patient cooperative. It is best to repeat measurements several times in order to obtain a reliable reading.
Direct Fundoscopic Exam
The direct ophthalmoscope allows a fundoscopic examination with approximately 15× magnification. Since the examiner performs the exam using only one eye, the view is not stereoscopic. Although a view may be obtained through a small pupil, pharmacologic dilation will enhance the view. The instrument field of view is limited to about the equator, making it inappropriate for a full peripheral funduscopic examination. The examination is performed with the eye that corresponds to the eye being examined. The focusing lens is rotated to the examiner’s refractive error or starting at zero and rotating until fundus details come into view. Focus first on a blood vessel and then trace it back to the optic nerve, noting color, clarity of disc margins, and cup to disc ratio. Note any abnormalities such as hemorrhages, exudates, or pigment changes.
IMAGING IN OCULAR TRAUMA
The decision for imaging patients with suspected ocular trauma should be guided by the mechanism of injury, clinical presentation, and physical examination. Frequently, the history and physical exam may be limited due to the severity of the injury, associated injuries, and/or facial swelling. The decision on which imaging study to order will depend on resource availability, local practice and custom, and the type of injury suspected. That said, computed tomography (CT) is considered the imaging study of choice in the evaluation of orbital trauma.3,13
Radiographs
Radiographs are being used less frequently. While the sensitivity of radiographs for detecting fractures is 64%–78%, it is very poor in identifying orbital content injuries.14 Radiographic findings suggesting fracture include an air-fluid level in, or opacification of, the maxillary sinus (from bleeding secondary to an orbital floor fracture) and the tear drop sign (orbital contents herniating into the maxillary sinus due to an orbital floor fracture). If there is a low suspicion for metallic orbital or intraocular foreign body (IOFB), a Water’s view x-ray may be a cost-effective test. However, if the pretest probability is high or the suspected foreign body is nonmetallic, radiographs play no role.
Ultrasound
Ultrasound has been used in the evaluation of the multitrauma patient for some time. It is now being increasingly used for the evaluation of ocular trauma. Ultrasound can be performed directly at the bedside and is fast, safe, noninvasive, and avoids the use of ionizing radiation. Ocular sonography has been shown to be used successfully by nonradiology and nonopthalmology physicians.15
A high-resolution linear array 10 MHz transducer (or vascular probe) should be used. The output and gain should be minimized to prevent image distortion by eyelid echos and to maximize image quality.16 The eye should be closed, ultrasound gel applied, and scanned in the sagittal and transverse plains. Injuries identified by ultrasound include retrobulbar hemorrhage (hypoechoic lucency deep to the retina), lens dislocation (abnormal position of the lens within the globe), vitreous hemorrhage (echogenic material within the vitreous body), IOFB (echogenic foreign body visualized within the globe), and globe rupture (difference in globe size between the eyes).16 There is some controversy regarding the role of ultrasound in evaluating suspected globe rupture. It appears that the majority of experts feel that ultrasound is contraindicated in suspected globe rupture due to potentially causing extrusion of intraocular contents.3,13,17 Those in favor of ultrasound recommend placing a large amount of ultrasound gel over the closed eye, so that the probe never actually exerts pressure on the eye.16 Regardless, if there is an obvious anterior perforation, ultrasound should not be performed.
Computed Tomography
CT is considered the standard imaging modality in the evaluation of mid-face fractures and orbital trauma.3 Typically, thin slices (i.e., 1 mm) with multiplanar reformation has the best results.11,13 The sensitivity of CT for orbital fractures is 79%–96%, with a lower sensitivity for infraorbital rim injury.18 CT identifies open-globe injuries with a sensitivity of approximately 71%.19 Findings suggesting open-globe injury on CT include a change in globe contour, an obvious loss of volume, a deep anterior chamber, scleral discontinuity, and intraocular air.13 The sensitivity of CT for detecting clinically occult open-globe injuries is slightly less, varying from 56% to 68%.13 When an IOFB is suspected, CT is usually the study of choice. It can demonstrate metal fragments <1 mm in size.13 It is also the best study for detecting glass, compared to US and magnetic reasonance imaging (MRI). Glass fragments of at least 1.5 mm diameter are detected 96% of the time and 48% for glass fragments 0.5 mm in size.20 Other injuries detected by CT include corneal laceration (decreased volume of the anterior chamber with decreased anterior–posterior dimension compared to normal globe) and lens displacement/dislocation (abnormal lens position).
Magnetic Resonance Imaging
Given the limitations of MRI, including availability, contraindications (i.e., presence of metal), and length of imaging time, MRI is not recommended as the initial imaging modality in orbital trauma. Currently, it is most useful in identifying intraorbital wood or organic material when CT results are either negative or equivocal.3,13
CORNEAL ABRASION
Patients will present with pain, foreign body sensation, photophobia, and tearing. Frequently, there is a history of trauma, but sometimes the patient does not recall any specific event. Placing a drop of topical ophthalmic anesthetic in the affected eye will allow for a more efficient history and physical examination. The immediate pain relief following placement is characteristic of corneal abrasion. Physical exam reveals conjunctival injection, tearing, and decreased visual acuity if the abrasion is large or lies within the visual axis. Fluorescein staining and examination under the slit lamp or use of a cobalt-blue light will reveal fluorescein uptake if there is an epithelial defect. The size and location should be documented. The anterior chamber should be examined for cells, flare, and blood. Always examine the eye carefully for the presence of foreign bodies, including everting the upper and lower eyelids. Treatment includes the use of cycloplegics to decrease ciliary spasm (and pain), topical ophthalmic antibiotic ointment, and analgesia (see Table 25.2). Pain may be managed with topical or po nonsteroidal anti-inflammatory medications or a short course of po narcotics. Patching the eye has been shown to offer no benefit for simple corneal abrasions and should not be used.21 Never give or prescribe the patient topical anesthetic agents, as their repetitive use will cause ocular toxicity. Because contact lens wearers are at risk for pseudomonas infection, topical ophthalmic tobramycin ointment should be used in these patients. Patients with corneal abrasions should be instructed not to wear their contact lenses until the abrasion is completely healed. All patients should be re-examined within 24 hours.
CORNEAL FOREIGN BODY
For a corneal foreign body, the presentation, evaluation, and management (after foreign body removal) are similar to corneal abrasion. Patients complain of foreign body sensation, pain, photophobia, and tearing. Vision may be affected if the foreign body is large or within the visual axis. Similar to corneal abrasion, placement of a drop or two of topical ophthalmic anesthetic will facilitate the history and physical examination. Foreign bodies are frequently visible without magnification; however, if available, a slit lamp exam should be performed. Examine the eye closely for any other injuries. Make sure to evert the lids to inspect for foreign bodies. The majority of corneal foreign bodies are superficial and can be safely removed in the ED. Full thickness corneal foreign bodies require ophthalmology consultation. Foreign bodies are best removed under slit lamp magnification. A 27-gauge needle on the end of a tuberculin syringe or a moistened Q-tip will usually work well in removing the foreign body. Both eyes should be anesthetized to decrease reflex blinking. During removal, the patient’s forehead should be pressed firmly against the slit lamp, the lids held open with the physician’s nondominant hand, and the dominant hand (holding needle or Q-tip) should rest against the bar of the slit lamp machine to stabilize it. Using the bevel of the needle, the motion should be a gentle scraping motion, away from the patient, and parallel to the eye.
Corneal rust rings are a complication of metallic foreign bodies. If the rust ring is superficial, not over the visual axis, and an ophthalmic burr is available, removal can be attempted. All patients should be referred for ophthalmologic follow-up within 24 hours. Rust ring removal is actually easier the following day due to corneal edema and anterior displacement of the foreign material.
Postremoval treatment includes cycloplegics, ophthalmic antibiotic ointment, and analgesia, as in corneal abrasion. If the foreign body is organic (i.e., plant or vegetable material), a topical ophthalmic fluoroquinolone should be used (see Table 25.2).
CHEMICAL INJURIES
The spectrum of injuries to the eye caused by exposure to chemicals varies from mild to very severe with potential blindness. The most common agents include alkalis (i.e., lye, plaster, cement, airbag powder or agents containing ammonia, sodium hydroxide, or lime), acids (sulfuric, sulphurous, hydrofluoric, acetic, chromic, and hydrochloric), solvents and detergents, and cyanoacrylate (superglue).22 We will discuss cyanoacrylate injury separately.
The severity of the chemical injury is related to the properties of the chemical, the duration and extent of exposure, and other concomitant injuries to the eye, including thermal exposure. In general, alkali injury is more severe than acid. Alkali injuries are especially damaging due to rapid, deep tissue penetration; complete corneal opacification and melting can occur. Acid burns cause denaturation of tissue proteins, which then acts as a barrier to further penetration, thus limiting their damage.23 Solvents and detergents typically result in chemical conjunctivitis.
Conjunctival and eyelid hyperemia, chemosis (conjunctival swelling/edema), and corneal punctuate epithelial defects are frequently observed in mild injuries. Conjunctival hyperemia or blanching (due to limbal ischemia), corneal haze, or opacification can be observed in severe cases.
Treatment should be instituted immediately and without delay, even before obtaining a visual acuity or pH testing. The only exception is in the case of a suspected open-globe injury, in which further damage may be caused by the force of irrigation.
A topical anesthetic should be placed into the eye along with an eyelid speculum. The treatment involves copious irrigation of the corneal surface with normal saline or Ringer’s lactate (preferred) for at least 30 minutes. This can be performed by attaching IV tubing to the irrigation solution and directing the flow of fluid into the eye. Tap water irrigation can be used if these solutions are unavailable. The upper and lower lids should be everted and inspected for retained particulate, which should be removed if present and then copiously irrigated. After 30 minutes of irrigation, wait 5–10 minutes and then check the pH by placing litmus paper in the inferior fornix. Irrigation should then continue until a neutral pH of 7.0 is reached. The volume of irrigation fluid and time needed to reach neutral pH varies widely and may involve as much as 8–10 L of irrigation.24
Cyanoacrylate (i.e., Super Glue and Krazy Glue) in the eye is managed differently. The most common injury following cyanoacrylate administration into the eye is a corneal and/or conjunctival abrasion. Cyanoacrylate bonds only with dry surfaces; therefore, fusion of the upper and lower lids occurs predominantly through bonding of the eyelashes.25 Collections of hardened glue particulate will tend to occur in the inferior fornix. Periocular skin irritation and dermatitis can also occur.
Initial management includes attempting to remove any loose glue stuck to the lashes and to gently open the eye. The use of ophthalmic ointment gently rubbed into the lashes may facilitate glue removal, especially if it is allowed to penetrate before attempting to mechanically remove loose glue. Avoid use of alcohol or other solvents. Cutting of the lashes may be necessary to open the eye. The eye should then be irrigated with normal saline or Ringer’s lactate for at least 15 minutes. Topical anesthetic and fluroscein should be used to aid in inspection of the cornea for any abrasions or glue debris, which should be removed. The upper and lower fornicies should be inspected for retained glue particulate. Any associated corneal abrasion or persistant glue on the lashes can be treated with ophthalmic antibiotic ointment. Most reported cases suggest spontaneous separation of the upper and lower lids will occur within 1 week from initial application of cyanoacrylate.25 Associated dermatitis can be treated with periocular skin lubrication, such as ophthalmic ointment. Cycloplegic agents may be used to increase patient comfort in the case of associated ciliary spasm or photophobia. Patients with corneal involvement should have ophthalmic follow up within 24 hours.
CONJUNCTIVAL LACERATIONS
Lacerations of the conjunctiva are usually associated with intraocular foreign bodies or scleral perforation.3 For these reasons, it is important to exclude a ruptured globe. Conjunctival lacerations may appear as a conjunctival defect or presence of fat. Slit lamp examination will usually be necessary to differentiate superficial from deep lacerations. Superficial lacerations <1 cm in length do not usually require repair and will normally heal quickly.3 Lacerations >1 cm should be repaired by ophthalmology, normally using 6–0 to 8–0 absorbable sutures. All patients should be treated with prophylactic antibiotic ointment or drops.3
LID LACERATIONS
The upper and lower eyelid skin is very thin, with minimal dermal tissue. Directly under the skin and dermis is the orbicularis muscle, responsible for eyelid closure. The muscle completely surrounds the lid fissure and is attached medially and laterally by the medial and lateral canthal tendons, which are adherent to the orbital rim. The orbital septum extends from the orbital rim and attaches superiorly to the levator aponeurosis and inferiorly to the lower lid retractors. The orbital septum separates the lid from the underlying orbital fat. The tarsus is the dense connective tissue deep to the orbicularis muscle, which gives the lid rigidity. Conjunctiva lines the lids and lid fissures and is continuous over the surface of the globe (see Fig. 25.1).
Multiple mechanisms of injury may result in laceration of the eyelid. It is critical that the patient presenting with a lid laceration be meticulously examined for the possibility of concurrent injuries such as canalicular lacerations, corneal or sclera lacerations, orbital wall fractures, an intraocular or embedded foreign body or injury to the extraocular muscles. Beginning with the external examination, an attempt should be made to ascertain the depth of the injury. If orbital fat is prolapsed through the wound, the orbital septum has been violated, and the fat will require repositioning. The presence of orbital fat at the wound should alert the practitioner to the possibility of deeper injuries involving the globe. In cases of possible high-velocity fragment injury, one should suspect penetration into the eye or perforation into the globe and obtain CT imaging. A foreign body should only be removed if there is no evidence of deeper extension into the globe or orbit.
Avulsion of the canalicular apparatus, which is medial, can occur with lateral traction injuries to the eyelid; this can commonly be seen in assault and dog-bite injuries. These injuries will require specialized surgical intervention to repair the lacrimal drainage system and prevent chronic tearing and lid malposition.
The presence of ptosis in a patient presenting with a lid laceration may indicate injury to the underlying levator muscle. Such injuries may require subsequent surgical intervention following initial repair in order to restore lid function. Cleansing of lid wounds should be performed using povidone–iodine 5% solution, only after the integrity of the globe has been established.
In extensive lid injuries in which closure of the eye is affected or when surgical repair needs to be delayed, saline-soaked dressings should be applied to the area to promote viability of the tissue.
For repair of lid lacerations, general anesthesia is used in children and in uncooperative adults. Otherwise, local anesthesia is used in adults (2% xylocaine with epineherine 1:100,000). Because direct injection of local anesthetic causes tissue distortion and bleeding, use the minimal amount of anesthetic necessary to obtain adequate pain control. Make sure that there is no injury to the globe before attempting eyelid repair. Place a drop of topical anesthetic into the eye to facilitate patient comfort. The wound should be irrigated thoroughly with normal saline or Ringer’s lactate.
Use toothed forceps or cotton-tipped applicators to gently open the edge of the wound to determine depth of penetration. The lid tissue should be realigned and repaired in layers. Any injury involving the lid margin or canalicular region will require specialized repair by an ophthalmologist or surgeon specialized in lid anatomy and surgical procedures. Lid margin injuries require precise apposition of tissue to prevent lid notching. If the tarsus is involved, use 5–0 absorbable sutures.26 Extreme care must be taken to avoid injury to the underlying globe. A corneal shield can be placed to avoid such injury, although it can make the repair more difficult due to its bulk and distortion of tissue. The orbicularis/deeper tissue can be repaired using 6–0 interrupted vicryl sutures, and the skin closed using 6–0 interrupted silk or nylon sutures. Care should be taken to evert the wound margin to avoid depressed scars. In some cases, where patient follow up may be limited, or in the case of children when it may be desirable to avoid suture removal, the skin may be closed with 6–0 fast absorbing gut or vicryl suture. Topical ophthalmic antibiotic ointment is applied to the wound. Generally, silk or nylon sutures are removed within 5–7 days. Contaminated injuries should be treated with systemic antibiotics: dicloxacillin or cephalexin, 250–500 mg PO QID in adults and 25–50 mg/kg/d divided into four doses for pediatric patients.26 In animal bite injuries, infection and rabies prophylaxis require consideration.
TRAUMATIC HYPHEMA
Hyphema is defined as blood in the anterior chamber. In urban settings, two-thirds of traumatic hyphema are due to blunt ocular trauma and one-third due to traumatic globe rupture.27 The source of bleeding is usually from the iris or ciliary body. The amount of blood present in the anterior chamber determines the grade of the hyphema: grade 0—microhyphema with red blood cells detected only by slit-lamp examination; grade 1—blood occupying less than one-third of the anterior chamber; grade 2—blood filling one-third to one half; grade 3—one half to less than total; and grade 4—chamber filled completely with blood (also known as an eight ball).3 The majority of hyphemas are grade 1 (see Fig. 25.3).

FIGURE 25.3. Grade 1 hyphema in a patient struck in the eye with a ball. (Reprinted with permission from Ehlers JP, Shah CP, Fenton GL, et al. The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008.)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


