
OBSTETRIC AND GYNECOLOGIC EMERGENCIES
ACUTE SURGICAL CARE CONSIDERATIONS IN THE PREGNANT PATIENT
Pregnant patients who require nonobstetrical surgical intervention pose unique challenges due to altered anatomy and physiology, as well as the impact of the surgical pathophysiology and its treatment upon the fetal environment. Disease processes amenable to surgical intervention are altered in their presentation, by both objective changes in maternal physiology and alteration of symptom perception by the gravid patient. Add to this the reluctance of providers to pursue a surgical therapeutic course for fear of complicating the pregnancy, and the delay of definitive treatment may become a major determinant of outcome. Furthermore, hesitancy to utilize certain diagnostic modalities can delay needed surgical intervention. Acute care surgeons should understand physiologic changes in pregnancy and abnormal presentations of common general surgical problems, since 0.5%-1% of pregnant patients will require nonobstetrical surgical intervention during pregnancy.1
To address these concerns, this section will review pertinent maternal physiology and typical diseases that require surgical therapy in pregnancy, provide normal laboratory values in the gravid patient, and give guidance on diagnostic modalities in pregnancy. If a gravid patient presents with signs and symptoms of disease requiring acute surgical intervention, two rules generally apply: treatment that supports or restores normal maternal physiology will help the fetus (to help the fetus, treat the mother first), and consultation with an obstetrician, if readily available, is advisable.
MATERNAL PHYSIOLOGY
Acid/Base
Respiratory changes during pregnancy produce a mild alkalosis via hyperventilation while maintaining normoxia. There is a concomitant, although smaller, increase in urinary excretion of bicarbonate. The result is a mild increase in pH with a lower pCO2 and lower serum bicarbonate. These changes are reflected in the blood gas values typical of pregnancy as seen in the table of normal lab values in pregnancy (Table 44.1).2
TABLE 44.1
NORMAL REFERENCE RANGES IN PREGNANT WOMEN
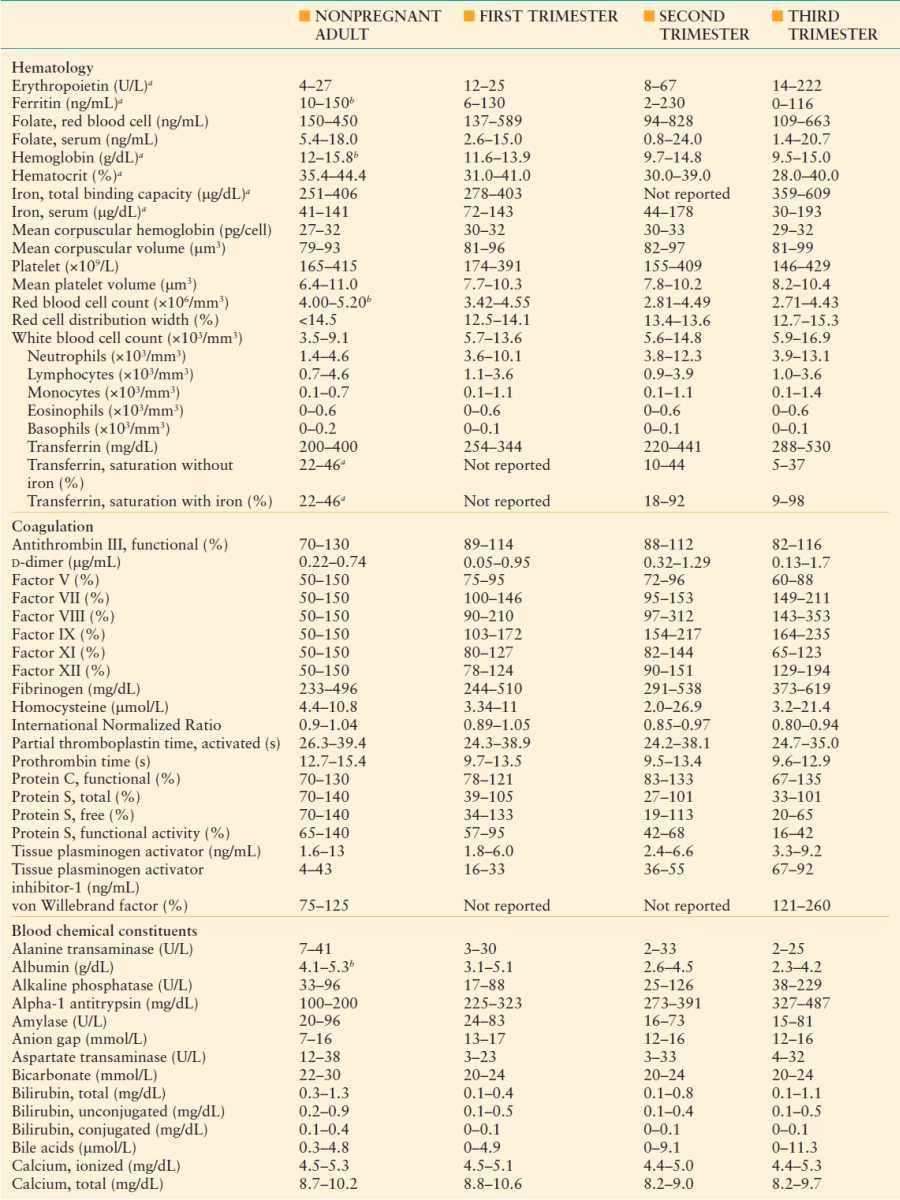
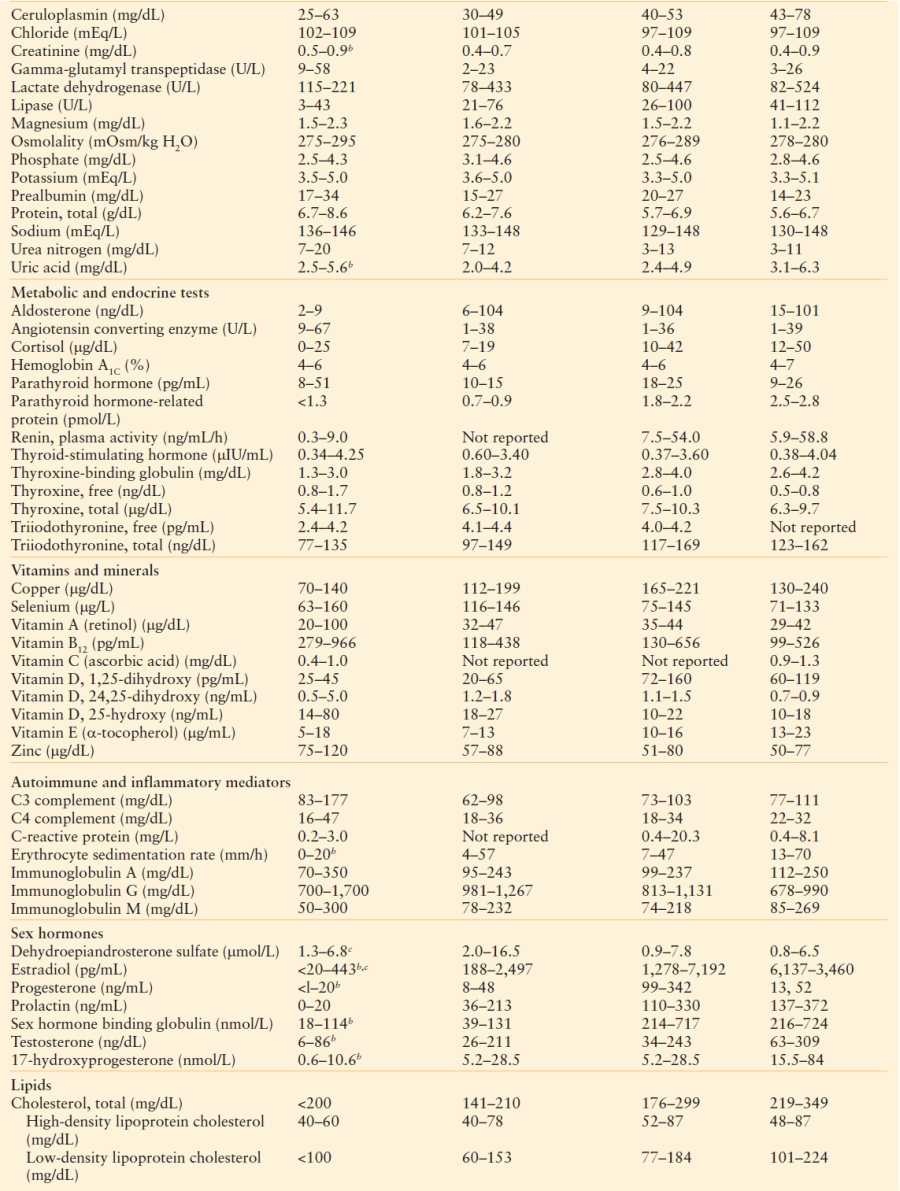
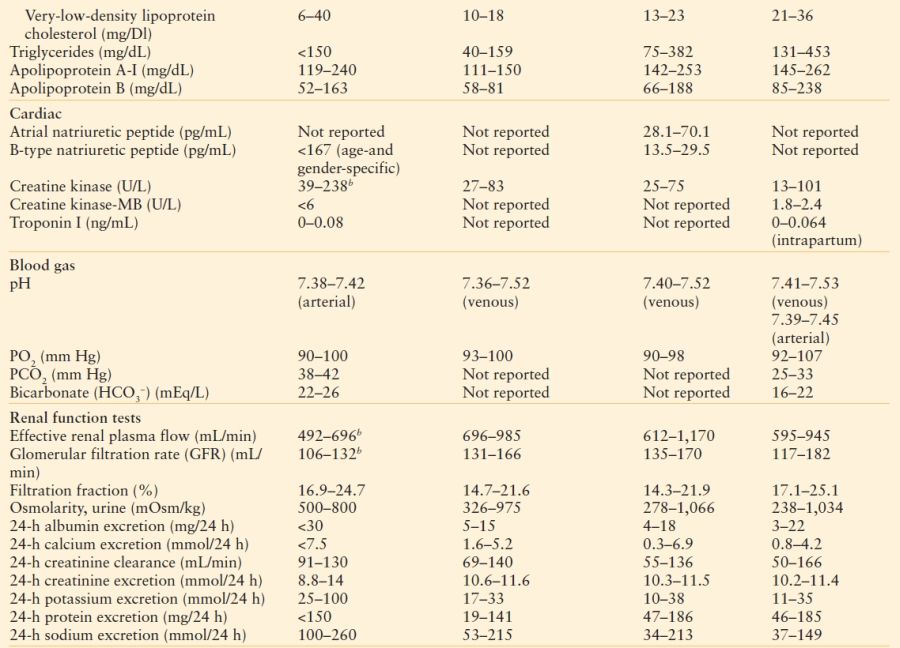
The references used to construct this table are listed in the UpToDate topic:
Normal reference ranges for laboratory values in pregnancy.
aRange from references with and without iron supplementation.
bNormal reference range is specific range for females.
cRange is for premenopausal females and varies by menstrual cycle phase.
Reproduced with permission from:Abbassi-Ghanavati M, Greer LG. Reference table of normal laboratory values in uncomplicated pregnancies. In: Cunningham FG, Leveno KJ, Bloom S, et al., eds. Williams Obstetrics, 23rd ed. New York: McGraw-Hill; 2010.
Cardiovascular
Cardiac output increases in response to an increase in basal metabolic rate along with blood volume expansion that begins at 8 weeks, reaches 15% by 12 weeks, and peaks at 40%-45% increase in blood volume.3 Reduction in systemic vascular resistance and an increase in resting heart rate of 10 beats per minute help achieve a cardiac output of 6–7 L/min in the third trimester, to 8–9 L/min in labor and in the immediate postpartum period. Maternal position can have a profound effect on cardiac output, with an increase of 1.2 L/min, about 20%, from a supine to left lateral decubitus position.4 Uterine blood flow at term is 600 mL/min but decreases by as much as one-third in the supine position.5 This uterine perfusion decline from supine positioning can alter fetal oxygen saturation by 10%6 and create persistent fetal heart rate decelerations, which may result in fetal distress.
Respiratory
An increase in minute ventilation is produced by 21% increase in tidal volume, whereas respiratory rate remains stable. The diaphragm elevates 4 cm and thoracic diameter increases by 2 cm resulting in a chest circumference increase of 6 cm. However, the sum of these changes is a decrease in total lung capacity of about 200 mL. Expiratory reserve volume and residual volume (and their sum, functional residual capacity) decrease due to diaphragmatic elevation and increase in tidal volume. Inspiratory reserve volume and vital capacity are preserved. Peak expiratory flow decreases by 0.5 L/min/wk of gestation across pregnancy, translating to a loss of 10% in a woman of average height.7 The total of these pulmonary changes is a diminished capacity of the gravida for tolerating respiratory insult, or exacerbation of underlying pulmonary disease, such as asthma.
Renal
Changes in renal function in pregnancy result in a temporarily hyperfunctioning organ. Both renal perfusion and glomerular filtration rate (GFR) increase early and rapidly. By 2 weeks postconception, GFR increases 25% over nonpregnant status; by the second trimester (13 weeks after the last menstrual period) GFR is up 50%. Renal perfusion increases to a greater degree, until late third trimester when renal perfusion declines slightly more than GFR. The increased urine production results in urinary frequency. Due to anatomic compression of the ureters and dextrorotation of the uterus, hydronephrosis and hydroureter occur, greater on the right than the left. High levels of progesterone from the placenta act as a smooth muscle relaxant, slowing ureteral peristalsis. The result is a higher risk for lower urinary tract infection, and pyelonephritis. Enhanced urine production results in a lower average serum creatinine of 0.5 mg/dL, with levels above 0.8 mg/dL considered abnormal in pregnancy. Hyperfunction allows greater excretion of bicarbonate, with a resulting decrease of serum bicarbonate by 4–5 mEq/dL, helping to balance the hyperventilation in the pulmonary system, and compensating partially for the respiratory alkalosis of pregnancy. Serum osmolarity is reduced by 10 mOsm/L, serum sodium is reduced by about 5 mEq/L, and amino acids and water-soluble vitamins are lost at a greater rate during urine production.
Metabolism
Pregnancy requires 10%-20% more caloric intake or approximately 300 kcal/d.8 Growth of the fetus and placenta, maternal blood volume expansion, and uterine muscle hypertrophy occur via addition of 1,000 g of protein. Nitrogen balance is positive due to more efficient use of dietary protein. Urinary amino acid metabolites suggest that maternal muscle is not broken down to obtain the amino acids that the placenta concentrates in the fetus. Medication metabolism is altered with many of the CYP enzymes elevated substantially throughout pregnancy, but others are reduced.9 Along with increased maternal plasma volume and weight, drug bioavailability and metabolism may be altered in difficult-to-predict patterns.
ANESTHESIA
General endotracheal anesthesia carries greater risk for the pregnant patient, primarily due to increased risk of aspiration and vascular congestion of the airway. Gastric emptying and pH are not altered in pregnancy, but progesterone relaxes the gastroesophageal sphincter, creating the equivalent of a full stomach. Laryngeal edema, soft tissue increases in the upper chest and neck, and the chest wall diameter increase in pregnancy may complicate airway management via face mask, laryngeal mask, or endotracheal tube. In addition, anesthetic agents, although known not to increase malformation risks for the fetus, are capable of hampering physiologic compensation for supine positioning and aortocaval compression in the second and third trimesters.
FETUS
Gestational age plays a key role in determining the approach to operative treatment in pregnancy. At term (>37 weeks gestation), delivery concomitant with surgical therapy may be an appropriate approach, though cesarean delivery is not uniformly indicated. Preterm birth occurs in about 5% of gravidas undergoing abdominal surgery before 37 weeks. Operative treatment for disease with a prominent infectious or inflammatory component is more likely to result in labor. Due to the increased risk of preterm birth, antenatal steroids (betamethasone 12 mg parenterally, 2 doses 24 hours apart) to accelerate fetal lung maturation should be considered between 24 and 34 weeks gestation, if the surgical condition is not adversely affected. Fetal lung surfactant production stimulated by betamethasone commences within hours and peaks by 48 hours after the first dose. However, operative intervention should not be postponed for that goal unless it is safe to do so. If maternal status allows, transfer to a tertiary care center should be made in case preterm delivery ensues. If transfer is not possible and delivery seems likely, then transport of the neonate needs to be arranged.
SURGICAL AND OBSTETRIC EMERGENCIES
Trauma
Trauma is a leading cause of maternal mortality, with homicide, accidents, and suicide being the most likely sources of trauma. Fetal death can occur, particularly after 12 weeks’ gestation when the uterus becomes an abdominal organ. Severe motor vehicle crashes can result in maternal shock or death, or placental abruption, contributing to fetal loss rate of 8%.10 Low birth weight and delivery within 48 hours are more common for unrestrained gravidas. If possible, a pregnant woman involved in a vehicular crash should be transported to a center with obstetric and intensive neonatal care capabilities. She should be placed in left lateral tilt position if injuries allow, to optimize cardiopulmonary function. The trauma survey should proceed normally, with attention to maintenance of adequate intravascular volume. Routine laboratory studies are obtained as are any imaging studies necessary for evaluating the injuries. If the mother is Rh negative, RhoGAM should be given after obtaining a type and screen and Kleihauer-Betke test to estimate the volume of any fetomaternal hemorrhage from blunt abdominal trauma. If known or thought to be 24 weeks or greater in gestation, assessment of fetal heart rate by ultrasound, or preferably, continuous external Doppler monitoring of the type used in labor and delivery, should be routine. An obstetric provider familiar with interpretation of fetal heart rate tracings (obstetrician, family practitioner, certified nurse-midwife or labor and delivery nurse) should assess fetal stability as early in the care as possible. If between 24 and 34 weeks’ gestation, administration of betamethasone to accelerate fetal lung maturity should be considered, if not contraindicated.
When the pregnant patient presents with trauma, symptoms such as vaginal bleeding and abdominal pain, and signs, such as tachycardia and hypertension, can overlap with several potential pregnancy complications. With blunt trauma, separation of the placenta from deformation of the uterine wall as a result of direct impact or sudden deceleration can result in placental abruption. Blood loss of 1–2 L can be sequestered in the gravid uterus, resulting in severe abdominal pain or labor, and can lead to rapid onset DIC. This places the mother and fetus at grave risk, with need for immediate delivery to prevent fetal death. A large-volume transfusion protocol should be employed early in the management of abruption of this degree. In addition, a drug screen should be obtained. Illicit drug use is a common problem in obstetrical emergencies. Nearly half of trauma in pregnancy is associated with substance abuse. Heroin and methamphetamines are the most commonly abused drugs in pregnancy.
Penetrating abdominal trauma is likely to affect the uterus in the second and especially third trimesters, with the risk for fetal injury or death increasing as gestational age increases. Diagnostic peritoneal lavage can be used in the gravid patient safely, although the location for incision may be altered. Amniocentesis may be helpful to determine whether the uterus has been penetrated or the fetus directly injured. Amniotic fluid, obtained by ultrasound-guided needle aspiration, can also be sent for fetal lung maturity studies in late preterm fetuses (>30 weeks) to aid in decisions regarding delivery. Depending upon the degree of prematurity as estimated by gestational age and neonatal care capabilities of the facility, immediate delivery of a fetus injured by penetrating trauma may be indicated.
Nontraumatic Obstetric Hemorrhage
The uterus grows in weight from 70 g nonpregnant to 1,100 g near term. Enlargement is accomplished by myocyte hypertrophy and addition of fibrous and elastic tissue. Perfusion of the uterus increases to a peak of 450–650 mL/min at term11 through uterine arteries that double their diameter by 20 weeks’ gestation, resulting in flow velocity that is eightfold greater than nonpregnant. Venous dilation to accommodate this increased blood flow is accomplished through decreased elastin and reduced adrenergic innervation in response to various placental hormones. Cessation of blood loss from placental implantation site after delivery is accomplished primarily via contraction of myocytes interlaced with the uterine vasculature. In addition, there are substantial increases in several of the coagulation proteins during pregnancy, and platelet concentration is decreased only slightly at term despite a large increase in circulating volume.
However, there are several conditions that can precipitate hemorrhage before or during labor, or after delivery. Acute obstetric hemorrhage is usually evident as vaginal bleeding, but may be sequestered within the uterus. Rarely, hemorrhage can occur intraabdominally. The mother’s complaints can range from painless vaginal bleeding to uterine contractions or even tetany; she may even present with signs of peritoneal irritation. Disseminated intravascular coagulation may occur with fetal death, massive placental abruption, or amniotic fluid embolism.
Abdominal Pain
Abdominal pain is a common complaint in normal pregnancy and frequently provokes acute visits to the obstetrician. Etiologies for abdominal pain may relate directly to pregnancy; “round ligament” pain, contractions, placental abruption, adnexal mass, ovarian torsion, or degenerating uterine fibroids. Other etiologies such as urinary tract infection, constipation, bowel gas, renal calculi, and gallstones are influenced by an enlarging gravid uterus and increasing levels of placental hormones. Some sources of abdominal pain are common, but unrelated to pregnancy per se, such as appendicitis, abdominal adhesions, bowel obstruction or intussception, and inflammatory bowel disease.
The most common diagnoses associated with abdominal pain that require surgical intervention are adnexal mass, appendicitis, and cholelithiasis/cholecystitis. Depending upon gestational age, these may be handled laparoscopically. Several series on third trimester laparoscopic operations appear to provide similar outcomes with the advantages of minimally invasive surgery. An altered approach to laparoscopic entry to the peritoneal cavity may be necessary depending upon the size of the gravid uterus. The greatest danger for appendicitis in pregnancy is delay in diagnosis, with a 50% negative appendectomy rate acceptable, given the high maternal morbidity and mortality as well as preterm birth risk of undiagnosed, ruptured appendicitis. Cholelithiasis can be treated conservatively with some success, although recurrent or prolonged symptoms may mandate cholecystectomy during pregnancy. The greatest danger is progression to cholecystitis, with a likely increase in preterm birth risk. Risk of untreated ovarian torsion is loss of the affected ovary and ovarian vein thrombus formation.
Surgery Outside the Abdomen
In general, surgery outside the abdomen is less likely to result in preterm birth. There is less opportunity for direct stimulation of the uterus, either by the disease or the surgical procedure. However, involvement of an obstetrician is advisable, and elective surgery should still await delivery of the pregnancy at term.
For orthopedic procedures prompted by trauma, the mechanism of trauma and any concomitant abdominal trauma are factors most likely to determine impact upon pregnancy. If prolonged immobilization is anticipated, thromboprophylaxis may be indicated, possibly for longer than is routine from the orthopedic perspective. Head and neck surgery may be impacted by anatomical alterations involving the airway secondary to vascular congestion as well as soft tissue accumulation in the upper chest and neck. Neurosurgical conditions may impact maternal cardiovascular and pulmonary physiology sufficiently to endanger maternal support of the fetus. At essentially all gestational ages, if management of neurosurgical disease mandates controlled hypotension to preserve maternal life or brain function, it should be used, knowing that the fetus is intolerant of prolonged maternal hypotension and may succumb. Thoracic surgical procedures may have the largest impact on preterm birth risk or pregnancy loss rate outside of abdominal nonobstetric surgery due to the severity of disease that mandates this approach. Cases of cardiopulmonary bypass have been reported with some fetal survival.12
The need for fetal monitoring may be driven by the pathophysiology requiring surgical treatment. For nonemergent surgery, recording fetal heart tones prior to and after surgery will be sufficient in most cases. If there is concern for fetal compromise from obstetric disease, fetal monitoring during surgery may be indicated. If need for fetal delivery during nonemergent, nonobstetric surgery is felt to be likely, then appropriate planning for the obstetric and pediatric teams needs to be included.
PREOPERATIVE WORKUP
Preoperative workup involving laboratory testing and imaging warrants special consideration in pregnancy. The table of normal laboratory values in pregnancy (Table 44.1) can aid in understanding expression of pathophysiology. There are some limits on imaging techniques in pregnancy due to fetal concerns. Ultrasound has been used for diagnostic imaging in pregnancy for several decades with a good safety profile and is typically the modality used first in evaluation of abdominal pathology during pregnancy. Ultrasound energy emission when the unit is set for obstetric imaging is half that of routine abdominal ultrasound. However, routine abdominal settings can still be used to image abdominal organs during pregnancy, as energy transfer to the fetus is minimal in most circumstances. Ionizing radiation from x-ray, computed tomography (CT), and fluoroscopy should be minimized or avoided if possible. If used, shielding of the uterus with a lead apron should occur if feasible. However, CT and x-ray imaging protocols that minimize the amount of radiation used in pregnant patients have been developed, and if critical, timely imaging information is required, they should not be withheld. For counseling purposes, the dose of ionizing radiation that reaches the uterus, and thus the increase in risk of childhood cancer for the fetus, can be estimated; the increase in risk is generally quite low. Magnetic resonance imaging (MRI) does not involve ionizing radiation and is thought to be safe for the fetus by most authorities. The use of MRI in pregnancy has expanded over the last 10 years, and more data are available on its diagnostic accuracy, particularly for nonobstetric abdominal pathology in pregnancy. Diagnostic accuracy for appendicitis in pregnancy approaches 95% with MRI.13 Use of gadolinium in pregnant animals has raised a concern for fetal renal impact, and use in human pregnancy has been studied on a limited basis. Given our current understanding, gadolinium should only be used if the benefit outweighs the risk. Endoscopic and endoultrasonic techniques for gastrointestinal, pulmonary, and cardiac conditions can be done safely in pregnancy. Sedation can be used. However, involvement of an anesthesia provider familiar with anesthesia management in pregnancy may be prudent.
POSTOPERATIVE MANAGEMENT
Postoperative management for a pregnant surgical patient is altered little in most cases. The same postoperative goals of adequate pain control, early ambulation, and judicious advancement of diet should be pursued. Prolonged bladder drainage via catheter should be avoided if possible, as pyelonephritis from ascending infection is more likely in pregnancy. Wound healing is altered for laparotomy incisions, in that the growing uterus will place the incision under constant tension and it may result in a wider cicatrix.
Medications
There are several medications that should be avoided or judiciously used in pregnancy. Antibiotics that should be avoided include fluoroquinolones and tetracycline. Aminoglycosides should be used in the lowest effective dose for the shortest duration to avoid auditory nerve toxicity in the fetus. Narcotic analgesics are the drug class of choice for postoperative pain in a pregnant surgical patient. The lowest dose and shortest duration of narcotic that achieves analgesia adequate to allow ambulation should be used. Such dosing is unlikely to create fetal or maternal dependence for most surgical cases. If prolonged narcotic use is anticipated, then discussion of possible fetal dependence should involve the obstetric and pediatric teams. Nonsteroidal anti-inflammatory medications have limited fetal impact if used for <72 hours below 32 weeks’ gestation, but are generally avoided in favor of oral narcotic analgesics because of their effect on the fetal ductus arteriosus. Thromboprophylaxis should be considered perioperatively, with use of compressive devices advisable in all cases where feasible. If surgical treatment is expected to result in prolonged immobilization, such as lower extremity orthopedic procedures, pharmacologic thromboprophylaxis may be warranted. A hematologist or maternal–fetal medicine specialist should be consulted for appropriate dosing and duration.
GYNECOLOGIC EMERGENCIES
Gynecological emergencies can best be classified into two categories: pregnancy related, and non–pregnancy related. For some conditions that are not directly related to pregnancy, the presence of a positive pregnancy test may make that condition more, or less, likely to be the etiology of the patient’s presenting complaints. Likewise, management decisions may be altered by the presence of a concomitant pregnancy.
Ectopic Pregnancy
An ectopic pregnancy is the implantation of a fertilized ovum outside the endometrial cavity of the uterus. Approximately 95% of these abnormal implantations are in the fallopian tubes. It is the number one cause of death in the first trimester of pregnancy, and accounts for 1 in 10 pregnancy-associated deaths.14 It is a commonly misdiagnosed condition with emergency department (ED) physicians failing to make the diagnosis on an initial visit nearly 50% of the time.15
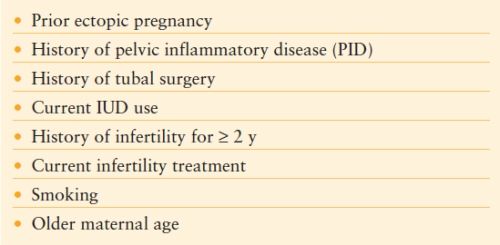
Table 44.2 lists the risk factors for ectopic pregnancy. The two main categories are conditions that result in tubal damage, and a history of infertility or infertility treatments.
TABLE 44.2
RISK FACTORS FOR ECTOPIC PREGNANCY
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


