Nonpharmacologic treatment
Nonpharmacologic treatments for arrhythmias—including pacemakers, implantable cardioverter-defibrillators (ICDs), and radiofrequency ablation—produce distinctive electrocardiogram (ECG) tracings. By understanding how these devices work, and the ECG changes they produce, you’ll be better able to evaluate whether the devices are functioning properly, and you’ll know what to do if they malfunction.
Pacemakers
A pacemaker is an artificial device that electrically stimulates the myocardium to depolarize, initiating mechanical contractions. It works by generating an impulse from a power source and transmitting that impulse to the heart muscle. The impulse flows throughout the heart and causes the heart muscle to depolarize. Pacemakers may be used as a temporary measure or a permanent one, depending on the patient’s condition.
A pacemaker may be used to treat arrhythmias—such as certain bradyarrhythmias and tachyarrhythmias, sick sinus syndrome (SSS), or an atrioventricular (AV) block—as well as following myocardial infarction or cardiac surgery.
Pacemaker fundamentals
Pacemakers consist of three main components: a pulse generator, pacing leads or wires, and one or more electrodes at the distal ends of leadwires. The pulse generator contains the pacemaker’s power source and circuitry. It creates an electrical impulse that moves through the pacing leads to the electrodes, transmitting that impulse to the heart muscle and causing the heart to depolarize.
In a permanent or implanted pacemaker, a lithium battery serves as its power source and lasts between 5 and 10 years. A
microchip in the device guides heart pacing. A temporary pacemaker, which isn’t implanted, is about the size of a small radio or telemetry box and is powered by alkaline batteries. These units also contain a microchip and are programmed by a touch pad or dials.
microchip in the device guides heart pacing. A temporary pacemaker, which isn’t implanted, is about the size of a small radio or telemetry box and is powered by alkaline batteries. These units also contain a microchip and are programmed by a touch pad or dials.
In temporary and permanent pacemakers, an electrical stimulus from the pulse generator moves through wires, or pacing leads, to the electrode tips. The leads for a pacemaker, designed to stimulate a single heart chamber, are placed in either the atrium or the ventricle. For dual-chamber (AV) pacing, the leads are placed in both chambers, usually on the right side of the heart. (See Pacing leads, page 214.)
The electrodes—one on a unipolar lead or two on a bipolar lead—send information about electrical impulses in the myocardium back to the pulse generator. The pulse generator senses the heart’s electrical activity and responds according to how it was programmed.
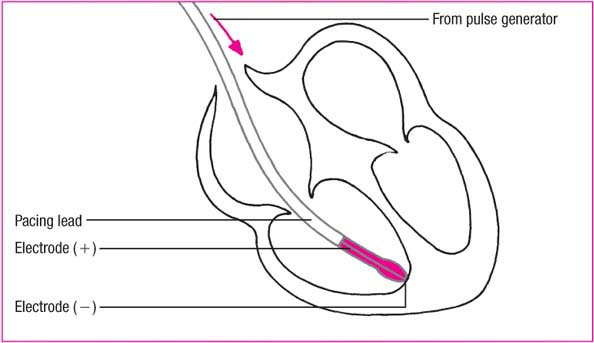
A unipolar lead system is more sensitive to the heart’s intrinsic electrical activity than a bipolar system. A bipolar system isn’t as easily affected by electrical activity, such as skeletal muscle contraction or magnetic fields, originating outside the heart and the generator. A bipolar system is more difficult to implant, however.
Permanent pacemakers
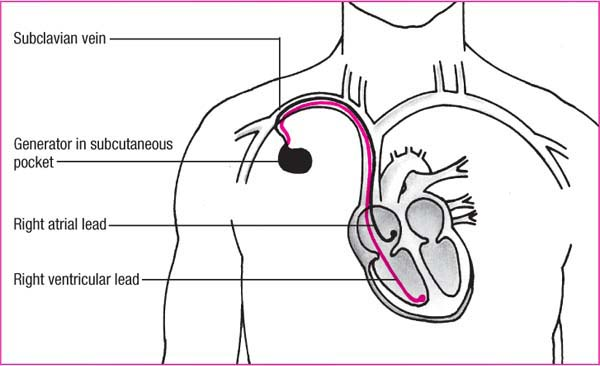
A permanent pacemaker is used to treat chronic heart conditions such as AV block. It’s surgically implanted, usually under local anesthesia. The leads are placed transvenously, positioned in the appropriate chambers, and then anchored to the endocardium. The generator is then implanted in a pocket made from subcutaneous tissue, usually under the clavicle. (See Placing a permanent pacemaker, page 215.)
Most permanent pacemakers are programmed before implantation. The programming sets the conditions under which the pacemaker functions and can be adjusted externally if necessary.
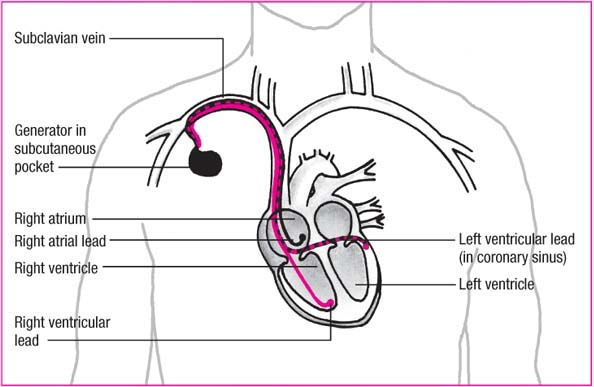
The biventricular pacemaker, a type of permanent pacemaker, uses three leads—one in the right atrium and one in each ventricle. Unlike traditional lead placement, the electrode tip for the left ventricle is placed in the coronary sinus to a branch of the inferior cardiac vein. Because this electrode tip isn’t anchored in place, lead displacement may occur. (See Understanding biventricular pacemakers, page 216, and Biventricular lead placement, page 217.)
Pacing leads
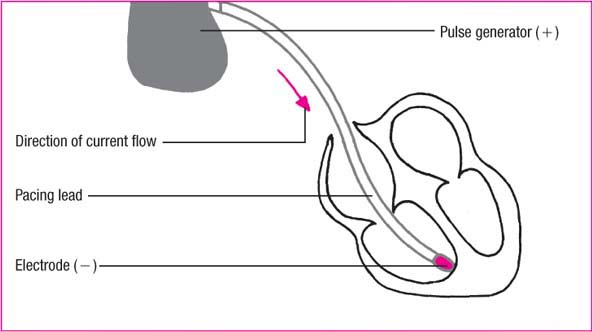
Pacing leads have either one electrode (unipolar) or two (bipolar). These illustrations show the difference between the two leads.
Unipolar lead
In a unipolar system, electric current moves from the pulse generator through the leadwire to the negative pole. From there, it stimulates the heart and returns to the pulse generator’s metal surface (the positive pole) to complete the circuit.
 |
Placing a permanent pacemaker
Implanting a pacemaker is a simple surgical procedure performed with local anesthesia and conscious sedation. To implant an endocardial pacemaker, the cardiologist usually selects a transvenous route and begins lead placement by inserting a catheter percutaneously or by venous cutdown. Then, using fluoroscopic guidance, the cardiologist threads the catheter through the vein until the tip reaches the endocardium.
Lead placement
For lead placement in the atrium, the tip must lodge in the right atrium or coronary sinus, as shown below. For placement in the ventricle, it must lodge in the right ventricular apex in one of the interior muscular ridges, or trabeculae.
Implanting the generator
When the lead is in proper position, the cardiologist secures the pulse generator in a subcutaneous pocket of tissue just below the patient’s clavicle. Changing the generator’s battery or microchip circuitry requires only a shallow incision over the site and a quick exchange of components.
 |
Temporary pacemakers
A temporary pacemaker is commonly inserted in an emergency. The patient may show signs of decreased cardiac output, such as hypotension or syncope. The temporary pacemaker supports the patient until the condition resolves.
A temporary pacemaker can also serve as a bridge until a permanent
pacemaker is inserted. These pacemakers are used for patients with high-grade heart block, bradycardia, or low cardiac output.
pacemaker is inserted. These pacemakers are used for patients with high-grade heart block, bradycardia, or low cardiac output.
Understanding biventricular pacemakers
Biventricular pacing (referred to as cardiac resynchronization therapy) is used to treat patients with moderate to severe heart failure who have left ventricular dyssynchrony.
What happens in heart failure
Under normal conditions, the right and left ventricles contract simultaneously to pump blood to the lungs and body, respectively. However, in heart failure, the damaged ventricles can’t pump as forcefully, and the amount of blood ejected with each contraction is reduced. If the ventricular conduction pathways are also damaged, electrical impulses reach the ventricles at different times, producing asynchronous contractions (intraventricular conduction defect), which further reduces the amount of blood that the heart pumps, worsening the patient’s symptoms.
To compensate for this reduced cardiac output, the sympathetic nervous system releases neurohormones, such as aldosterone, norepinephrine, and vasopressin, to boost the amount of blood ejected with each contraction. The resultant tachycardia and vasoconstriction increase the heart’s demand for oxygen, reduce diastolic filling time, promote sodium and water retention, and increase the pressure that the heart must pump against.
How biventricular pacemakers help
Biventricular pacemakers pace both ventricles at the same time, causing them to contract simultaneously. This coordinates ventricular contractions, which increases cardiac output and improves hemodynamic status. This produces an immediate improvement in the patient’s symptoms and activity tolerance.
Moreover, biventricular pacing improves left ventricular remodeling and diastolic function and reduces sympathetic stimulation. This, in turn, slows the progression of heart failure and improves the patient’s quality of life.
Who are candidates for biventricular pacing?
Not all patients with heart failure benefit from biventricular pacing. Candidates should have systolic heart failure and ventricular dyssynchrony along with the following characteristics:
symptom-producing heart failure despite maximal medical therapy
moderate to severe heart failure (New York Heart Association class III or IV)
QRS complex greater than 0.13 second
left ventricular ejection fraction of 35% or less.
Types of temporary pacemakers
Several types of temporary pacemakers are available, including transvenous, transcutaneous, transthoracic, and epicardial.
Biventricular lead placement
The biventricular pacemaker uses three leads: one to pace the right atrium, one to pace the right ventricle, and one to pace the left ventricle. The left ventricular lead is placed in the coronary sinus. Both ventricles are paced at the same time, causing them to contract simultaneously, improving cardiac output.
 |
Transvenous pacemakers
The transvenous pacemaker is probably the most common and reliable type of temporary pacemaker. It’s inserted through a vein, such as the subclavian or internal jugular vein, at the bedside or in a fluoroscopy suite. The leadwires are advanced through a catheter into the right ventricle or atrium and then connected to the pulse generator.
Transcutaneous pacemakers
Use of an external or transcutaneous pacemaker has become commonplace in the past several years. In this noninvasive method, one electrode is placed on the patient’s anterior chest wall to the right of the upper sternum below the clavicles and a second electrode is applied to his back (anterior-posterior electrodes). An electrode may also be placed to the left of the left nipple with the center of the electrode in the midaxillary line (also called the anterior-apex position). An external pulse generator then emits pacing impulses that travel through the skin to
the heart muscle. Transcutaneous pacing is built into many defibrillators for use in emergencies. In this case, the electrodes are built into the same pads used for defibrillation.
the heart muscle. Transcutaneous pacing is built into many defibrillators for use in emergencies. In this case, the electrodes are built into the same pads used for defibrillation.
Transcutaneous pacing is a quick, effective method of pacing heart rhythm and is commonly used in emergencies until a transvenous pacemaker can be inserted. However, some patients can’t tolerate the irritating sensations produced from prolonged pacing at the levels needed to pace the heart externally. If hemodynamically stable, these patients may require sedation.
Transthoracic pacemakers
A transthoracic pacemaker is a type of temporary ventricular pacemaker only used during cardiac emergencies as a last resort. Transthoracic pacing requires insertion of a long needle into the right ventricle, using a subxiphoid approach. A pacing wire is then guided directly into the endocardium.
Epicardial pacemakers
Epicardial pacemakers are commonly used for patients undergoing cardiac surgery. The tips of the leadwires are attached to the heart’s surface and then the wires are brought through the chest wall, below the incision. Finally, they’re attached to the pulse generator. The leadwires are usually removed several days after surgery or when the patient no longer requires them.
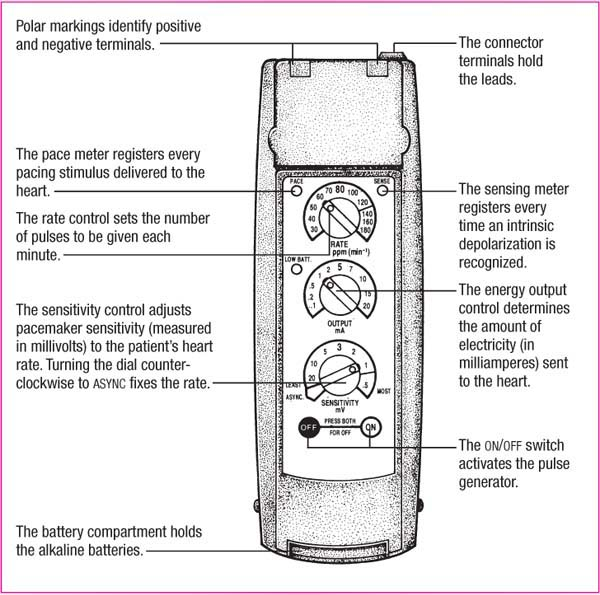
Temporary pacemaker settings
A temporary pacemaker has several types of settings on the pulse generator. The rate control regulates how many impulses are generated in 1 minute and is measured in pulses per minute (ppm). The rate is usually set at 60 to 80 ppm. (See Temporary pulse generator.) The pacemaker fires if the patient’s heart rate falls below the preset rate. The rate may be set higher if the patient has a tachyarrhythmia being treated with overdrive pacing.
A pacemaker’s energy output is measured in milliamperes (mA), a measurement that represents the stimulation threshold, or how much energy is required to stimulate the cardiac muscle to depolarize. The stimulation threshold is sometimes referred to as energy required for capture.
You can also program the pacemaker’s sensitivity, measured in millivolts. Most pacemakers allow the heart to function naturally and assist only when necessary. The sensing threshold allows the pacemaker to do this by sensing the heart’s normal activity.
ECG characteristics
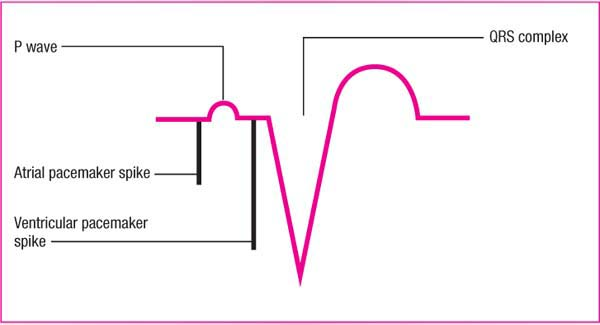
The most prominent characteristic of a pacemaker on an ECG is the pacemaker spike that occurs when the pacemaker sends an electrical impulse to the heart muscle. (See Pacemaker spikes, page 220.) The impulse appears as a vertical line, or spike. The collective group of spikes on an ECG is called pacemaker artifact.
Depending on the electrode’s position in the heart, the spike appears in different locations on the waveform:
When the pacemaker stimulates the atria, the spike is followed by a P wave and the patient’s baseline QRS complex and
T wave. This series of waveforms represents successful pacing, or capture, of the myocardium. The P wave appears different from the patient’s normal P wave.
When the ventricles are stimulated by a pacemaker, the spike is followed by a QRS complex and a T wave. The QRS complex appears wider than the patient’s own QRS complex because of how the pacemaker depolarizes the ventricles.
When the pacemaker stimulates the atria and ventricles, the spike is followed by a P wave, then a spike, and then a QRS complex. Be aware that the type of pacemaker used and the patient’s condition may affect whether every beat is paced.
Knowing your patient’s medical history and whether a pacemaker has been implanted also helps you to determine whether your patient is experiencing ventricular ectopy or paced activity on the ECG. (See Distinguishing intermittent ventricular pacing from PVCs.)
Pacemaker modes
Pacemakers have two basic modes for pacing: synchronous and asynchronous. In synchronous, or demand, pacing, the pacemaker initiates electrical impulses
only when the heart’s intrinsic heart rate falls below the preset rate of the pacemaker. In asynchronous, or fixed, pacing,
the pacemaker constantly initiates electrical impulses at a preset rate without regard to the patient’s intrinsic electrical activity or heart rate. Asynchronous pacing is rarely used.
only when the heart’s intrinsic heart rate falls below the preset rate of the pacemaker. In asynchronous, or fixed, pacing,
the pacemaker constantly initiates electrical impulses at a preset rate without regard to the patient’s intrinsic electrical activity or heart rate. Asynchronous pacing is rarely used.
 Look-Alikes
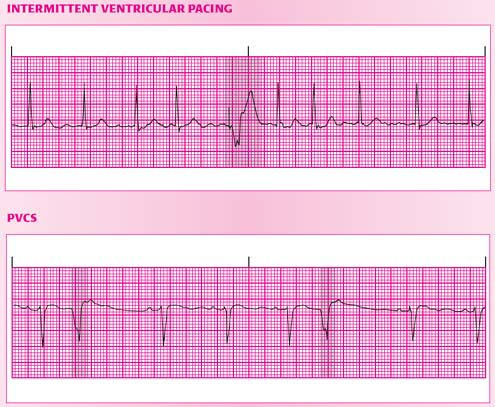
Look-AlikesDistinguishing intermittent ventricular pacing from PVCs
Knowing whether your patient has an artificial pacemaker helps you avoid mistaking a ventricular paced beat for a premature ventricular contraction (PVC). If your facility uses a monitoring system that eliminates artifact, make sure the monitor is set up correctly for a patient with a pacemaker. Otherwise, the pacemaker spikes may be eliminated as well.
If your patient has intermittent ventricular pacing, the paced ventricular complex will have a pacemaker spike preceding it, as shown in the shaded area of the top electrocardiogram (ECG) strip. You may need to look in different leads for a bipolar pacemaker spike because it’s small and may be difficult to see. What’s more, the paced ventricular complex of a properly functioning pacemaker won’t occur early or prematurely, it will occur only when the patient’s own ventricular rate falls below the rate set for the pacemaker.
If your patient is having PVCs, they’ll occur prematurely and won’t have pacemaker spikes preceding them. Examples are shown in the shaded areas of the bottom ECG strip.
 |
Pacemaker description codes
Pacemakers use a uniform code system to describe how they’re programmed. This system consists of five letters that indicate the chamber paced, the chamber sensed, the response to sensing, the programmability, and antiarrhythmia function. (See Pacemaker coding systems.)
Although the coding system consists of five letters, a three-letter code is typically used to describe pacemaker function. Pacemaker codes include AAI, VVI, DVI, and DDD.
AAI
The AAI, or atrial demand, pacemaker is a single-chambered pacemaker that paces and senses the atria. When the pacemaker senses intrinsic atrial activity, it inhibits pacing and resets itself.
Because AAI pacemakers require a functioning AV node and intact conduction system, they aren’t used in AV block. An AAI pacemaker may be used in patients with sinus bradycardia, which may occur after cardiac surgery, or with SSS, as long as the AV node and His-Purkinje system aren’t diseased.
VVI
The VVI, or ventricular demand, pacemaker paces and senses the ventricles. When it senses intrinsic ventricular activity, it inhibits pacing.
This single-chambered pacemaker benefits patients with complete heart block and those needing intermittent pacing. Because it doesn’t affect atrial activity, it’s used for patients who don’t need an atrial kick—the extra 15% to 30% of cardiac output that comes from atrial contraction.
If a patient has spontaneous atrial activity, a VVI pacemaker won’t synchronize the ventricular activity with it, so tricuspid and mitral insufficiency may develop. Sedentary patients may receive this pacemaker, but it won’t adjust its rate for more active patients. (See AAI and VVI pacemakers, page 224.)
DVI
The DVI, or AV sequential, pacemaker paces the atria and ventricles. This dual-chambered pacemaker senses only the ventricles’ intrinsic activity, inhibiting ventricular pacing.
Two types of DVI pacemakers may be used, a committed DVI and a noncommitted DVI pacemaker. The committed DVI pacemaker
doesn’t sense intrinsic activity during the AV interval—the time between an atrial and ventricular spike. It generates an impulse even with spontaneous ventricular depolarization. The noncommitted DVI pacemaker, on the other hand, is inhibited if a spontaneous depolarization occurs. (See DVI pacemaker rhythm strip, page 225.)
doesn’t sense intrinsic activity during the AV interval—the time between an atrial and ventricular spike. It generates an impulse even with spontaneous ventricular depolarization. The noncommitted DVI pacemaker, on the other hand, is inhibited if a spontaneous depolarization occurs. (See DVI pacemaker rhythm strip, page 225.)
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


