Chapter 15 Nonintubation Management of the Airway
Airway Maneuvers and Mask Ventilation
I Overview
A Upper Airway Anatomy and Physiology
Nonintubation airway management seeks to produce patency to gas flow through the oropharynx, nasopharynx, and larynx without the use of artificial airway devices that extend into the laryngopharynx or trachea. A thorough understanding of upper airway anatomy and physiology is necessary to appreciate the therapeutic maneuvers and devices employed in airway management (Fig. 15-1). More detailed reviews of airway anatomy are found elsewhere in this book and in various atlases and texts.1–3
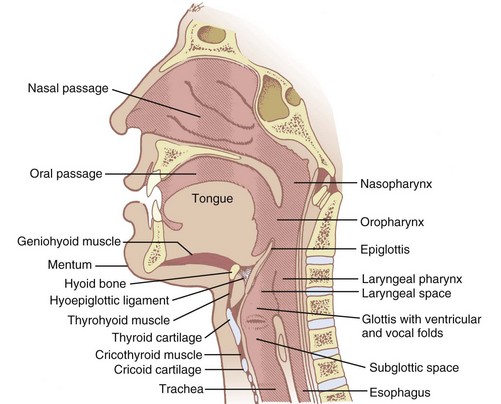
Gas passes from outside the body to the larynx through the nose or mouth. If through the nose, ambient gas passes through the nares, choanae, and nasopharynx (where it is warmed and humidified). The humidified gas then traverses the oropharynx and hypopharynx (also called laryngopharynx) on its way to the larynx. If through the mouth, the oropharynx and hypopharynx are traversed before entering the glottis. Nasal passages can be obstructed by choanal atresia, septal deviation, mucosal swelling, or foreign material (e.g., mucus, blood). Entry to the oropharynx can be blocked by the soft palate lying against the posterior pharyngeal wall. The pathway of gas by either route can be restricted by the tongue in the oropharynx or the epiglottis in the hypopharynx. These are sites of potential pharyngeal collapse.4–7 Airway manipulation and devices can remedy these causes of obstruction. Laryngeal obstruction related to spasm, however, must be treated by positive airway pressure, deeper anesthesia, muscle relaxants, or endotracheal intubation.
Laryngeal closure is accomplished by the intrinsic or extrinsic muscles of the larynx. Tight closure, as seen in laryngospasm, results from contraction of the external laryngeal muscles, which force the mucosal folds of the quadrangular membrane into apposition (Fig. 15-2). Muscle groups also extend from the thyroid cartilage to the hyoid and cricoid cartilages. When they contract, the interior mucosa and soft tissue (ventricular and vocal folds) are forced into the center of the airway, and the thyroid shield is deformed (compressed inward), providing a spring to reopen the airway rapidly after these muscles relax.8 The larynx closes at the level of the true cords by action of the intrinsic muscles of the larynx during phonation, but this closure is not as tight as the laryngospasm described earlier.
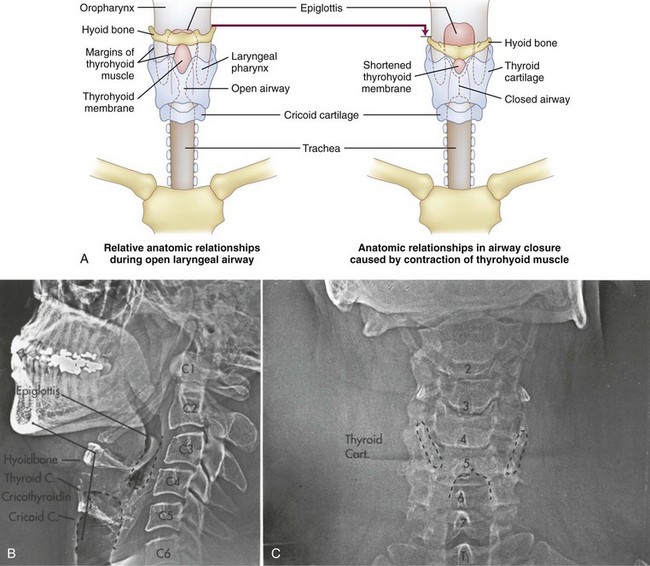
Opening of the pharynx and larynx is achieved by elongating and unfolding the airway from the hyoid to the cricoid cartilage.8 Several muscle groups tether the various airway structures to one another to form a functional airway apparatus. When the head is tilted, the chin and mandible are displaced forward on the temporomandibular joint. This produces maximum stretch at the hyoid-thyroid-cricoid area. The hyoid bone is pulled in an anterior direction along with the epiglottis and base of the tongue, which opens the oropharynx. The ventricular and vocal folds flatten against the sides of the thyroid cartilage, opening the laryngeal airway.8
B Upper Airway Obstruction
1 Pharyngeal Obstruction
In patients susceptible to obstructive sleep apnea, the geometry of the pharynx can be altered during normal sleep.9 Although it is usually oval with the long axis in the transverse plane, the pharynx in patients with obstructive sleep apnea is round or oval with the long axis in the anterior-posterior plane (the lateral walls are thickened).10,11 This obstruction can often be treated effectively with nasal continuous positive airway pressure and with intraoral devices that advance the mandible as much as the jaw thrust maneuver.12–14
2 Hypopharyngeal Obstruction
Hypopharyngeal obstruction has been investigated by placing a nasal fiberscope at the level of the soft palate in anesthetized subjects.15 The epiglottis and the glottic opening can be seen, recorded, and analyzed. The percentage of glottic opening (POGO) seen from this view can be determined. Typically, airflow increases and snoring decreases as POGO increases. However, a POGO of 100% has been documented with airway occlusion, and a POGO of 0% has been documented with no stridor and no obvious impairment to ventilation. Although less than perfect, these evaluations do support the potential for airflow restriction at the hypopharynx and are consistent with the cause being the epiglottis obstructing the airway.
II Nonintubation Approaches to Establish Airway Patency
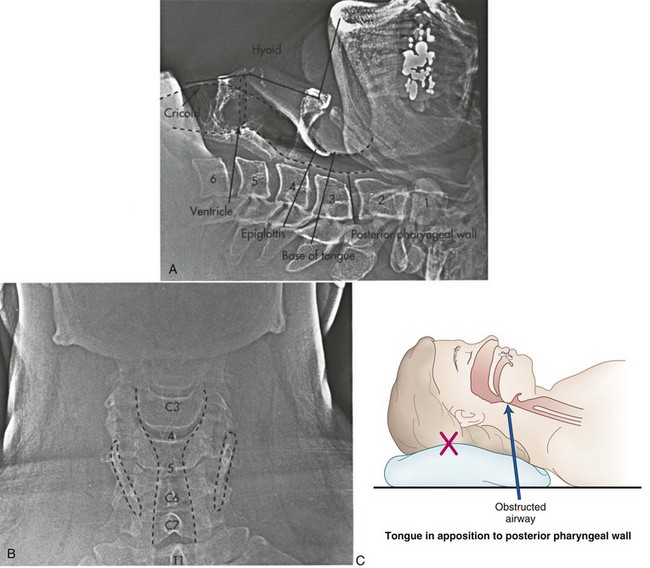
When the muscles of the floor of the mouth and tongue relax, the tongue may cause soft tissue obstruction by falling back onto the posterior wall of the oropharynx. It is also possible for the epiglottis to overlie and obstruct the glottic opening or to seal against the posterior laryngopharynx. This effect can be exaggerated by flexing the head and neck or opening the mouth, or both (Fig. 15-3), because the distance between the chin and the thyroid notch is relatively short in the flexed position. Any intervention that increases this distance straightens the mentum-geniohyoid-hyoid-thyroid line and therefore elevates the hyoid bone further from the pharynx. The elevated hyoid then secondarily elevates the epiglottis through the hyoepiglottic ligament, potentially alleviating the obstruction.
A Simple Maneuvers for the Native Airway
1 Head Tilt-Chin Lift
The head tilt-chin lift is accomplished by tilting the head back on the atlanto-occipital joint while keeping the mouth closed (teeth approximated) (Fig. 15-4). This technique may be augmented by elevating the occiput 1 to 4 inches above the level of the shoulders (sniffing position) as long as the larynx and posterior pharynx stay in their original position. The head tilt-chin lift is the simplest and first airway maneuver used in resuscitation, but it should be used with extreme caution in patients with suspected neck injuries.
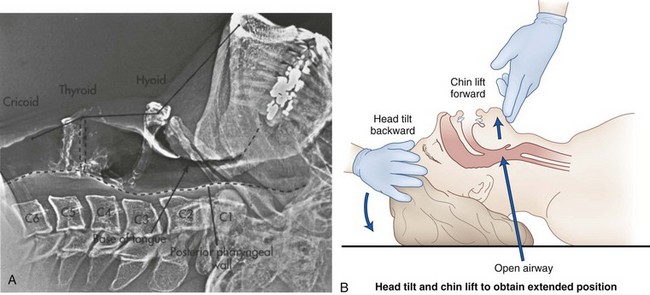
Figure 15-4 A, Lateral xerogram of the head and neck shows the extended position (head tilt) in an awake and supine patient (compare with Fig. 15-3A). The mentum is superior to the hyoid bone, the base of the tongue and the epiglottis are farther from the posterior pharyngeal wall, and the thyroid and cricoid cartilages are at the C4-5 level. The hyoid bone has been raised and elevated from C3-4 to C2-3. B, Diagram of the head tilt-chin lift maneuver.
2 Jaw Thrust
The jaw thrust maneuver more directly lifts the hyoid bone and tongue away from the posterior pharyngeal wall by subluxating the mandible forward onto the sliding part of the temporomandibular joint (mandibular advancement) (Fig. 15-5). The occluded teeth normally prevent forward movement of the mandible, and the thumbs must depress the mentum while the fingers grip the rami of the mandible and lift it upward. This results in the mandibular teeth protruding in front of the maxillary teeth (after the mouth opens slightly). In practice, the insertion of a small airway sometimes makes this procedure easier because it separates the teeth, allowing the mandible to more easily slide forward. In most people, the mandible is readily drawn back into the temporomandibular joint by the elasticity of the joint capsule and masseter muscles. Consequently, this position can be difficult to maintain with one hand.
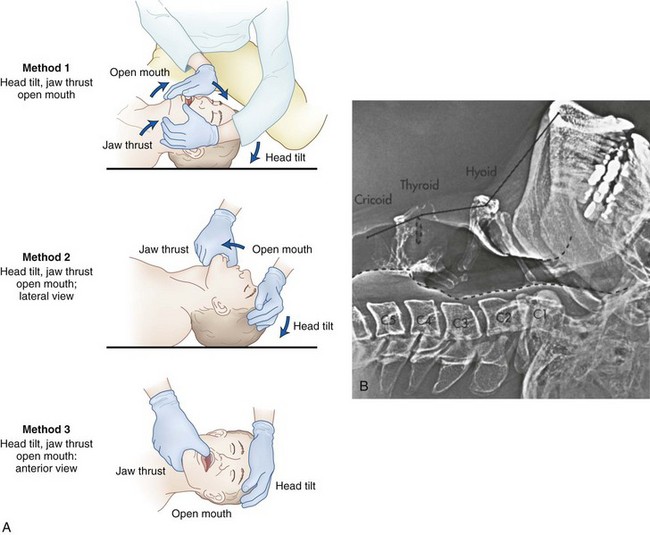
Figure 15-5 The triple airway maneuver includes the head tilt-chin lift, jaw thrust, and open mouth. A, Diagrams show three methods of performing the maneuver: (1) the head extended on the atlanto-occipital joint, (2) the mouth opened to take the teeth out of occlusion, and (3) the mandible lifted upward, forcing the mandibular condyles anteriorly at the temporomandibular joint. B, Lateral xerogram of the head and neck show the extended position with jaw protrusion (compare with Figs. 15-3A and 15-4A). Notice that the mandibular incisors protrude beyond the maxillary incisors and that the mandibular condyles are subluxated anteriorly from the temporomandibular joint.
In up to 20% of patients, the nasopharynx is occluded by the soft palate during exhalation when the airway muscles are relaxed. If the mouth and lips are also closed, exhalation is impeded. In these cases, the mouth must be opened slightly to ensure that the lips are parted. When the head tilt-chin lift, jaw thrust, and open mouth maneuvers are done together, it is known as the triple airway maneuver (see Fig. 15-5). The triple airway maneuver is the most reliable manual method to achieve patency of the native upper airway (Box 15-1).
Box 15-1 Simple Maneuvers for the Native Airway
Head Tilt-Chin Lift
Procedure: With the patient supine, place one hand on the forehead and the first two fingers of the other hand on the underside of the chin. Simultaneously exert upward traction on the chin while tilting the forehead gently backward to extend the head on the atlanto-occipital joint.
Indications: Soft tissue upper airway obstruction
Contraindications: Cervical spine fracture, basilar artery syndrome, infants
Jaw Thrust
Procedure: From above the patient’s head, place the thumbs on the chin and the fingers behind the angle of the jaw bilaterally. Simultaneously open, lift, and displace the jaw forward, subluxating the mandible anteriorly on the temporomandibular joint.
Indications: Soft tissue airway obstruction when a head tilt-chin lift is contraindicated (e.g., fractured neck) or ineffective
Contraindications: Fractured or dislocated jaw, awake patient
Triple Airway Maneuver
Procedure: Perform the head tilt-chin lift followed by a jaw thrust maneuver. Maintain the mouth in an open position after subluxating the mandible during the jaw thrust.
Indications: Expiratory obstruction after a head tilt-chin lift and jaw thrust
Contraindications: Same as for a head tilt-chin lift and jaw thrust
Complications: Same as for a head tilt-chin lift and jaw thrust
3 Heimlich Maneuver
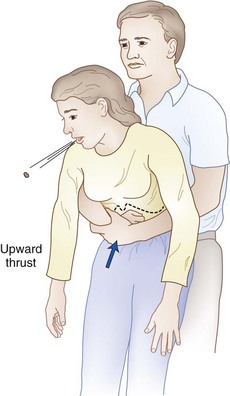
Airway maneuvers can aid in establishing and maintaining airway patency, but they do not relieve an obstruction due to foreign material lodged in the upper airway. Foreign body obstruction should be suspected after a witnessed aspiration when the patient cannot speak, when spontaneous ventilation is absent, or when PPV remains difficult after routine airway maneuvers have been performed. A Heimlich maneuver (subdiaphragmatic abdominal thrusts) is recommended when coughing or traditional means, such as back blows, are unable to relieve complete airway obstruction due to foreign material (Fig. 15-6 and Box 15-2). The goal is to increase intrathoracic pressure sufficiently to simulate a cough. Alternatively, a forceful chest compression in the manner of a rapidly executed bear hug (for upright patients) or a sternal compression (for supine patients) can also be effective. In emergency situations, the failure of one technique to relieve an obstruction should not preclude additional attempts using the various alternatives.
Box 15-2 The Heimlich Maneuver
Procedure: In the upright patient, wrap both arms around the chest with the right hand in a closed fist in the low sternal-xiphoid area and the left hand on top of the fist. With a rapid, forceful thrust, compress upward, increasing subdiaphragmatic pressure and creating an artificial cough.
Indication: Complete upper airway obstruction by a foreign body with impending asphyxia
Contraindications: Partial airway obstruction, fractured ribs (relative), cardiac contusion (relative)
Complications: Fractured ribs or sternum, trauma to liver, spleen, or pancreas
B Artificial Airway Devices
1 Oropharyngeal Airways
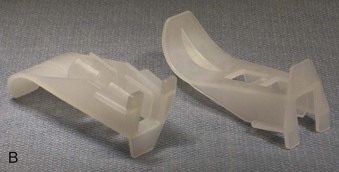
An oropharyngeal airway (OPA) is the most commonly used device to provide a patent upper airway. OPAs are manufactured in a wide variety of sizes from neonatal to large adult, and they are typically made of plastic or rubber (Fig. 15-7). They should be wide enough to make contact with two or three teeth on each of the mandible and maxilla, and they should be slightly compressible so that the pressure exerted by a clenched jaw is distributed over all of the teeth while the lumen remains patent. OPAs are frequently designed with a flange at the buccal (proximal) end to prevent swallowing or over insertion. They also feature a distal semicircular section to follow the curvature of the mouth, tongue, and posterior pharynx so that the tongue is displaced anteriorly (concave side against the tongue). An air channel is often provided to facilitate oropharyngeal suctioning.

Related posts:
 Prehospital Airway Management
Prehospital Airway Management
 Medical-Legal Considerations: The ASA Closed Claims Project
Medical-Legal Considerations: The ASA Closed Claims Project
 Performance of Rigid Bronchoscopy
Performance of Rigid Bronchoscopy
 Intubating Introducers, Stylets, and Lighted Stylets (Lightwands)
Intubating Introducers, Stylets, and Lighted Stylets (Lightwands)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


