Fig. 70.1
(1) Joint capsule of the metatarsophalangeal joint, (2) capsule of the articulatio hallucis (3) metatarsophalangeal joint,(4) collateral ligaments (Reproduced with permission from Dr. Danilo Jankovic)
Indications
Rheumatology (rheumatoid arthritis, gouty arthritis)
Orthopedics (hallux rigidus, hallux valgus, pain in the metatarsophalangeal joint of the hallux, hallucal sesamoid pain)
Procedure
Patient Positioning
Supine position with flexed knee joint, or sitting (with the foot placed on a small footstool).
Materials
Sterile precautions, fine 25-mm-long 26-G needle, swabs, compresses, tuberculin syringe, local anesthetic, glucocorticoid if needed
Strict Asepsis
Thorough and broad skin disinfection, drying and covering of the injection site with a fenestrated drape. Local anesthesia (skin infiltration)
Injection Techniques
Landmark Based [1, 5, 6]
The articular space can be palpated during movement of the large toe (Fig. 70.2). The needle is introduced horizontal to the surface of the skin between the head of metatarsal I and the base of the proximal phalanx of the great toe (Fig. 70.2). The depth of injection is 0.5–1.0 cm. The injection must only be carried out when there is no resistance.

Fig. 70.2
Metatarsophalangeal joint. Injection. The needle is introduced horizontal to the surface of the skin between the head of metatarsal I and the base of the proximal phalanx of the great toe (Reproduced with permission from Dr. Danilo Jankovic)
Ultrasound Guidance
The accuracy of landmark-guided technique is at best 65 %, while the accuracy for ultrasound guidance is 100 % [4, 7–9]. A linear probe with a small footprint (6–13 MHz) is used and applied to the dorsal aspect of metatarsophalangeal joint just medial to the extensor hallucis longus tendon (Fig. 70.3). The needle is introduced out-of-plane from medial to lateral [4]. A successful injection will result in spread of the injectate to the first metatarsophalangeal joint recess.
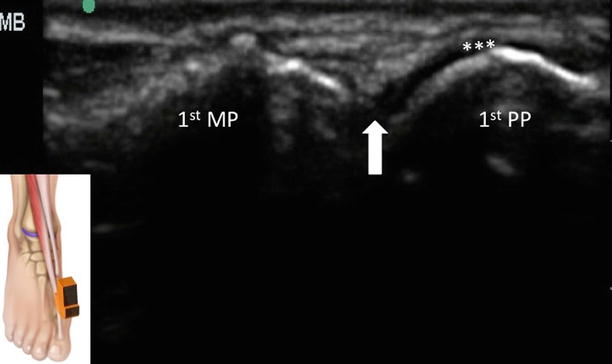
Fig. 70.3
Sonography of the long axis view of the first metatarsophalangeal joint (MTPJ). The ultrasound probe position was indicated in the insert in the left lower corner. The MTPJ was indicated by the bold arrow. 1st PP first proximal phalanx, 1st MT first metatarsal, ** metatarsophalangeal joint recess (Reproduced with permission from Philip Peng Educational Series)
Dosage
1.0–1.5 mL local anesthetic — e.g., 0.5–0.75 % ropivacaine (mixed with 20 mg methylprednisolone if appropriate)
Side Effects and Complications
Infection (prophylaxis: strictest possible asepsis)
Injury to cartilage or bone
A temporary increase in pain may occur in approximately 25 % of the patients (who should be informed about this
Hematoma formation
Injections of the Morton’s Neuroma
In 1935, Dudley Morton described two structural variants of the foot skeleton that are regularly found either individually or together in patients who report metatarsalgia [6, 10–12].
The most frequent variant was hypermobility of metatarsal I (in the tarsometatarsal joint) with simultaneously slack long plantar ligaments. The hypermobility of metatarsal I overstrains the tibialis posterior and flexor digitorum longus muscles.
Metatarsalgia is not an anatomic diagnosis. Primary metatarsalgia can be triggered by the following factors: static, congenital, hallux valgus, or surgical procedures. Secondary metatarsalgia can be provoked by trauma, sesamoiditis, or neurogenic diseases [6, 10].
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


