CHAPTER 49

MECHANICAL VENTILATOR SUPPORT
The respiratory system is responsible for both oxygenation and ventilation. Oxygenation is the ability to provide oxygen to the tissues. Ventilation is the removal of carbon dioxide via the lungs to maintain a neutral pH. When the ability to breathe is compromised, whether it is secondary to hypoxia, acidosis, injury, oversedation, somnolence, muscle fatigue, or other issues, supplemental and artificial modes must be employed in order to provide adequate oxygenation and ventilation; these methods will be discussed.
NONINVASIVE VENTILATION
As part of the evaluation and treatment of patients, there are a number of adjuncts that can be utilized in an attempt to preclude the need for intubation with an artificial airway and mechanical ventilation.1 To address hypoxemia, supplemental oxygen should be initiated.
The basic form of oxygen supplementation is via a nasal cannula. Oxygen is delivered through prongs that are inserted into the nares and can be regulated between a low flow (1–2 L/minute) and a high flow concentration (10 L/minute), although the higher flow rates can be uncomfortable for a patient. Flows up to 20 L/min with humidification have also been used to create a continuous positive airway pressure (CPAP) effect as well. This oxygen supply is either from a wall source via a regulator or from an oxygen tank. Caution must be exercised in patients with end-stage or chronic pulmonary disease as many of these patients rely on hypoxia to provide their respiratory drive. Providing too high an arterial oxygen saturation can abolish this drive.
If a nasal cannula is inefficient in oxygen delivery, that is, delivery of oxygen to a mouth breather, other modalities may be employed. Oxygen delivery via a face mask is a simple means to improve oxygenation in a patient. Oxygen flow from a wall circuit or a specialized tank can increase the concentration of oxygen in inspired air to approximately 55%. Openings on the side of the mask allow removal of CO2 without effort. However, if an individual’s tidal volume (TV) is high, room air may be entrained into the mask, thus diminishing the enriched oxygen concentration. To diminish this latter effect, the patient may be switched to a venturi mask. This apparatus is similar in appearance to a face mask, but has one way valves replacing the openings on the side of the mask. This allows an increase in enriched oxygen concentrations up to 80% at the tertiary bronchioles, as well as CO2 removal. Another less frequently used noninvasive oxygen delivery system is a face tent. This fits below the chin and oxygen flow is directed into the oral and nasal passages without the mask actually touching the face. This is particularly useful in patients with burns, macerated facial skin, etc. and can provide up to 50% oxygen concentration levels.
Higher concentrated levels of oxygen can be provided by CPAP or bilevel positive airway pressure mask. This is a mask that is firmly secured over the nose and/or mouth, and delivers concentrated oxygen under positive pressure. Prior to initiation of this treatment, the patient should be awake, able to cough and may require gastric decompression via a nasogastric tube. This is done to avoid gastric distension and aspiration resulting from the aerophagia generated from the provided pressure.
MECHANICAL VENTILATION
Ventilation using mechanical means has seen changes from a century ago when the use of negative pressure ventilation and the so called “iron lung” was utilized during the polio epidemic. This has progressed to the current usage of positive pressure ventilation with digital rather than analogue technology. Advanced computer technology incorporating patient data and operator data, coupled with pharmacomanipulation and ancillary assistance described below has also led to the improvement of mechanical ventilation.2–6
Ventilation–perfusion ratio (V/Q) looks at oxygen consumption and CO2 production. It assumes that there is a near linear relationship between CO2 and PCO2. Alveolar–capillary gas transport can be expressed as DO2I = (SaO2 × Hb × 1.34) + (0.0031 × PaO2) × CI × 10 where DO2I is oxygen delivery index and normal values are 500–600 mL O2/min/m2. Oxygen consumption is generally 25% of oxygen delivery and together give rise to the extraction ratio or A-VO2 difference, with normal being 5 mL O2/dL of blood. In times of high O2 demands, the normal tissues can extract 50% or more O2 from the blood. In various conditions however, such as SIRS, the extraction is less.
Ventilation
The ventilator circuit is approximately 60 inches of corrugated plastic tubing connecting the ventilator to the artificial patient airway, for example, an endotracheal (ET) or tracheostomy tube. The circuit may contain filters, humidifiers, water traps, heated wires, artificial noses, closed suction catheters, and devices for aerosol administration or capnography and is directly connected to the ventilator.
To determine acceptable placement of the ET tube, a colorimetric CO2 detector may be used. This device has a pH-sensitive chemical bonded to a specialized paper element that changes color with ventilation in the presence of CO2. During CPR this detector is of limited value. The cardiac output, and thus the pulmonary blood flow, may both be diminished and CO2 may not be exchanged, let alone exhaled. Another device available to verify ET tube placement into the trachea is the esophageal detection device. Negative pressure applied at the end of the artificial airway allows the bulb to inflate if the ET tube is in the trachea on inspiration. This relies on the fact that with inspiration the lungs are distended and the esophagus is collapsed and thus the bulb will not fill if the ET tube is in the esophagus, unless the patient has had a large amount of gas insufflated into the esophagus such as from manual ventilation.
Aside from the traditional ET tube, tubes impregnated with silver and tubes with a supraglottic suction port to prevent secretions from contaminating the respiratory tree, have been used. Both adjuncts add considerable cost to the tubes with little proven benefit.
The cycle of respiration using mechanical ventilation consists of the following steps:
- A trigger either by the patient or the machine to initiate a breath may be in the form of a set time, pressure, or volume.
- The volume or pressure goal, if set, is reached and may also be influenced by flow sensitivity.
- Then based on whether volume cycled, time cycled, flow cycled, or pressure cycled, the inspiratory phase is completed and there may be a pause.
- The exhalation phase then begins, which in most cases is passive and dependent in part on pulmonary compliance and airway and equipment resistance, the product of which is called the time constant (Tc).
Terms Utilized for Mechanical Ventilation
- TV is the amount of air the patient inspires or is delivered by the ventilator during an inspiration (mL).
- Respiratory rate or frequency is the number of breaths per minute and may include the patient’s breaths, the ventilator breaths or both.
- Minute volume ventilation (MVV) is the product of the TV and the frequency (L/minute).
- Peak airway pressure (Paw) is the pressure required to deliver the set TV to the patient (cm H2O).
- Plateau pressure (Pplat) is the pressure necessary to distend the lung at end inspiration (cm H2O).
- Mean airway pressure (Maw) is the average pressure delivered (cm H2O).
- Inspiratory time (IT) is the number of seconds required to deliver a set TV.
- Peak inspiratory flow is the highest flow during the inspiratory phase used to deliver the set TV (L/min).
- FiO2 is the fraction of inspired oxygen or the concentration of inspired oxygen gas with 0.21 (21%) being room air and 1.0 (100%) being the maximum short of using a hyperbaric chamber.
- Compliance is the change in volume divided by the change in transthoracic pressure.
- Elastance is the change in transthoracic pressure divided by the change in volume.
- Resistance is the ratio of change in pressure to change in volume.
- Static compliance is the ability of the alveoli to expand with increasing volume or pressure and is measured in a no-flow condition. It is expressed as the ratio of the change in volume over the change in alveolar pressure. Dynamic compliance is the same ratio while flow is occurring. The opposite of compliance is elastance.
Modes of Mechanical Ventilation
Mechanical ventilators operate via one of two modes: pressure control or volume control (Table 49.1). Pressure control is a mode of ventilation where the pressure delivered with each breath is constant.7 Volume control ventilation is a mode where the volume of each breath delivered remains constant. Dual control implies that breaths are a combination of volume and pressure control. There are wide ranges of other modes of mechanical ventilation, which are detailed below (Table 49.2):
TABLE 49.1
CONTROLLED MANDATORY VENTILATION VS. PRESSURE CONTROLLED VENTILATION
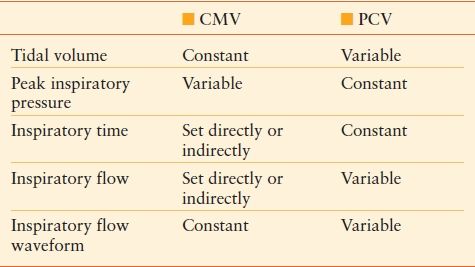
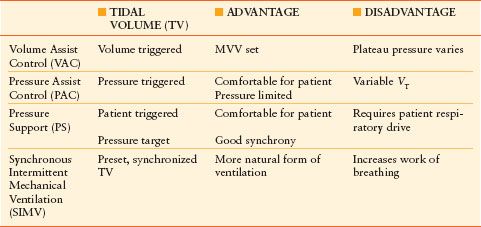
TABLE 49.2
BASIC MODES OF MECHANICAL VENTILATION
CMV is continuous mandatory ventilation in which all breaths are delivered by the ventilator at a minimum preset frequency to a preset volume (Table 49.1). It is rarely used today as it is considered an unnatural form of ventilation, and thus should only be considered in patients who are chemically paralyzed.
ACV is assist–control ventilation in which a set volume is delivered at a set minimum frequency. In addition, the patient can trigger the ventilator to deliver an additional breath at the preset volume or pressure above the preset frequency.
IMV is intermittent mandatory ventilation in which the machine breaths are delivered at a set frequency, volume, and pressure.8 Any additional breaths are spontaneous with patient generated volumes or pressure. This form of ventilation is primarily utilized in the NICU.
SIMV is synchronized intermittent mandatory ventilation where the ventilator delivered breath is presented within a preset time, preferably in concert with the patient’s inspiratory effort. If there is little or no spontaneous breathing, a time triggered breath is delivered in the absence of a patient generated breath. Patients can be weaned from this mode of ventilation.
PSV is pressure support ventilation in which the patient’s inspiratory effort is assisted by the ventilator to a preset pressure. This mode of ventilation is patient triggered, pressure limited, and flow cycled, allowing patients to set their own frequency, IT, and volume. Patients can be weaned from this mode of ventilation (Algorithm 49.1).
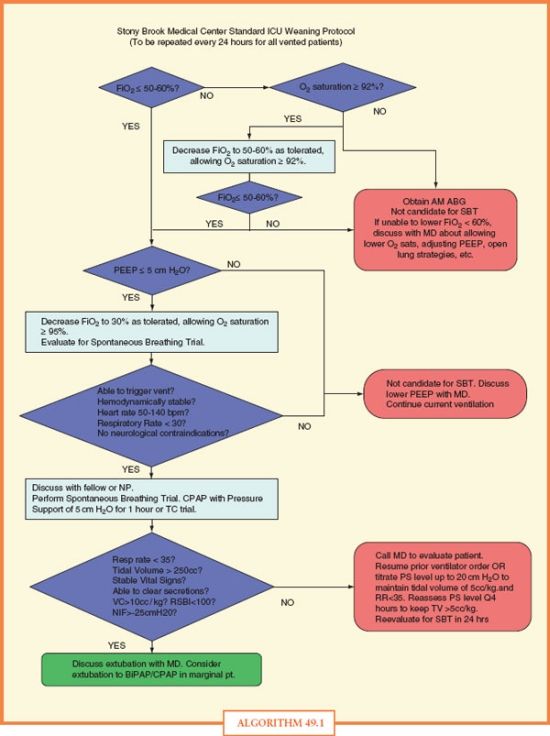
ALGORITHM 49.1 Stony Brook Medical Center Standard ICU Weaning Protocol. To be repeated every 24 hours for all vented patients.
CPAP is continuous positive airway pressure where a constant level of positive pressure is set while the patient is breathing spontaneously. This mode can be used prior to extubation or decannulation of a mechanically ventilated patient.
APRV is airway pressure release ventilation that allows spontaneous breathing. The patient ventilates with a high pressure (Phi) level, which is essentially CPAP, and during the inspiratory phase the Phi is released at a set low pressure level (Plo). The time spent at each level of ventilation is the Thi or the IT and Tlo, which is the expiratory time. The spontaneous breaths are pressure controlled, pressure triggered, pressure limited, and pressure cycled. APRV allows spontaneous breaths during the inflation period. This mode is attractive in that it may limit acute lung injury (ALI) by decreasing maximal pressures and increasing mean pressures, thus improving oxygenation.9–11
PCIRV is pressure controlled inverse ratio ventilation and is a time triggered, pressure limited, and time cycled mode of ventilation in which all breaths are mandatory.7 This mode generally has inspiration times longer than exhalation. When spontaneous breathing is absent this is similar to APRV.
PRVC is pressure-regulated volume control where the TV is set and the inspiratory pressure is adjusted by the ventilator to assure the preset volume delivery.
HFOV is high-frequency oscillatory ventilation with low TVs and small airway fluctuations. The goal of this mode is to decrease mean airway pressures, while avoiding stacking of breaths. The frequencies may vary between 100 and 900 breaths per minute with gas transport via nonconvective mechanisms.12 The most successful use for HFOV has been in the treatment of respiratory failure in premature infants.
PAV is proportional assist ventilation, which is an interactive ventilatory mode to improve synchrony between patient ventilatory demand and ventilator support.13 The ventilator provides dynamic inspiratory pressure assistance in linear proportion to patient inspiratory effort. For PAV to work the patient must be spontaneously breathing. If the patient tires, PAV will not provide the ventilatory support for a targeted pressure or volume.
Permissive hypercapnia is a modality of ventilation utilized to remove carbon dioxide from the blood when more conventional methods, that is, increasing the rate and decreasing TV, are unsuccessful. The manipulation of the ventilator to allow the PCO2 to rise upwards to 50–80 mm Hg or higher, while not jeopardizing arterial pH, is the goal of this therapy. This form of ventilation is another mode of lung-protective ventilation, and may be required in patients with a PaO2:FiO2 ratio below 300.
PEEP is positive end-expiratory pressure and occurs at the end of exhalation and prevents the deflation and collapse of an alveolus opened during inspiration. The primary role of PEEP is alveoli recruitment. Under normal circumstances, the alveolar and airway pressures are equal with complete lung emptying. Intrinsic PEEP occurs when lung emptying is not complete and the airway pressure rises to equal that of the elevated alveolar pressure. In this circumstance, if PEEP continues to rise, barotrauma to the lungs can lead to a pneumothorax.
Independent lung ventilation is a form of ventilation that commonly uses a dual lumen ET tube to allow individual lung ventilation. This may also be accomplished using two small ET tubes, one ending in each mainstem bronchus. This form of therapy is used during a thoracotomy or thoracoscopy, so the surgical side can be preferentially deflated and TV lowered to facilitate exposure for operation. Other indications for use in the operating room or the intensive care unit (ICU) include massive hemoptysis, pulmonary alveolar proteinosis, unilateral lung injury, single-lung transplantation, or bronchopleural fistula. A single or dual ventilator can be used and even set to different modes of ventilation for use with independent lung ventilation.
ACUTE LUNG INJURY
Mechanical ventilation is used to treat hypoxemia, acidosis, and other life-threatening conditions. Although lifesaving, it may incite ventilator-induced lung injury. This may occur by barotrauma manifesting as extra-alveolar air, volutrauma from mechanical stretch, atelectrauma from alveolar mechanical stress, and biotrauma from systemic inflammatory mediators.
A pneumothorax is extra-alveolar, intraplueral air and occurs in 4%–15% of patients mechanically ventilated over 24 hours. Patients most prone are those with asthma, chronic obstructive pulmonary disease (COPD), ALI, and the adult respiratory distress syndrome (ARDS). Due to the observation that this may be precipitated by right mainstem intubation, alveolar overdistension may play a major role in its pathogenesis.14
In 2000, the NIH-sponsored ARDS Network phase III study looked at two groups of patients with respiratory failure and divided them based on TV calculated from the predicted body weight.15–17 These variables were 6 and 12 mL/kg, respectively. In the 6 mL/kg group, the plateau pressure goal of <30 cm H2O was achieved by decreasing the TV to a minimum of 4 mL/kg predicted body weight. The study was terminated early due to the statistical superiority of diminished mortality in the low TV group and substantial decrease in ventilator free days. Parsons also found that these low TV patients had a substantial decrease in inflammatory mediators such as IL-6, 8, and 10.
PHARMACOLOGIC APPROACH TO MECHANICAL VENTILATION
Up to 71% of SICU and seriously ill patients experience considerable pain. If untreated pain can lead to increases in sympathomimetics, catecholamines, and cytokines.
Elevated cytokines such as TNF-alpha, IL-1, IL-6, IL-8, as well as a decrease in IL-2, can adversely affect the T cell mediated immune response. The hyperglycemia that pain and stress induce may decrease chemotaxis and phagocytosis by neutrophils, leading to an increase in the infection rate, specifically ventilator-associated pneumonias (VAPs). Increased fibrinogen concentrations, increased plasminogen activator inhibitor, and increased platelet reactivity from stress can lead to a hypercoagulable state and thrombosis. In addition, stress increases myocardial oxygen consumption, placing more stress on the heart. Thus, control of pain is important in controlling and weaning patients from mechanical ventilation. Attenuation or removal of painful and noxious stimuli is a crucial goal in oxygenation, ventilation, and weaning of these patients. Simple maneuvers such as proper positioning, using an appropriate type of bed, stabilization of fractures, and removing any physical irritants can also help decrease pain medication requirements.
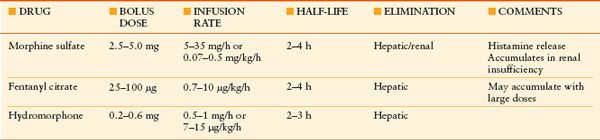
Pharmacologic adjuncts are helpful, and include opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and neural blockade. Opioids are the most common medications used for analgesia in the SICU (Table 49.3). They act centrally and peripherally via both mu and kappa receptors. Administration occurs by many avenues and includes oral, patch-transdermal, sublingual, epidural, intramuscular, or intravenous such as with a patient controlled analgesia device. There are a number of potential side effects of opioid use, the most important of which include respiratory depression, hypotension, altered mental status, constipation, and urinary retention. Naloxone is a narcotic antagonist that assists in reversal of unwanted opioid side effects.
TABLE 49.3
COMMONLY USED OPIOIDS IN THE ICU
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


