Lumbar Plexus Block
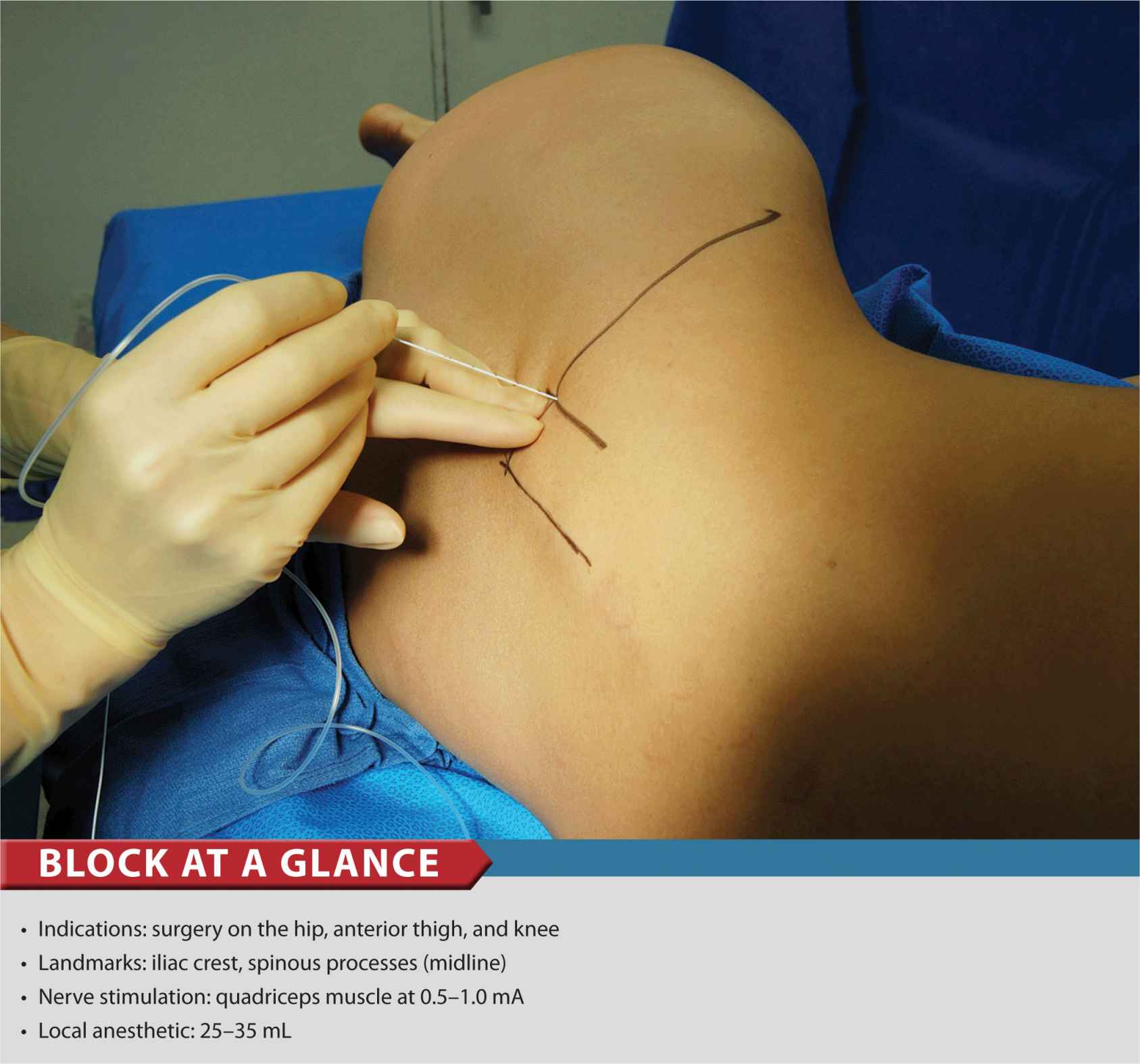
FIGURE 18-1. To accomplish the lumbar plexus block, a needle is inserted perpendicular to the skin plane, 4 cm lateral to the midline at the level of L3-L5.
General Considerations
The lumbar plexus block (psoas compartment block) is an advanced nerve block technique. Because the placement of the needle is in the deep muscles, the potential for systemic toxicity is greater than it is with more superficial techniques. The proximity of the lumbar nerve roots to the epidural space also carries a risk of epidural spread of the local anesthetic. For these reasons, care should be taken when selecting the type, volume, and concentration of local anesthetic, particularly in elderly, frail, or obese patients. The lumbar plexus block provides anesthesia or analgesia to the entire distribution of the lumbar plexus, including the anterolateral and medial thigh, the knee, and the saphenous nerve below the knee. When combined with a sciatic nerve block, anesthesia of the entire leg can be achieved. Because of the complexity of the technique, potential for complications, and existence of simpler alternatives (e.g. fascia iliaca or femoral blocks), the benefits of lumbar plexus block should always be weighed against the risks.
Functional Anatomy
The lumbar plexus is composed of five to six peripheral nerves that have their origins in the spinal roots of L1 to L4, with a contribution from T12 (Figures 18-2 and 18-3). After the roots emerge from the intervertebral foramina, they divide into anterior and posterior branches. The small posterior branches supply innervation to the skin of the lower back and paravertebral muscles. The anterior branches form the lumbar plexus within the substance of the psoas muscle and emerge from the muscle as individual nerves in the pelvis.
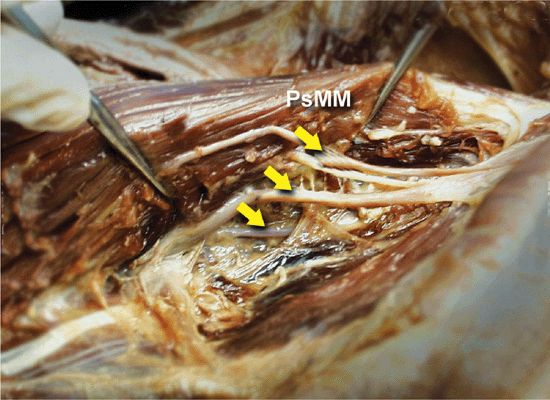
FIGURE 18-2. Anatomy of the lumbar plexus. Roots of the lumbar plexus (arrows) are seen within the substance of the psoas major muscle (PsMM); the lumbar plexus is exposed through the abdominal cavity.
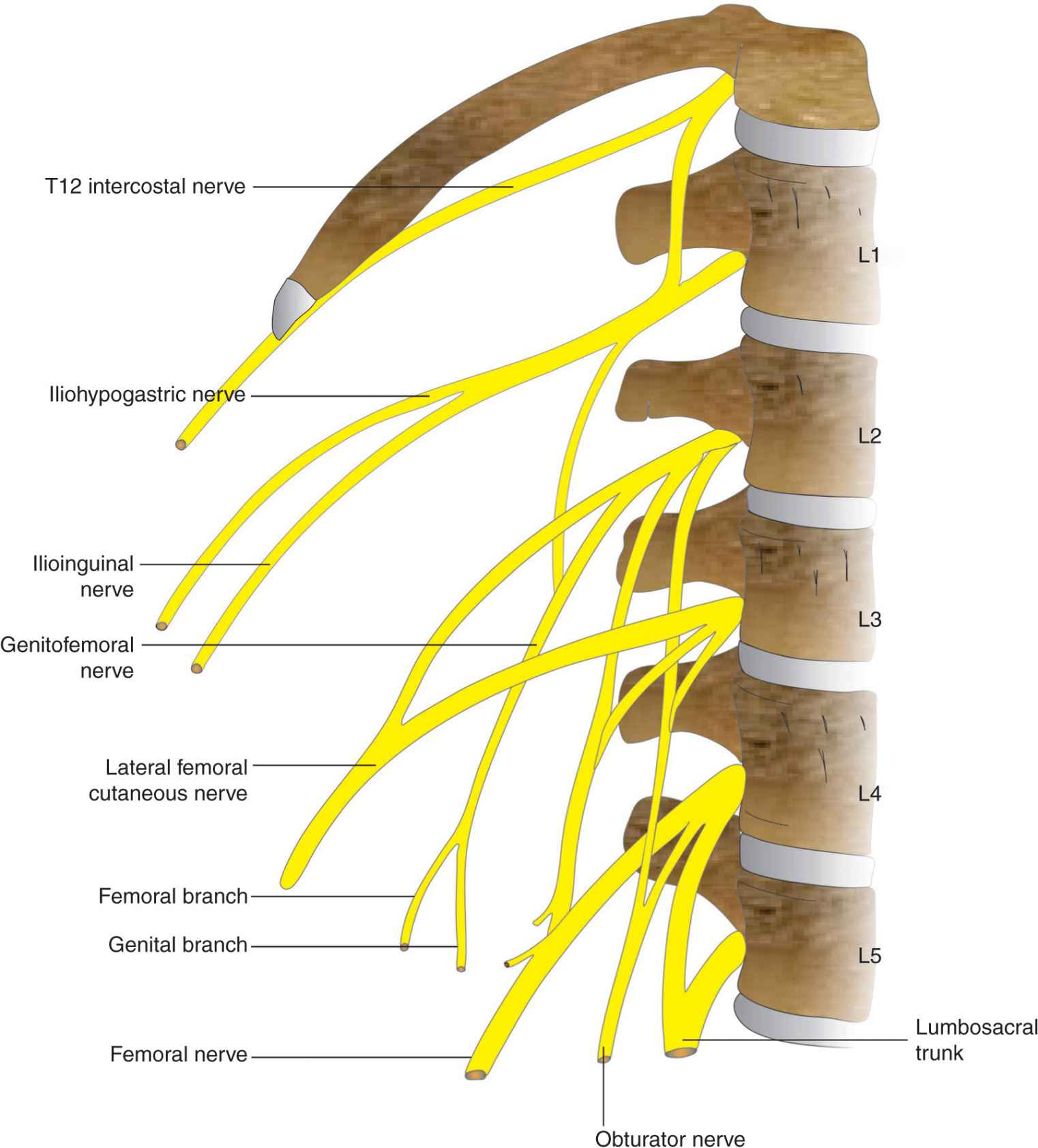
FIGURE 18-3. Organization of the Lumbar Plexus into peripheral nerves.
The major branches of the lumbar plexus are the iliohypogastric (L1), ilioinguinal (L1), genitofemoral nerve (L1/L2), lateral femoral cutaneous nerve (L2/L3), and the femoral and obturator nerves (L2,3,4). Although not a lumbar nerve root, the T12 spinal nerve contributes to the iliohypogastric nerve in about 50% of cases.
Distribution of Blockade
The femoral nerve supplies the quadriceps muscle (knee extension), the skin of the anteromedial thigh, and the medial aspect of the leg below the knee and foot (Figure 18-4 A and B). The obturator nerve sends motor branches to the adductors of the hip and a variable cutaneous area over the medial thigh or knee joint. The lateral femoral cutaneous, iliohypogastric, ilioinguinal, and genitofemoral nerves are superficial sensory nerves.

FIGURE 18-4. (A) Cutaneous distribution of the lumbar plexus to the lower extremity. (B) Motor innervation of the lumbar plexus to the lower extremity.
Single-Injection Lumbar Plexus Block
Equipment
A standard regional anesthesia tray is prepared with the following equipment:
• Sterile towels and gauze packs
• Two 20-mL syringes with local anesthetic
• A 10-mL syringe plus a 25-gauge needle with local anesthetic for skin infiltration
• A 10-cm, 21-gauge short-bevel insulated stimulating needle
• Peripheral nerve stimulator
• Sterile gloves; marking pen
Landmarks and Patient Positioning
The patient is in the lateral decubitus position with a slight forward tilt (Figure 18-5). The foot on the side to be blocked should be positioned over the dependent leg so that twitches of the quadriceps muscle and patella can be seen easily. The operator should assume a position from which these responses are visible. Palpation of the anterior thigh can be useful to make sure the motor response is indeed that of the quadriceps muscles.

FIGURE 18-5. Patient position for the lumbar plexus block.
The anatomical landmarks are as follows (Figure 18-6):
FIGURE 18-6. Landmarks for the lumbar plexus block. The needle insertion site is labeled 3-4 cm lateral to the intersection of the (horizontal) line passing through spinous processes and iliac crest (perpendicular) line.
1. Iliac crests (intercristal line)
2. Spinous processes (midline)
3. A point 3–4 cm lateral to the intersection of landmarks 1 and 2 (needle insertion point)
Maneuvers to Facilitate Landmark Identification
The identification of the iliac crest can be facilitated by the following maneuvers:
• Placing the palpating hand over the ridge of the pelvic bone and pressing firmly against it (Figure 18-7).

FIGURE 18-7. Technique of palpation of the iliac crest.
• To better estimate the location of the iliac crest, the thickness of the adipose tissue over the iliac crest should be considered.
• Pelvic proportions greatly vary among people; thus a visual “reality check” is always performed. If the estimated iliac crest line appears to be almost at the level of the midtorso or touching the rib cage (too cranial), make an appropriate adjustment to avoid insertion of the needle too cranially.
Technique
After disinfecting with an antiseptic solution, the skin and paravertebral muscles are anesthetized by infiltrating local anesthetic subcutaneously at site of needle insertion.
The fingers of the palpating hand are firmly pressed against the paravertebral muscles to stabilize the landmark and decrease the skin–nerve distance (Figure 18-8). The palpating hand should not be moved during the entire block procedure so that precise redirections of the angle of needle insertion can be made, if necessary. The needle is inserted at an angle perpendicular to the skin with the nerve stimulator set initially to deliver a current of 1.5 mA (1.5 mA, 2 Hz, 0.1–0.3 ms). As the needle is advanced, local twitches of the paravertebral muscles are obtained first at a depth of a few centimeters. The needle is advanced further, until twitches of the quadriceps muscle are obtained (usually at a depth of 6–8 cm). After these twitches are observed, the current should be lowered to produce stimulation between 0.5 and 1.0 mA. Motor response should not be present at a current less than 0.5 mA, which could indicate needle placement in the dural sleeve. At this point, 25 to 35 mL of local anesthetic is injected slowly while avoiding resistance to injection and with frequent aspirations to rule out inadvertent intravascular needle placement. A resultant, typical spread of the local anesthetic solution is demonstrated in Figure 18-9.
FIGURE 18-8. Needle insertion for the lumbar plexus block. The needle is inserted to walkoff the transverse processes and advance the needle 1-2 cm deeper.
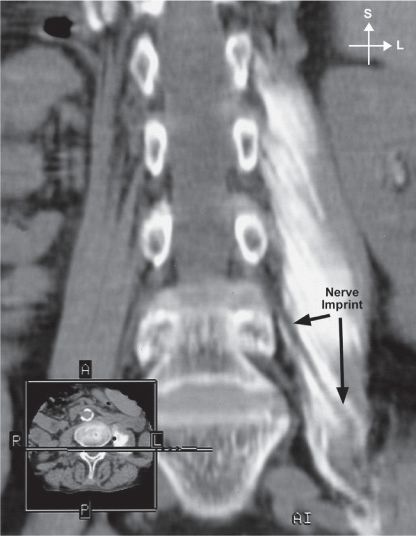
FIGURE 18-9. Radiograph demonstrating distribution of the radiopaque solution within the psoas muscle after a lumbar plexus injection.
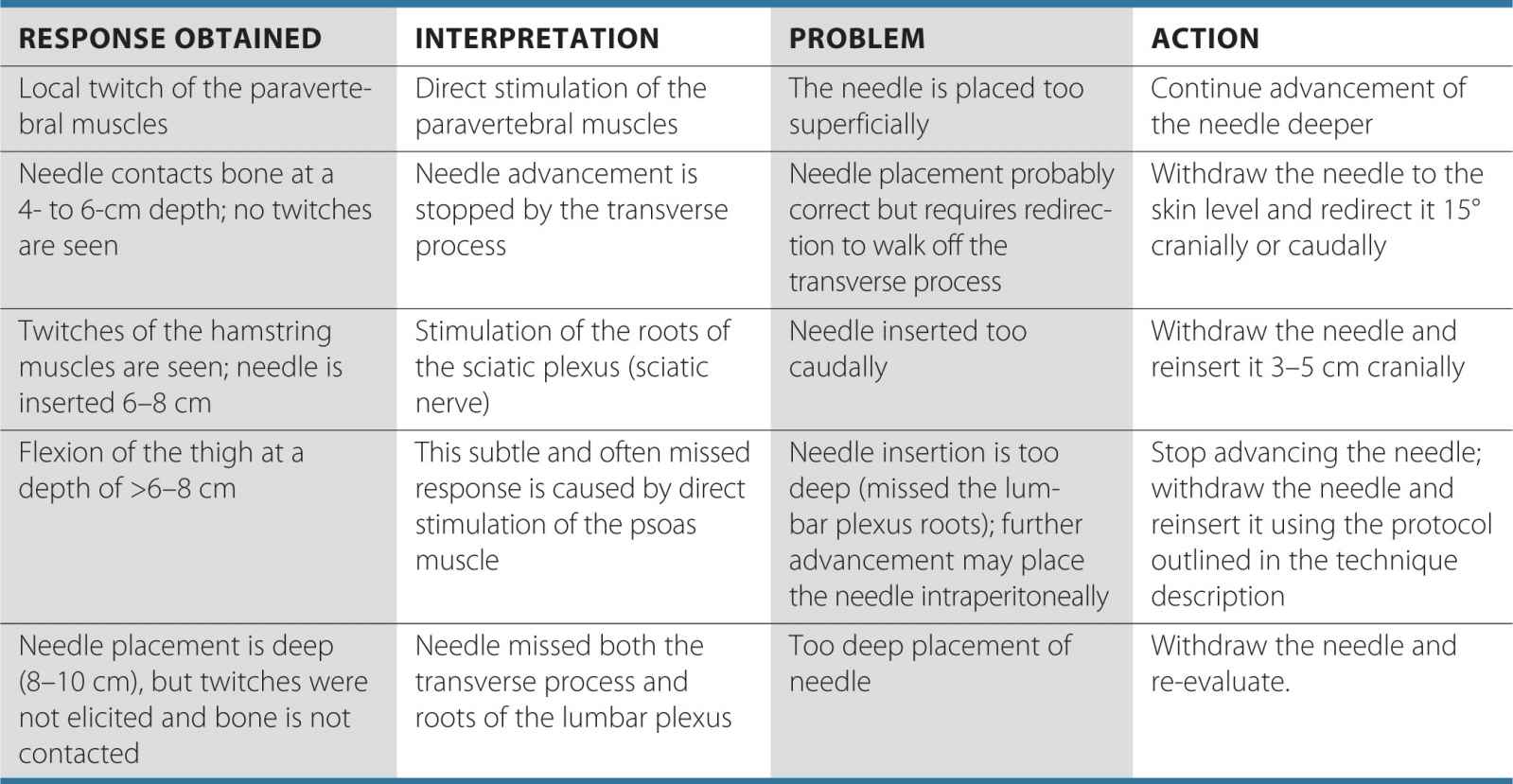
TABLE 18-1 Some Common Responses to Nerve Stimulation and Course of Action for Proper Response
Troubleshooting
When insertion of the needle does not result in quadriceps muscle stimulation, the following maneuvers should be followed:
1. Withdraw the needle to the skin level, redirect it 5° to 10° cranially, and repeat the procedure.
2. Withdraw the needle to the skin level, redirect it 5° to 10° caudally, and repeat the procedure.
3. Withdraw the needle to the skin level, redirect it 5° to 10° medially, and repeat the procedure.
4. Withdraw the needle to the skin level, reinsert it 2 cm caudally or cranially, and repeat the procedure.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


