DEFINITION
Recent clinical experience and experimental data define a rather narrow therapeutic index for local anesthetics with respect to their potential for neurotoxic injury.1 The actual risk varies based on the definition used or the threshold for detection. For example, persistent or clinically significant functional impairment remains a rare occurrence when local anesthetics are properly employed for spinal and epidural anesthesia. In contrast, minor or subtle deficits are not infrequent, and although such effects reflect alterations in neurologic function and/or architecture they are generally transient or fully reversible. Strictly speaking, anesthetic action could be considered a form of neurotoxicity. However, in common usage, neurotoxicity refers to those neurologic effects that do not derive from the reversible binding and blockade of the sodium channel, but rather extend beyond these effects. Despite such simplicity, causation is often difficult to establish, because it is frequently difficult to distinguish anesthetic neurotoxicity from other potential etiologies. In addition, adverse effects of the local anesthetics may be indirect, being mediated through mechanisms such as disturbance in nerve blood flow.2,3 To further complicate matters, other factors or adjuvants that are coadministered may potentiate toxicity. For example, there is experimental data to suggest that epinephrine can enhance the neurotoxicity of spinally administered lidocaine4 (Fig. 11-1), an effect presumably due to greater exposure to local anesthetic resulting from delayed clearance.
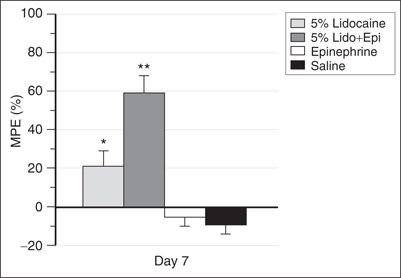
FIGURE 11-1. Sensory function 7 days after intrathecal administration of 5% lidocaine, 5% lidocaine with epinephrine (0.2 mg/mL; Lido Epi), epinephrine (0.2 mg/mL), or saline. Sensory function assessed by tail flick and expressed as percentage maximum possible effect (MPE): [(tail-flick latency – baseline)/(cutoff – baseline]) Å – 100. Data represent mean ± SD. *p <.05 versus epinephrine or saline. **p <.05 versus all other groups. (Adapted from Hashimoto K, Hampl KF, Nakamura Y, et al. Epinephrine increases the neurotoxic potential of intrathecally administered lidocaine in the rat. Anesthesiology 2001;94:876–881, with permission.)
Abundant experimental animal data support the concept that all currently used local anesthetics are capable of inducing disturbances in function and/or morphology at very low concentrations, at times below those commonly used for clinical anesthesia.5,6 Such information is critical for determining mechanisms of injury, and for developing clinical strategies for minimizing or eliminating the risk of toxicity. However, extrapolation to clinical practice is challenging, and the clinical significance of data obtained primarily from animals can be easily overstated. Thus, if one were to consider minor or transient effects and the possibility of subclinical injury as defined by experimental laboratory studies, anesthetic neurotoxicity might be a relatively common occurrence. However, this chapter is narrowly restricted to the rare significant clinical deficits for which there is clear evidence supporting local anesthetic neurotoxicity as the mechanism of injury. As such, it does not consider transient neurologic symptoms (TNS) because of the uncertain relationship of TNS to neural injury (Chapter 13). Although the primary emphasis is overt clinical injury, experimental work is reviewed as necessary to provide an appreciation of mechanisms of injury and the factors that may promote or attenuate damage.
 SCOPE
SCOPE
Since the introduction of local anesthetics into clinical practice, sporadic reports of neurologic injury associated with spinal and epidural anesthesia have periodically raised concern that local anesthetics are potentially neurotoxic. These concerns first coalesced with a report in 1937 by Ferguson and Watkins of 14 cases of cauda equina syndrome associated with the use of “heavy” Durocaine, an anesthetic formulation containing 10% procaine, 15% ethanol, glycerin, and gum acacia or gliadin.7 Although experimental studies in cats demonstrated that 10% procaine alone could induce similar injury, the nature of the vehicle components distracted focus from the local anesthetic.
Concern for anesthetic neurotoxicity was again heightened in the early 1980s by reports of injury associated with apparent unintentional intrathecal injection of doses of 2-chloroprocaine (Nesacaine-CE) intended for the epidural space.8 However, similar to the injuries associated with Durocaine, questions concerning the toxicity of one of the components of the Nesacaine-CE solution (the antioxidant sodium bisulfite) created uncertainty regarding the actual toxicity of the local anesthetic.9 Although the experimental data were somewhat conflicted,10 most concluded that 2-chloroprocaine was not neurotoxic (or at least no more so than other local anesthetics).
Although the issue of 2-chloroprocaine neurotoxicity was never actually settled, concern for local anesthetic neurotoxicity again subsided, only to reemerge a decade later with reports of injuries associated with continuous spinal anesthesia (CSA).11 The initial report contained four cases: three involved the administration of 5% lidocaine with 7.5% dextrose that was administered through a small-bore (28-gauge) microcatheter specifically marketed for CSA. The other case occurred with 0.5% tetracaine with 5% glucose administered though a standard epidural catheter intentionally positioned within the subarachnoid space for CSA.11 Despite differences in technique, all four cases shared certain elements critical to the development of neurotoxicity: administration of anesthetic produced a restricted sacral block; repetitive doses of local anesthetic were required to achieve adequate surgical anesthesia; and a cumulative dose exceeding that normally used with a single-injection spinal technique. It was suggested that the combination of maldistribution and the high dose of anesthetic led to neurotoxic anesthetic concentrations in a restricted area of the subarachnoid space, a mechanism that gained support from subsequent in vitro and in vivo experimental studies12,13 (Box 11-1). Within a year, eight additional cases were reported,14 all consistent with this etiology.
BOX 11-1 Continuous Spinal Anthesia: Guidelines for Anesthetic Administration
 Insert catheter just far enough to confirm and maintain placement.
Insert catheter just far enough to confirm and maintain placement.
 Use the lowest effective anesthetic concentration.
Use the lowest effective anesthetic concentration.
 Place a limit on the amount of local anesthetic to be used.
Place a limit on the amount of local anesthetic to be used.
 Administer a subarachnoid test dose and assess the extent of block.
Administer a subarachnoid test dose and assess the extent of block.
 If maldistribution is suspected, use maneuvers to increase the spread of local anesthetic (e.g., change the patient’s position, alter the lumbosacral curvature, switch to a solution with a different baricity).
If maldistribution is suspected, use maneuvers to increase the spread of local anesthetic (e.g., change the patient’s position, alter the lumbosacral curvature, switch to a solution with a different baricity).
 If well-distributed sensory anesthetic is not achieved before the dose limits is reached, abandon the technique.
If well-distributed sensory anesthetic is not achieved before the dose limits is reached, abandon the technique.
Adapted from Riger ML, Drasner K, Krejcie TC, et al. Cauda equina syndrome after continuous spinal anesthesia. Anesth Analg 1991;72 275–281, with permission.)
The occurrence of these cases led the Food and Drug Administration (FDA) to withdraw approval for microcatheters (defined as 27-gauge and smaller) and to issue a bulletin to all health care providers to alert them to “a serious hazard associated with CSA.”14 However, this action did not eliminate risk, as practitioners remained at liberty to use large-bore (epidural) catheters for CSA, a practice that remains particularly common following unintentional dural puncture during attempted epidural placement. Moreover, small-bore catheters may be reintroduced into clinical practice in the near future.15 Avoidance of injury therefore requires an understanding of the factors that contribute to neurotoxicity and appropriate clinical management (Box 11-1).
The factors that can lead to neurotoxic injury with CSA are not unique to this technique, but are also present with single-injection spinal anesthesia. Specifically, maldistribution can and does occur with single-injection spinals. In fact, maldistribution is likely the most common cause of a “failed spinal.” In this case, as with CSA, repeat injection following such failure may confer risk because the second injection may produce a similar restricted distribution (albeit less than with a catheter in fixed position). Here again, the combination of maldistribution and the relatively high anesthetic dose has the potential to achieve neurotoxic concentrations of anesthetic within the subarachnoid space. A 1991 review of the closed claims database, and subsequent case reports, provide compelling support for this mechanism of injury.16
There is a third mechanism by which relatively high doses of anesthetic may be administered intrathecally during routine anesthetic practice. While attempting an epidural anesthetic, a practitioner may fail to appreciate that the needle or catheter has been unintentionally positioned in the subarachnoid space and administer an “epidural dose” that far exceeds that appropriate for spinal block. Although the excessive spread of spinal anesthesia and the hemodynamic and respiratory consequences have often been the focus of attention, these complications can be readily managed without long-term sequelae. In contrast, the effects of local tissue toxicity are likely to be permanent. As previously noted, concern for neurotoxicity under these clinical circumstances initially surfaced in the early 1980s with reports of injuries associated with 2-chloroprocaine.8 Beginning in 1992, similar cases have been reported with lidocaine,17 an anesthetic once considered the “gold standard” for safety.
The reports of injury with CSA, repetitive injection after a failed spinal, and intrathecal injection of an “epidural dose” of anesthetic served to establish the significant risk of toxicity with doses of intrathecal anesthetic exceeding those commonly used for single-injection spinal anesthesia. Far more surprising, and of greater concern, two subsequent reports raised suspicion that injury can occur with lidocaine administered within the dose range generally recommended for single-injection spinal anesthesia. One described a case in which cauda equina syndrome followed otherwise uncomplicated administration of 100 mg of hyperbaric lidocaine with epinephrine.18 The second report contained data from a prospective study of regional anesthesia in France.19 In this database, which contained roughly 10,000 single-injection lidocaine spinals, there were eight persistent deficits that could not be explained on any basis other than neurotoxicity. All of these injuries occurred with doses at the high end of the normal dosage range (≥75 mg), and the two that were permanent followed injection of the highest recommended dose (100 mg). The lack of an alternative etiology and this clustering of injury at the high end of the dose range made toxicity the most likely etiology.20
Recent reports of injury associated with lidocaine, combined with supportive experimental data, have generated interest in alternative local anesthetics for spinal anesthesia. This interest has been reinforced by the common occurrence of TNS associated with this agent (Chapter 13). Despite a rather blemished record, considerable attention is now focused on 2-chloroprocaine, and based on early systemic volunteer studies,21–23 small clinical reports,24 and fairly extensive off-label use, it would appear to hold promise, although additional clinical data are required to establish safety.25 Clinical use of 2-chloroprocaine has rested on the assumption that the neurotoxicity associated with the Nesacaine-CE formulation was due to the presence of bisulfite (at a low pH) rather than to the anesthetic per se.9 However, as mentioned previously, this etiology was never clearly established, and recent experimental data suggest that bisulfite might actually be neuroprotective26 (Chapter 8). Ironically, these data also suggest that the toxicity of 2-chloroprocaine is roughly equivalent to lidocaine on a milligram-for-milligram basis, a fact that could be used to support the use of spinal 2-chloroprocaine and to provide guidance regarding an acceptable dose range for this agent. (It should be recalled that previously reported injuries associated with 2-chloroprocaine likely involved administration of high doses intended for the epidural space.)
 PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Despite a century of clinical concern, the pathophysiology of anesthetic neurotoxicity is still poorly understood. The issue rests not in the lack of an effect that might underlie the toxicity of these compounds but with which of the many identified injurious effects of the local anesthetics play a role in clinical toxicity. Specifically, studies using cell culture6,27,28 or isolated segments of frog,5 crayfish,29 rabbit,30 or rat31 axon demonstrate myriad detrimental effects with “clinical” concentrations of local anesthetics, including conduction failure, membrane damage, enzyme inhibition, loss of membrane potential, enzyme leakage, cytoskeleton disruption, accumulation of intracellular calcium, disruption of axonal transport, growth cone collapse, neurite degeneration, and cell death. As anticipated, blockade or attenuation of some of these effects may reduce or prevent toxicity. For example, preventing the anesthetic-induced rise in intracellular calcium by preloading cultured dorsal root ganglion (DRG) neurons with the Ca buffer BAPTA can inhibit anesthetic-induced cell death.6 However, the manner in which the diverse deleterious factors interact and (specifically) in which effects are “upstream” has yet to be defined, though membrane disruption (perhaps via a detergent effect) is likely to be an early event.32 Further complicating the matter, the concentration having a specific effect in an isolated segment of axon or in cell culture must be interpreted with caution, as the relevant concentrations achieved at the neuronal or cellular level in vivo are largely speculative.
Although the underlying mechanisms of toxicity have yet to be clearly defined, in vivo studies demonstrate the potential clinical relevance of anesthetic toxicity. To this end, spinal administration of clinical concentrations of anesthetic in an intact animal can induce functional loss corresponding to clinical injury and histologic damage consistent with impairment.4,33,34 Substantial evidence suggests that these effects are due to the anesthetic per se, rather than to the presence of glucose or to high osmolarity (e.g., hyperbaric 5% lidocaine has an osmolarity of roughly 857 mOsm). Specifically, dose-dependent loss of sensory function produced by intrathecal lidocaine is unaffected by the presence of 7.5% glucose, and in contrast to 5% lidocaine, administration of 10% glucose does not induce functional impairment or morphologic damage34 (Fig. 11-2). Moreover, when applied directly to an axon in vitro, 7.5% glucose does not affect the compound action potential or potentiate conduction failure induced by lidocaine.5
FIGURE 11-2. Nerve injury score for sections obtained 7 days after an intrathecal infusion of 5% lidocaine, 10% glucose, or normal saline. Data reflect the mean ± SEM. (Adapted from Hashioto K, Sakura S, Bollen AW, et al. Comparative toxicity of glucose and lidocaine admin-istered intrathecally in the rat. Reg Anesth Pain Med 1998;23:444–450, with permission.)



