Chapter 22 Laryngeal Mask Airway
III. Laryngeal Mask Airway Insertion Technique
IV. Classic Laryngeal Mask Airway
V. Flexible Laryngeal Mask Airway
VI. Laryngeal Mask Airway Use in Patients with Difficult-to-Manage Airways
VII. ProSeal Laryngeal Mask Airway
VIII. Supreme Laryngeal Mask Airway
IX. Disposable Laryngeal Mask Airways
X. Exchange Using the Aintree Intubation Catheter
XI. Problems and Controversies
I Introduction
The laryngeal mask airway (LMA, LMA Company, Henley, England) is a supraglottic airway device developed by Archie Brain, a physician and honorary consultant anesthetist of the Royal Berkshire Hospital, Reading, England. It was introduced into clinical practice in 1988. In the first paper on the LMA,1 Brain described the device as “an alternative to either the endotracheal tube (ETT) or the face-mask with either spontaneous or positive-pressure ventilation (PPV).” Twenty years and more than 200 million safe uses later, the LMA has significantly improved the comfort and safety of airway management worldwide. Many authorities in anesthesia consider the LMA to be the most important development in airway management in the past 50 years.
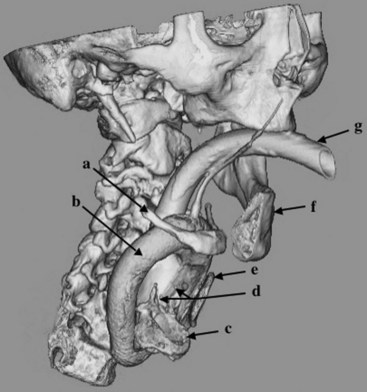
The LMA is a minimally invasive device designed for airway management in the unconscious patient. An inflatable mask is fitted with a tube that exits the mouth to permit ventilation of the lungs. The mask fits against the periglottic tissues, occupying the hypopharyngeal space and forming a seal above the glottis instead of within the trachea (Fig. 22-1). Originally produced as a single, general-purpose design in a range of sizes, it is currently made in various forms to satisfy different requirements.
The LMA is a supraglottic airway management device. A substantial body of literature, while supporting the wisdom of exercising caution when learning to use the supraglottic approach, provides ample evidence of a wide range of uses that go beyond those originally postulated.2 For example, the LMA is becoming increasingly popular outside the operating room, as evidenced by its endorsement by the European Resuscitation Council and the American Heart Association.3 Its more exotic uses include the adoption of the Fastrach ILMA, which is the intubating form of the LMA, by the National Aeronautics and Space Administration (NASA) as part of its emergency medical kit for space travel. A literature search indicates that the later varieties of the LMA, including the FLMA, ILMA,4 and PLMA,5 may be more appropriate tools for specific uses than the original LMA.
More than 2000 scientific articles have described the impact of the LMA on modern anesthesia, and a full review is beyond the scope of a single chapter. Our aim instead is to provide an overview of the LMA’s uses worldwide. After a historical review and comments regarding the correct LMA insertion technique, we explore the principal uses of each LMA model, discuss possible problems, and offer suggestions for getting the best results from each device. We describe the evolution of the LMA’s use in patients with difficult-to-manage airways and provide the current recommendations for LMA use from the American Society of Anesthesiologists (ASA) difficult airway algorithm.6
II History and Development
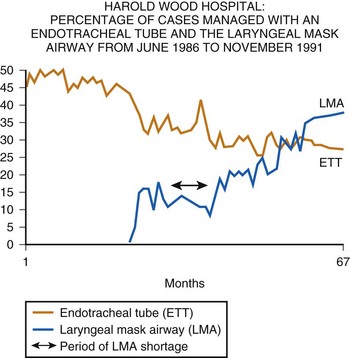
In 1988, the definitive device, now referred to as the LMA Classic, was released commercially in the United Kingdom. Although the LMA was rapidly adopted there, it was not until 1991 that the U.S. Food and Drug Administration permitted release of the device in the United States and then only with the stricture that “the LMA is not a replacement for the endotracheal tube.” Because the LMA was at that time a very unconventional way of managing the airway, this caution was understandable. Nevertheless, it resulted in a somewhat slower acceptance of the concept of “masking the larynx” in the United States than in the United Kingdom, where the LMA was purchased by every health authority within 2 years of its launch, resulting almost immediately in a reduction in ETT use (Fig. 22-2).
A From Idea to First Prototype
Brain is often asked how the idea of the LMA first arose. Like many before him, he thought that a supraglottic approach would be less traumatic than intubation and therefore more desirable, provided the method could be easier to control and more reliable than the face mask. Other inventors had mainly explored the oral and pharyngeal spaces above the larynx,7–12 but the LMA was the first device to encircle the periglottic tissues in the hypopharynx with a mask. The idea was conceived in early 1981, and later that year, Brain began providing dental anesthesia at the outpatient clinic of the Royal London Hospital. At that time, a device known as the Goldman dental nose piece was being used for airway maintenance during dental extractions in anesthetized patients. It was a reusable, vulcanized rubber mask that could be detached from its rigid base for cleaning (Fig. 22-3). The mask was designed to fit over the nose, leaving the mouth free for surgical access. Noticing a certain similarity between the contours around the nose and those around the glottis, Brain wondered if the Goldman mask could be modified to fit over the larynx. Placing a device over the larynx would short-circuit the upper airway passages, perhaps eliminating some of the problems associated with maintaining their patency under anesthesia.

Because the Goldman mask was scheduled to be discontinued in favor of a disposable version, Brain was able to obtain samples for experimentation. Using an acrylic adhesive, he glued a diagonally cut, 10-mm Portex ETT to the rubber mask’s attachment flange, which he had to draw across the mask aperture into the midline to form a base (Fig. 22-4). Figure 22-5 is a 1981 photograph of the inventor as he is about to insert one of the resulting prototypes into his anesthetized pharynx to test the validity of his hypothesis. In his diary, he recorded an absence of any complications, despite having repeated the experiment four times. This observation, combined with a broadly worded institutional review board approval, provided the justification for subsequent extensive clinical investigations, which occupied him for the next 7 years. During this time, he built many prototypes, which he used in approximately 7000 patients.13 He also kept extensive notes in private diaries to record his progress but published only a small number of cases, because he believed there was little point in presenting data concerning an invention that was not ready for production.


B Early Publications
The first article about the LMA, published in the British Journal of Anaesthesia in 1983, presented data from only 23 patients and received little attention.1 A second description 2 years later in Anaesthesia was subtitled “Development and Trials of a New Type of Airway” and detailed the LMA’s use in 118 patients, although it also reported that Brain and colleagues had gained experience in more than 500 cases.14 On the basis of this experience and a case report published the previous year in Archives of Emergency Medicine,15 Brain and colleagues felt justified in concluding that “the laryngeal mask may have a valuable role to play in all types of inhalational anesthesia, while its proven value in some cases of difficult intubation indicates that it may contribute to the safety of general anesthesia.”14
In the same issue of Anaesthesia, Brain presented further evidence of the potential usefulness of the device in cases of difficult intubation, but there was still no response to these claims from the profession, perhaps because no product was available for independent assessment.16 However, he had given one of his prototypes to a visiting American anesthesiologist, Ronald Katz, a physician and chairman of the anesthesiology department at the University of California–Los Angeles. Katz provided the first independent description of the LMA based on his experience with this prototype, writing in Wellcome Trends in Anesthesiology in October 1985 and again in February 1986.17,18 The second article provided the first published image—reproduced from one of the inventor’s transparencies—of the glottis seen fiberoptically through the LMA prototype and mentioned the potential of the device to overcome intubation problems. American awareness of the LMA preceded its availability in the United States by 6 years.
C From Handmade Models to Clinical Use
There were three reasons why the LMA took so long to become clinically available: the initial lack of commercial interest, which meant there were no models available for others to use; the solitary nature of the LMA’s development, which was carried out virtually single-handedly by a clinician who continued to work with largely homemade equipment until the first commercial prototypes were made in early 1988; and the complexity of the airway anatomy, which made it hard to design a device that was safe and effective. One advantage of the long development process was that the considerable clinical history that the inventor accumulated between 1981 and 1988 guided the development of the LMA, and the first factory-made models required little modification. They were produced in Gary, Indiana; tested by Brain; and then demonstrated to colleagues at the Royal East Sussex Hospital, Hastings, United Kingdom, in April 1988. Colin Alexander, the chairman of the anesthesiology department at the Royal East Sussex Hospital, immediately authorized the LMA’s use in his department and published his experience in a letter (“Use your Brain”) in Anaesthesia that year.19 He concluded that the device “should be considered whenever the indication for tracheal intubation does not include protection of the airway from gastric contents.” Meanwhile, a few colleagues who had been given prototypes by Brain (one person built his own) continued to explore the LMA’s use in known cases of difficult intubation, with encouraging results.13
Arguably, the most influential clinical study using Brain’s hand-built prototypes was not published until 1989, after the commercial form of the device had become available. Brodrick and colleagues studied 100 cases in which the patients breathed spontaneously.20 Eighteen anesthesiologists took part in the study and recorded a “clear and unobstructed airway in 98% of cases,” but obstruction on initial placement of the LMA occurred in 10 cases and “appeared to be as a result of downfolding of the epiglottis.” A stainless steel introducer tool with a handle similar to that of the Fastrach ILMA and a blade fitting into a slot in the distal anterior end of the LMA’s mask had been designed to overcome this problem. An aperture in the blade into which the epiglottis fit caused the epiglottis to be drawn upward as the tool was removed from the patient’s pharynx. This insertion tool was used successfully in these cases, but fears that it could cause trauma led to it being abandoned in the commercial form of the LMA. Brodrick is often quoted in support of limiting the use of the LMA to spontaneously breathing patients. However, because the LMAs used by Nunn’s group were prototypes, only a size 3 device was available for use in 72 men and 28 women (weight not recorded). Given the possibility that the LMA’s size was less than optimal, it is not surprising that eight patients could not be ventilated using positive pressure without unacceptable leaks and that the mean leak pressure was 17 cm H2O, similar to that recorded by Brain 6 years earlier.13
In addition to the information accumulated in his clinical work, study of the anatomy and physiology of the larynx and pharynx guided Brain throughout development of the LMA. As the work progressed, he struggled to achieve a balance in simplicity, efficacy, and safety. In designing a device that fit into the lower pharynx, measures favoring efficacy tended to counteract those favoring simplicity. Improving the seal, for example, required more complex construction to avoid potential trauma related to high mucosal pressures. Likewise, an effort to make the device easier to insert led to the development of an insertion tool, which was determined by Brain to be potentially unsafe and therefore abandoned, despite the efficacy it demonstrated.13 Ultimately, the solutions chosen were compromises. For example, Brain realized that seals with a leak pressure much higher than 20 cm H2O were rarely necessary in practice and that an inadequate seal often could be overcome by using a more appropriately sized device, using a better fixation technique, or giving a more appropriate anesthetic. To make insertion of the LMA maximally reliable and minimally traumatic, a technique gradually evolved that was based on the swallowing mechanism. Unfortunately, he underestimated the difficulty of teaching others to master such a subtle technique, which is virtually impossible to learn without direct, hands-on demonstration and guidance.21 As a result, many articles in the LMA literature suggest variant insertion methods, most of which had already been tried and rejected by Brain for being unreliable or traumatic.
Despite these difficulties, the history of the LMA since its first commercial launch is essentially a story of steady expansion in use around the world. Availability, cost, and user education have governed the speed at which the various forms of the LMA have been accepted. Figure 22-2 demonstrates data collected by the anesthesiology department of Harold Wood Hospital, a typical general hospital near London, on the influence of the LMA Classic in the first 3 years of its availability and on the use of the ETT and the face mask. The dip in the curve representing LMA use indicates a period when it was commercially unavailable. These data show that use of the ETT almost immediately declined in favor of the new method of airway management, and they illustrate the rapid growth of LMA use in the United Kingdom. They also cast some doubt on the widely held view that the popularity of the LMA in the United Kingdom has been due to the more frequent use of the face mask there than in the United States.
III Laryngeal Mask Airway Insertion Technique
Investigations using magnetic resonance imaging (MRI) to assess the effect of the LMA on the anatomy of the airway may help to explain the reliability of the device. A study by Shorten and coworkers of 46 adults requiring sagittal MRI views of the head and neck compared the anatomic differences in awake, sedated, and anesthetized patients.22 With an LMA in place, the epiglottic angle was more than twice as great with respect to the posterior pharyngeal wall in the anesthetized group as it was in the sedated or awake group. This had no apparent effect on ventilatory function in most patients, probably due to the depth of the LMA bowl, which the inventor found to be a critical dimension when experimenting with different design ideas during the 1980s. The recommended standard insertion technique evolved slowly as Brain gained experience, and it was not until he had been inserting LMAs for almost 10 years that he realized that his technique was becoming more and more similar to the physiologic act of swallowing food. When he realized this, it was a simple matter to study this mechanism more closely and make allowances for the fact that in the anesthetized patient, this reflex is partially or completely abolished. The following key points emerged:
1. Correct mask deflation is important. The purpose of chewing food is to form a soft, atraumatic paste that can easily be passed through the pharynx and esophagus. At the onset of swallowing, this paste (i.e., food bolus) is pressed by the tongue into the hard palate. The pressure generated is distributed widely over the palatal surface, so there is no localized high-pressure point, which would give the sensation of a sharp object and lead to rejection instead of swallowing. Brain realized that to imitate the sensation of a soft food bolus, he needed to deflate the mask so that it presented an elastic, hollow shape. When this shape was pressed into the dome of the palate, the hollow form would need to be inverted. The pressure required by inserting the finger to achieve this would cause the outer rim of the mask to act like a gentle spring, producing the desired effect of spreading pressure smoothly over the entire posterior surface of the mask. This spring effect cannot be achieved without deflating the mask to a vacuum pressure of about −40 cm H2O. Only in this way was it possible to prevent the pointed distal end of the mask bowl from transmitting an irritating localized pressure point as it was pressed into the oropharyngeal curve. Partial mask inflation could not achieve this aim, however, because the soft distal end of the mask rolled backward, allowing the pointed tip of the mask bowl to scratch the palatal surface. Deflating the mask such that it followed the curvature of the palate had the same disadvantage, because it made the pointed end even more prominent. Inserting a fully inflated mask introduced excessive bulk, which created the possibility of tearing the cuff against the teeth and was physiologically equivalent to swallowing too large a bolus of food, which could lead to the rejection reflex.
2. The deflated mask must be lubricated if the oral cavity is not already wet. There is a parallel with swallowing because lubrication is a key part of deglutition. Because the mask is slid against the palate, it makes sense to apply a bolus of lubricant to the distal hollowed posterior surface of the mask immediately before insertion. Water-soluble jelly is a good substitute for oral secretions. It is not necessary or desirable to spread the lubricant over the whole surface of the mask before insertion.
3. Flatten the mask against the hard palate. Initially during swallowing, the tongue flattens the softened food bolus against the hard palate; during the first step in LMA insertion, the mask, correctly prepared to impart a sensation similar to that of a soft food bolus, is flattened by pressing it against the hard palate. Placing the index finger on the airway tube at its junction with the mask under the deflated proximal rim of the cuff is the best way to impart the necessary force.
4. Cranioposterior movement of the index finger. In swallowing, the bolus of food is advanced into the pharynx, esophagus, and stomach through precise coordination of several muscle groups, beginning with the tongue. During LMA insertion, the clinician must use her or his index finger to advance the mask in the cranioposterior direction, imitating the action of the tongue. This allows a completely deflated tip to slide smoothly along the hard palate, soft palate, and posterior pharyngeal wall while minimizing the contact of the mask with anterior structures such as the base of the tongue, epiglottis, and laryngeal inlet. The finger must continue to push in a cranioposterior direction even though the anatomy forces the mask and the finger to move caudally. The finger must never consciously be directed caudally and should be inserted to its fullest extent until resistance is felt as the mask tip enters the upper esophageal sphincter (UES). It is anatomically impossible to perform this action correctly without extending the proximal metacarpophalangeal joint of the index finger and flexing the wrist.
5. Widening the oropharyngeal angle is the first role of the nondominant hand. Cadaveric work demonstrates that if the head of the supine subject is pushed by the supinated hand in a caudal direction, head extension, neck flexion, and mouth opening are simultaneously achieved. This maneuver widens the oropharyngeal angle to greater than 90 degrees in the normal subject and draws the larynx away from the posterior pharyngeal wall. Both effects facilitate LMA insertion. The nondominant hand should therefore maintain firm caudal pressure on the occiput from the start of insertion until the mask has passed behind the tongue.
6. Removal of the index finger is the second role of the nondominant hand. To prevent the mask sliding out of position after it is fully inserted, the nondominant hand should move from behind the head to grasp the proximal end of the LMA before the index finger is removed. As the index finger is removed, the mask is held steady, or if it has not been fully inserted, it can be pressed further into position by the nondominant hand.
7. The mask is inflated. As the mask is inflated, its increased bulk and the relatively large radius of the airway tube cause it to slide cranially. It can be shown anatomically that this results in loss of contact between the mask tip and the UES. However, the LMA should not be held in place during inflation because this can result in the distal end of the mask stretching the UES. All LMAs should be inflated to a pressure of less than 60 cm H2O; pressures above this have been found to cause discomfort in awake volunteers.
8. Device fixation restores stability of the seal against the UES. The distal end of the tube is again pressed into the curve of the hard palate to reestablish firm contact between the proximal end of the device and the UES. While this pressure is maintained, adhesive tape is applied to the maxilla on one side of the patient’s face and passed over and under the tube in a single loop before fixing to the opposite maxilla. This form of fixation ensures stability of the device and is likely to afford maximum protection in the event of unexpected regurgitation, and it reduces the incidence of gastric insufflation during PPV.*
The basic insertion technique is identical for all LMA models. Unfortunately, misunderstanding of and a lack of commitment to mastering this technique are widespread, as reflected in the multiplicity of insertion methods advocated in the literature and the common belief that a failure rate of 10% is acceptable. When variant insertion techniques are used, the failure rate is about fivefold higher than it is with the standard insertion technique. The risk of complications, such as laryngeal or pharyngeal trauma and pulmonary aspiration, probably increases even more than the failure rate when the standard insertion technique is not used. The use of variant insertion techniques also may hinder or prevent the user from acquiring the skills necessary for advanced clinical applications of the LMA. As shown in several reports, use of the standard insertion technique results in a reliable airway, a minimal stress response, and an extremely low risk of complications, probably because the LMA’s position in relation to the respiratory and alimentary tracts is optimal when the standard insertion technique is used. The manuals for the LMA Classic, the FLMA, the Fastrach ILMA, and the PLMA offer step-by-step instructions on the recommended insertion technique.23
IV Classic Laryngeal Mask Airway
A Basic Uses
1 Indications for Use
Indications for LMA use have evolved since its invention. Although it has long been accepted that success rates for establishing an airway with the LMA tend to be high, even in relatively unskilled hands, it is equally clear that there is more to the art of using the LMA than getting it into place. Indications have steadily expanded as the device’s popularity has spread. Just as complications tend to diminish with increasing user experience, so the more confident and more adept user seems to find applications for the LMA that might previously have seemed inappropriate. Using the LMA for airway maintenance during atrial septal defect repair in children, for example, would no doubt strike many American anesthesiologists as highly unconventional, just as it would have alarmed the inventor had it been suggested he try this in 1988.24
2 Inherent Teaching Difficulties: A Vicious Circle
The learning curve for correct LMA insertion extends beyond the often cited 10 to 15 uses by one or two orders of magnitude.25 For the anesthesiologist who is just starting to get used to the LMA, an important advantage of confining its use to simple cases is that they represent the greater part of the surgical caseload in many locations, and there are many opportunities for learning and practice. Most anesthesiology residents, however, start out in a teaching hospital, where the caseload tends to be weighted more heavily toward long and complex procedures for which LMA use would be inappropriate in any but the most experienced hands. For this reason, it is common to hear experienced U.K. and U.S. consultant anesthesiologists complain that newly appointed colleagues, who have spent the greater part of their training years in teaching hospitals, appear to have only the most rudimentary concept of LMA use. It is, unfortunately, the same academic colleagues who carry out many of the studies that make up the core of evidence-based knowledge for the LMA. This represents a vicious circle that is not easy to break, particularly at a time when there is increasing pressure on the medical profession to justify all clinical activity by reference to proven techniques. A suggested way out of this impasse is outlined subsequently.
3 Graduating from Simple to Specialized Uses of the Laryngeal Mask Airway
The safety of the patient must be the guiding principle when deciding whether someone is qualified to perform specialized uses of the LMA. A clinician whose first-time insertion success rate is 90% or less should not be considered adequately trained to progress beyond the simplest procedures in ASA I patients. Davies and colleagues reported a success rate of 94% in the first 10 cases in which naval medical trainees used the LMA for the first time in ASA I anesthetized patients.26 The insertion success rate depends on the types of cases routinely encountered, and the preceding generalization applies to clinicians in an average peripheral hospital that performs a broad range of common procedures.
B Specialized Uses
1 Procedures Outside the Operating Room
a Radiology and Magnetic Resonance Imaging
The potential advantages of the LMA in investigative imaging were first described in a letter to Anaesthesia from Glasgow, Scotland, in 1990.27 The investigators pointed out that the LMA permitted hands-free control of the airway in patients who needed to be kept immobile for prolonged periods, a situation often necessitating general anesthesia in restless or young patients. To improve its performance and durability, the LMA’s valve later was fitted with a small, stainless steel spring, which unfortunately interfered with MRI of the head and neck. However, LMAs equipped with valves made of nonferrous material were subsequently made available for use in this situation. Stevens and Burden, in a letter to Anaesthesia in 1994, commented that they had used the LMA Classic with the modified, nonmetallic valve in more than 500 small children undergoing MRI and that it had proved safe and reliable.28 They also presented an MRI image demonstrating that the FLMA could not be used for investigations involving the head and neck because the tube contained a wire, which obliterated the image of the surrounding area.
Goudsouzian and associates were the first Americans to report the efficacy of the LMA during MRI, using the images obtained during investigations in 28 children to comment on the position of the device when inserted by residents in training.29 Despite poor user skills (21% of attempts resulted in a failure to insert, 21% of the cases required more than one insertion attempt, 82% had a downward deflection of the epiglottis, and 7% had oropharyngeal misplacement), satisfactory ventilatory parameters were maintained in all of the children. The safety of the LMA, even in less than fully skilled hands, is a powerful argument for its use in areas remote from the operating room. Van Obbergh and colleagues, working in Brussels, Belgium, presented results from somewhat more experienced users.30 The LMA was used during MRI in 100 consecutive procedures in children that were carried out using propofol. The position of the LMA was not recorded, but only 16% of the cases required more than one insertion attempt, there were no failures to insert, and oxygen saturation values of 99.1% or above were maintained in all of the children. Ventilation was manually assisted using an Ayre T-piece.
b Radiation Therapy
Grebenik and coworkers were the first to describe the use of the LMA in pediatric radiation therapy in their study of 25 children who underwent a total of 312 courses of radiation therapy under anesthesia.31 The children were between 3 weeks and 3 years old, and eight of them were anesthetized once daily for 20 or more consecutive days. In each case, the LMA was left in place until the protective reflexes returned. The absence of complications suggests that the LMA may be appropriate for procedures requiring frequent, repeated use of anesthetics in children.
A major advantage of the LMA over the ETT in children receiving radiation therapy on a daily basis during a 4- to 6-week course of treatment is that the LMA does not invade the trachea. The risk of tracheal ulcerations, granulation tissue, and subsequent tracheal stenosis associated with repeated intubations with an ETT is eliminated. The LMA causes much less stimulation than does an ETT; anesthesia requirements for the LMA are significantly lower. For example, at the University of Texas M.D. Anderson Cancer Center in Houston, all children undergoing radiation therapy receive an intravenous infusion of propofol as the sole anesthetic agent during their treatment. The LMA is frequently used for airway management, and spontaneous respiration is preserved (Fig. 22-6). This allows more rapid turnover of patients and more efficient use of the radiation therapy suite.

c Diagnostic and Short Therapeutic Procedures in Children
The LMA can be very useful during short diagnostic, therapeutic, and minor surgical procedures performed in children in the hospital’s procedure room or in the operating room. These procedures include spinal puncture with or without intrathecal therapy, bone marrow aspirations, insertion or removal of a central line or a Port-a-Cath, and minor biopsies (Fig. 22-7). Most children tolerate these procedures well under deep intravenous sedation with propofol and local anesthesia with maintenance of spontaneous respiration. However, some children develop respiratory depression or airway obstruction during deep sedation. In those children, the LMA can be an excellent and much less invasive alternative to endotracheal intubation, resulting in a clear airway without resorting to general anesthesia and muscle relaxation.

d Cardiology
The LMA can be useful in patients undergoing transesophageal echocardiography (TEE). TEE is an invasive procedure, and many patients experience significant discomfort or are unable to tolerate TEE under topical anesthesia. In the cardiology clinic setting, TEE is usually performed with topical anesthesia consisting of spraying the oropharynx with a local anesthetic (e.g., 4% lidocaine or 20% benzocaine), with or without sedation.32,33 However, a significant number of patients experience discomfort during the procedure, and many cannot tolerate the insertion of the probe, even after sedation.34,35 Because topical anesthesia and light sedation do not completely abolish the gag reflex, deep sedation or general anesthesia may be necessary for patients with highly sensitive reflexes in the upper airway and pharynx. A possible solution for patients who cannot tolerate the insertion of the TEE probe with topical anesthesia and light sedation is deep sedation with propofol. The LMA can be used to maintain the airway in patients undergoing TEE examination during deep sedation with propofol.36 The LMA can easily be inserted with the TEE probe in place, and the presence of the LMA does not interfere with the manipulation of the probe (Fig. 22-8).
The LMA can be a better alternative than endotracheal intubation in patients undergoing cardioversion in whom face mask ventilation is difficult or inadequate. The minimal hemodynamic stimulation associated with insertion of the LMA, which contrasts with a significant hemodynamic response during endotracheal intubation, offers a great advantage in patients with cardiovascular disease.37
2 Head and Neck Surgery
Most of the applications of the LMA in procedures involving the head and neck are done with the FLMA. However, a unique advantage of using the LMA Classic in these patients is the access to the larynx that the device allows (Fig. 22-9), which is particularly useful for diagnostic evaluation of the larynx and trachea and during neodymium:yttrium-aluminum-garnet (Nd:YAG) laser surgery. It is difficult to manage the airway using an ETT in patients who require Nd:YAG laser treatment of lesions located in the vocal cords or the proximal part of the trachea because the ETT limits access to these lesions. There also is a high risk of a laser-induced airway fire when an ETT is used. In contrast, the LMA provides an unobstructed view of the surgical field and virtually eliminates the risk of airway fire (Fig. 22-10).


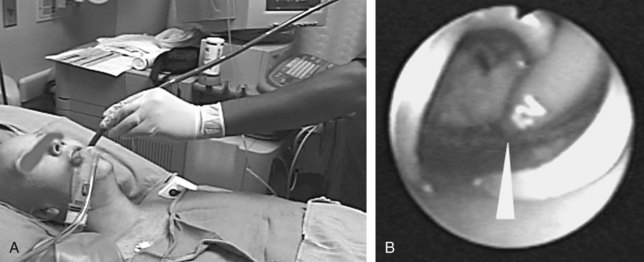
Head and neck surgery is associated with the risk of bruising or otherwise traumatizing nerves that control the motor functions of the larynx. The LMA can be useful in evaluating the function of the vocal cords at the conclusion of neck dissection and thyroid and parathyroid surgery.38 While the patient is still under general anesthesia, the LMA is inserted behind the ETT and inflated. The anesthesiologist then removes the ETT, and the patient is allowed to breathe spontaneously. As the patient emerges from general anesthesia, a fiberoptic bronchoscope (FOB) is inserted through the lumen of the LMA to observe the function of the vocal cords. At M.D. Anderson Cancer Center, this technique has become an important diagnostic tool to detect the functional status of the nerves providing motor function to the larynx and has allowed the anesthesiologists and surgeons to make more informed decisions about the postoperative airway management of their patients. Similarly, patients undergoing brainstem surgery in the area that involves the lower cranial nerves, which control the pharynx and larynx, can be evaluated fiberoptically through the LMA in the intensive care unit. This helps the intensivist and the surgeon determine whether the patient will be able to maintain her or his airway postoperatively (Fig. 22-11).

3 Pulmonary Medicine and Thoracic Surgery
a Bronchoscopy in Children and Adults
Physicians in the fields of thoracic surgery and pulmonary medicine have shown interest in the LMA because of the unique access it provides to the larynx and respiratory tree. Diagnostic fiberoptic laryngoscopy and FOB can be performed readily through the LMA in patients under general anesthesia or under topical anesthesia with sedation.39–41 Maekawa and colleagues, in a 1991 letter to Anesthesiology describing the use of a size 1 LMA as a conduit for FOB with a 3.6-mm flexible endoscope in two children (ages 2 and 8 months), listed four advantages. First, the LMA tube is much larger (5-mm internal diameter) than the corresponding ETT, permitting the use of a larger bronchoscope, which gives a better view than that obtained through the 2- to 2.5-mm bronchoscope normally required to fit through the ETT in this age group. Second, the use of the LMA permitted examination of the larynx, including vocal cord movement and the part of the trachea normally occupied by the ETT. Third, the larger-diameter LMA airway tube permits easy ventilation, which permits uninterrupted observation. Fourth, not using an ETT may be valuable in cases of laryngeal or tracheal stenosis that may be made worse by the passage of the ETT.42
In a letter to Anesthesiology, Theroux and associates described the use of the size 1 LMA as a conduit for intubation in a 2.5-kg baby with Schwarz-Jampel syndrome who could not be intubated by other means.43 The uncuffed ETT was advanced over a 2.2-mm bronchoscope, which was easily passed into the trachea through the LMA. In 1997, Mizikov and coworkers reported their experience of using FOB through the LMA in 45 children: 15 diagnostic cases, 22 cases of lavage, 7 cases of foreign body removal, and 1 case of electrocoagulation of an adenoma.44 Total intravenous anesthesia and PPV were used in all cases. Patients’ ages ranged from neonatal to 15 years. They used the Olympus BF3C20 bronchoscope (3.6-mm diameter) with the size 1 LMA, and the Olympus BFP30 (5-mm diameter) was used with the size 2 LMA. The epiglottis was within the mask in 96.5% of cases but was not associated with significant airway obstruction in any case.
Related posts:
 Prehospital Airway Management
Prehospital Airway Management
 Medical-Legal Considerations: The ASA Closed Claims Project
Medical-Legal Considerations: The ASA Closed Claims Project
 Performance of Rigid Bronchoscopy
Performance of Rigid Bronchoscopy
 Intubating Introducers, Stylets, and Lighted Stylets (Lightwands)
Intubating Introducers, Stylets, and Lighted Stylets (Lightwands)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


