
INITIAL EVALUATION OF THE TRAUMA PATIENT
The assessment and management of the injured patient is a unique situation in which time and efficiency are of the essence. There is ample evidence in the literature that standardization of care improves outcomes and reduces morbidity and mortality in trauma patients.1 Multiple trauma systems exist in the United States and throughout the world. However, one well-regarded and widely practiced system of trauma patient assessment and management has significantly shaped the care of the trauma patient in the last 25 years.
Advanced trauma life support (ATLS) is a course provided by the American College of Surgeons; it is meant to prepare a variety of clinicians to treat, triage, and transport the broad spectrum of trauma patients. Introduced in 1978 and rapidly adopted throughout the United States, it is now taught in more than 50 countries. Now in its eighth edition, it is the gold standard for trauma patient assessment and management. ATLS protocols are based on a comprehensive review of the international literature to date.2
In ATLS, the initial assessment of the trauma patient is broken down into many components including; triage, preparation, the primary and secondary surveys and their radiologic adjuncts, ongoing resuscitation, and transfer to definitive care.
The primary survey consists of the ABCDEs (airway, breathing, circulation, disability, and exposure/environment). Adjuncts to the primary survey include plain radiographs of the chest and pelvis, and the focused assessment with sonography for trauma (FAST). The secondary survey is a quick head-to-toe physical examination, the purpose of which is to rapidly identify critical injuries and determine if these injuries are going to require further imaging or necessitate transfer to another facility for definitive care. The secondary survey may include simple or advanced imaging such as extremity plain films or computed tomography (CT) scans.
Throughout the primary and secondary surveys, resuscitation of the patient must be ongoing and continually reassessed. Upon completion of the initial assessment and resuscitation of the patient to a stable or semi-stable state, a decision must be made regarding transfer to definitive care. Transfer to an appropriate setting (operating room, intensive care unit [ICU], interventional suite) or facility (tertiary care center, level I trauma center, burn center) should be initiated as soon as possible after completing the initial assessment.
With timely diagnosis and intervention being the driving force in trauma evaluation, we need to determine if our emphasis on speed is supported by the data. Much has been described regarding the Golden Hour of Trauma, the 1 hour following injury when lives may be lost or saved by proper medical attention, but is this truth or myth?
The classical trimodal distribution of trauma deaths was first described in the seminal article by Trunkey in 1983, in which he demonstrated that almost half of all trauma deaths occurred in the first hour after injury.3 The other two peaks occurred within the next 1–4 hours and after the first week of injury. Trunkey considered many of the deaths occurring during the second peak (hours 1–4), as potentially preventable, and identification and treatment of these patients during the Golden Hour became the focus of the initial assessment. Great strides have been made in trauma systems management, prehospital emergency medical technology, resuscitation, and ICU care since this seminal paper. These advancements have resulted in more patients surviving to reach hospitals alive, and surviving after admission to the ICU, further emphasizing the need to concentrate on the early hours of trauma evaluation and resuscitation.4,5 In a study by Bansal in a level I trauma center in San Diego, while the majority of deaths still occurred within the first hour, a second peak occurred within hours 1–3, and hemorrhage continued to contribute to deaths up to 6 hours post injury4 (Fig. 21.1). A study by Demetriades et al.,5 also in a mature level I trauma center in Los Angeles, revealed similar information, with the majority of deaths upon arrival and a second peak of trauma deaths between hours 1–6.5 These studies also revealed that mechanism of injury (MOI) and body cavity involved affected time of death considerably.
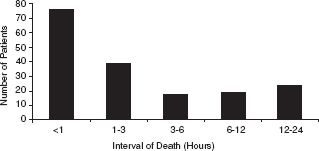
FIGURE 21.1. Distribution of in-hospital deaths over time for the first 24 hours after admission to trauma center (Data from Bansal V, Fortlage D, Lee JG, et al. Hemorrhage is more prevalent than brain injury in early trauma deaths: the Golden Six Hours. Eur J Trauma Emerg Surg. 2009;35:26–30.).
TRIAGE
The concept of triage is an essential element in modern medical care where resources are nearly universally exceeded by demand, even in highly developed, technically advanced centers. The basic tenants of triage incorporate accurate assessment of victims, victim acuity and available resources, and quickly assign the proper resources to the proper patients.6
Many protocols exist for prehospital triage of victims, determining the optimal distribution of patients to hospitals in the area based on victim factors such as acuity and age, and the resources of the area such as number of, and distance to, specialty trauma or burn centers. The ACSCOT has a protocol for this in Resources for the Optimal Care of the Injured Patient 2006.7
Outside of mass casualty and disaster management situations, categorization of traumas is generally based on patient acuity. Prior to the patient’s arrival, as much data from prehospital personnel should be gathered as possible. The components that determine level of acuity include clinical factors and MOI. Clinical indicators are subdivided into physiologic factors such as vital signs and level of consciousness, and anatomic factors such as body system involved—head, neck, thoracoabdominal, or isolated extremity trauma.
Trauma victims are generally classified into trauma team activations, urgent consults, or routine consults based on highest, medium, and lowest level of patient acuity and risk of substantial or operative injury. Trauma team activations (TTAs) are the highest level of trauma victims and generally require the presence of the most experienced trauma physician or surgeon, and the presence of the entire trauma team if one exists. Additional personnel who should be present at this level of acuity include an anesthesiologist or other airway specialist, radiology technologist, respiratory technologist, and trauma/emergency room/surgical ICU nurses. Additional personnel who may be helpful include a pharmacist, social worker, and ultrasonographer. Specific guideline for who must be present at TTAs for level I verification exist in the ACSCOT Resources for Optimal Care of the Injured Patient 2006.7
Many studies have validated this tiered system of trauma patient evaluation. A study by Petrie et al.8 in 1996, comparing TTAs requiring the involvement of the trauma team in the patient’s initial assessment and resuscitation to non-TTA trauma patients, revealed a notable improvement in the number of survivors compared to non-TTA patients per 100 population. This improvement in mortality occurred despite a considerably higher injury severity score (ISS). A similar study 10 years later by Cherry et al.,9 in 2007, revealed similar results: TTA protocols correctly identified patients with higher ISS, and early (<4 weeks) mortality, and TTA patients had significantly improved survival compared to their less injured non-TTA counterparts.
Clinical Criteria
Clinical criteria for level of trauma acuity include physiologic derangements of heart rate, blood pressure, and level of consciousness. In most trauma centers, patients with significant tachycardia (heart rate ≥120), hypotension (systolic blood pressure <90), or depressed mental status (Glasgow Coma Scale (GCS) < 8) are classified as a TTA. Additionally, most patients who were intubated in the field or require assisted ventilation also meet TTA criteria.
Clinical criteria have been repeatedly validated as useful triage tools.–912 Although debate does exist in the literature as to specific cutoff values for triggering a TTA, several studies have confirmed hypotension with systolic blood pressure <90 as an excellent predictor of mortality and injury severity.–911 Tachycardia with heart rate >120 beats per minute is also a validated triage criteria, though it appears to be less specific than hypotension. Depressed mental status with GCS < 8 is also highly predictive of mortality.9
Mechanism Criteria
Penetrating mechanisms such as stab wounds and gunshot wounds to the trunk or neck should be considered high-level traumas. Blunt mechanisms that indicate significant force include falls over 15 feet, automobile versus pedestrian, and high-speed motor vehicle crashes. Additional factors denoting involvement of great forces in the trauma are accidents with fatalities at the scene, crashes with significant passenger space intrusion, steering column deformation, ejection of the victim from the vehicle or rollover of the vehicle.
It must be kept in mind that MOI criteria in isolation have a very low predictive value in identifying severely injured patients.–911 MOI criteria are most helpful when taken into account with additional patient variables such as heart rate, GCS, and anatomic area of injury. Some studies suggest that experienced EMTs are very helpful in improving the positive predictive value of MOI criteria by exercising proper discretion upon application of MOI criteria in stable and evaluable patients in the field.10
Age Criteria
In the Primary Survey chapter of ATLS 8th Edition, care is taken to emphasize the increased incidences of comorbidities and need for specialized resuscitation strategies for the elderly trauma patient.13 While no specific age criteria for field triage currently exist in the ACSCOT guidelines, multiples studies confirm the unique characteristics of the elderly trauma patient.–1418 The older trauma patient has less physiologic reserve and a much lower ability to respond to injury compared to younger patients. Elderly patients are at increased risk for substantial and more advanced comorbid conditions such as hypertension, diabetes, coronary or peripheral vascular disease, chronic obstructive pulmonary disease, and emphysema. Because of these comorbidities, the elderly are more likely to be on medications such as beta blockers, calcium channel blockers, and diuretics; these medications may mask tachycardia, worsen hypotension, and interfere with efforts at resuscitation. Additionally, elderly patients with significant injuries may not meet traditional hemodynamic criteria for a TTA. The hypertensive patients may have a normal appearing blood pressure, but compared to their baseline this may be relative hypotension; alternatively, if the patient is on a beta blocker, substantial hemorrhage may be ongoing but the compensatory tachycardic response may be blocked. Elderly patients are also more likely to be on medications such as antiplatelet agents or anticoagulants, which considerably increase their risk of bleeding. In addition, elderly patients may have a baseline alteration in mental status or dementia, or have hearing or visual deficits, making communication and evaluation more difficult.
Several studies have demonstrated increased mortality in the elderly trauma patients even after correcting for injury severity.14,19–21 Additionally, analysis of mortality by age has identified 70 years or greater as the cutoff for considerably increased mortality.14 Using an age of 70 years or greater alone as a TTA criteria has demonstrated improved outcomes in trauma patients.19,20 In a series of studies by Demetriades et al., he noted that many patients 70 years or greater had severe injuries without meeting typical hemodynamic criteria for TTA (HR > 120, SBP < 90). The authors have also demonstrated improved survival in these patients after age alone was instituted as a TTA criteria.19,20 An additional study by Scalea et al.22 demonstrated that the elderly trauma patient had improved survival when early invasive monitoring was instituted.
Over and Undertriage
Because any triage system will not be perfect, they should be evaluated routinely to ensure over and undertriage rates are at acceptable levels. The ACSCOT has determined an acceptable under triage rate (seriously injured victims not taken to a trauma center) to be ≤5%, while the acceptable overtriage rate may vary from 25% to 50%. Because overtriage results primarily in overutilization of resources, while undertriage can result in missed injury, delay in treatment or death, there is a need to err toward overtriage rather than undertriage.
PREPARATION FOR PATIENT ARRIVAL
Given the importance of time in the initial assessment and management of the trauma patient, proper and thorough preparation prior to patient arrival is essential, and can prevent the loss of pivotal minutes in treatment after patient arrival. All monitoring devices, ECG leads, blood pressure cuffs in a variety of sizes, and pulse oximeter should be available. Warmed intravenous fluids, lactated ringers or normal saline should be available, as should blood products, O negative blood, and in some level I trauma centers, thawed universal donor plasma. Multiple intravenous access devices, angiocatheters in a variety of sizes, and central or intraosseous (IO) lines should be available, along with vacutainers for blood samples. Adjunctive devices such as suction canisters, laryngoscopes, masks and bags for ventilation, oral and nasal airways, urinary and nasogastric catheters, splinting or casting material, pelvic binders or sheets, and basic surgical instrument trays should also be available and kept stocked in standard locations that are easily and quickly accessible.
Prior to patient arrival, personal protective gear should be donned by all members of the assessment team. Universal precautions are necessary for all personnel coming into direct patient contact. Precautions should include occlusive gown, gloves, face shield or, at a minimum, eye protection, a mask and surgical cap if any sterile procedures are anticipated, and shoe covers. Protection is worn not only for the protection of the patient about to undergo sterile procedures, but for the protection of the staff from blood-borne infection. The incidence of blood-borne infections, most importantly HIV and Hepatitis C, vary in the literature, with recent studies revealing HIV in 1.4%–1.9% and Hepatitis C in 3%–8% of trauma patients.–2325 However, a series of studies from John Hopkins University revealed much higher rates of infection among trauma patients, 26% for HIV and 33% for Hepatitis C.26,27 The true incidence of HIV and hepatitis infection among trauma populations likely varies according to geography and type of hospital; however, full-barrier precautions should be universally employed.
PRIMARY SURVEY
The primary survey is a quick simple way to assess every trauma patient in a few minutes. Patients, upon arrival to the evaluation and resuscitation area, are visually surveyed for injuries; devices such as noninvasive blood pressure cuffs, pulse oximetry, and electrical cardiac monitors are used to obtain vital signs; large-bore intravenous access is established, and the patient is completely disrobed. The primary survey is performed by an experienced physician who should be designated prior to the patient’s arrival, and is performed while simultaneously addressing any life-threatening situations in real time as they are identified.
The physical examination of the primary survey is broken down into five basic components, ABCDEs. The ABCDEs are a sequence of physical examinations that are taught in ATLS to occur in a specific sequence. This sequence has been derived to address the most quickly life-threatening injuries most rapidly; as such, airway obstruction, which can lead to death in 1–5 minutes, is first, while equally important but less rapidly lethal conditions such as hypoxia and hypotension are second and third, respectively. In reality, many of the components of the primary survey occur simultaneously; equally, many problems in one area of the primary survey impact on other areas of the primary survey. For example, a tension pneumothorax, primarily a breathing problem, may result in the appearance of airway obstruction as the patient demonstrates air hunger or inability to vocalize, and may also impact circulation by decreasing preload and resulting in hypotension. Because of this, while the protocol of the primary survey addressing ABCDE in a strict sequence is done for medical priority, the informed clinician must also be able to keep the big picture in mind. Although not part of the list of life-threatening conditions, hemorrhagic shock remains the most common cause of death following injury. However, it is unlikely that patients arriving alive to trauma centers will die of exsanguinating hemorrhage within the first few minutes after admission. These individuals may still be bleeding, but compensatory mechanisms such as vasoconstriction and tachycardia, in addition to clot formation, develop to slow down bleeding and maintain perfusion to vital organs.6,28,29
Adjuncts to the primary survey exist in each of the categories; in the past, these have focused primarily on plain x-rays of the cervical spine (cross-table lateral view), chest, and pelvis. In most level I trauma centers today, less emphasis is placed on plain radiography of the cervical spine during the initial assessment when protection of the cervical spine far outweighs the need to diagnose injury. The most important adjuncts of the primary survey today include a single anteroposterior view of the chest and pelvis, and ultrasonography or FAST, which includes views of the abdomen and pericardium.
During evaluation of the ABCDEs, resuscitation should be ongoing and titrated to improvements or deteriorations in vital signs. A type and screen for type-specific blood and plasma transfusion should be the first priority in obtaining blood samples. Blood should also be drawn to obtain hematologic, chemical, and coagulation profiles. Pregnancy tests should be done in all females. In addition, every effort should be made to obtain an arterial sample for the analysis of oxygenation, hypercapnia, and acid–base status.
It is important to keep in mind that the primary survey is applicable to all trauma patients; while the anatomic and physiologic responses to injury may vary, the priorities for pediatric, geriatric, and obstetric trauma patients are the same.
AIRWAY
Addressing the airway is the highest priority in the initial assessment because obstruction, occlusion, or loss of airway is the most rapidly lethal of all injuries. The clinician must assess if the airway is patent, if it is protected, and if there is an evolving injury that may impact the future patency of the airway.
The easiest way to rapidly assess for both patency and protection of the airway is to ask the patient a simple question—“are you ok?”, “what is your name?” If the patient responds appropriately in a normal tone, timbre, and volume, you have assessed that they are conscious enough to protect their airway and that the airway is patent. The presence of hoarseness, weakness, or inability to speak in full sentences is an indication of impending airway compromise. Additionally, if there is gurgling, coughing, or obvious aspiration of material, this is definite evidence of obstruction. Lack of a verbal response, combativeness, or restlessness indicates inability of the patients to protect their airway. All of the above abnormalities require immediate intervention.
If airway compromise is diagnosed, the clinician should perform simple maneuvers such as the jaw thrust or chin lift, to bring the tongue and soft palate out of the oropharynx and provide high-flow supplemental oxygen by face mask. The oropharynx should be cleared with suctioning; care should be taken to avoid deep suctioning to prevent activating the gag reflex, causing vomiting and aspiration. Supplements to airway patency such as the nasal trumpet and oral airway can be considered. Care must be taken to use the oral airway only in completely obtunded patients again to avoid vomiting and aspiration. The oropharyngeal airway is placed with the aid of a tongue blade; in adults, it is inserted upside down, the end sliding along the palate, then rotated 180 degrees into proper position behind the base of the tongue; this is to avoid having the device push the tongue posteriorly during insertion and worsen obstruction. This maneuver is not used in children because of potential for injury to the palate. The nasal airway is generally well tolerated by conscious or semiconscious patients, and should be equivalent in length to the distance from the nares to the angle of the mandible. The nasopharyngeal airway should be lubricated, and then placed into one of the nares; however, it should not be used in the presence of obvious midface injury or possible facial fractures to avoid displacement of bone fragments or the device itself into the cranial vault (Fig. 21.2).

FIGURE 21.2. Basic airway adjuncts—mask with reservoir, oral and nasal airways.
A more advanced temporary airway is the laryngeal mask airway (LMA). This soft plastic device, invented in 1983 by British anesthesiologist Archie Brain, comes in a variety of sizes and is meant to fit the posterior oropharynx. The LMA is placed in the supraglottic position and an inflatable cuff is deployed to seal the oropharynx for spontaneous or manual ventilation. A drawback of the LMA is that it does not fit into the trachea, so communication between the esophagus and trachea remains completely open and aspiration remains a significant risk. Some improvements in the design of the LMA have included esophageal drainage ports, and the ability to use the LMA to guide placement of an endotracheal tube (ETT). This last option may be attractive in patients with known or highly suspected cervical spine injuries where minimization of neck movement is of the utmost importance, and laryngoscopy may be difficult or impossible. However, optimal placement of the LMA, similar to intubation, often requires extension of the head on the neck, and, at a minimum, the jaw must be thrust forward for optimal placement. As with any airway maneuver, LMA placement is not risk free, and must be undertaken while simultaneously protecting the cervical spine with in-line traction.
Other supraglottic airways include the King Laryngeal tube and the esophageal/tracheal Combitube. These devices are meant to be inserted blindly or with the aid of a laryngoscope; they contain a large superior cuff to seal the supraglottic pharynx, and a smaller inferior cuff. In the case of the King Laryngeal tube, the smaller cuff is preferentially inserted into, and inflated in, the esophagus. Ventilation is achieved through port holes between the upper and lower cuffs in the supraglottic pharynx just above the trachea; the superior cuff prevents air leakage from the mouth and nose, and the inferior cuff prevents insufflation of the stomach and decreases risk of aspiration. The Combitube is also inserted blindly, and the superior cuff is inflated to prevent air leakage from the mouth and nose. However, the tube may be inserted into either the trachea or the esophagus; the distal portion of the tube enters the esophagus in over 90% of insertions.30 Once the tube is placed, both cuffs are inflated. Once the cuffs are inflated, there are two ports to ventilate through—a distal port below the distal cuff can be used if the end of the Combitube is within the trachea—and ventilation proceeds as with any ETT. If, in contrast, the distal tube is in the esophagus, the patient is ventilated through proximal ports located between the superior and inferior cuffs, and ventilation proceeds through the supraglottic oropharynx, and the distal cuff prevents esophageal/stomach insufflation, as in the King Laryngeal tube. A comprehensive review of acute airway management is beyond the scope of this chapter and can be found in the Airway Control Chapter 12 of Trauma 6th Edition.31
All above-mentioned maneuvers are temporizing and if the airway compromise does not resolve, a definitive airway is indicated. Strict indications for a definitive airway include obvious or impending airway obstruction, obtundation with GCS < 9, and respiratory insufficiency (hypoxia, hypercarbia, apnea). Definitive airways include orotracheal or nasotracheal intubation and surgical airways—cricothyroidotomy and tracheostomy.32
Placement of a definitive airway in the comatose patient can generally be accomplished without sedating or paralyzing medications, which has the benefit of avoiding pharmacologic interference with neurologic examination and possible hemodynamic compromise that is a side effect of many such agents. Additionally, the use of a paralyzing agent can often turn an urgent airway situation into an emergent airway; loss of the small amount of muscular tone in the pharynx can cause partial obstruction to turn into complete obstruction, making bag-mask-valve ventilation impossible. Occasionally, in the comatose patient, increased muscular tone and biting in the semiconscious patient make sedating and paralytic agents a necessity, as does intubation of the conscious patient. If the clinician tests jaw rigidity by performing a jaw thrust or attempts to gently open the jaws with the scissor technique and meets resistance, a sedative and paralytic should be used prior to any attempt at obtaining a definitive airway. Rapid sequence intubation is a technique of administering bolus doses of a sedative and paralytic simultaneously while using cricoid pressure (the Sellick maneuver) to prevent aspiration and the use of minimal or no preoxygenation to prevent gastric insufflation and minimize aspiration risk. One common agent used, Etomidate, is a short-acting sedative with relatively minimal cardiodepressive effects; the dosage is 0.3 mg/kg and induction occurs in 30–60 seconds. There is some suggestion in the literature that Etomidate may result in adrenal suppression and relative adrenal insufficiency, but this is still an area of active research. Some alternative sedatives include Propofol, which is also very rapid in onset, and short acting, or benzodiazepines. However, both may result in significant cardiac depression and hypotension. A popular paralytic agent is Succinylcholine, which has a rapid onset and brief duration of action. The induction dosage is 0.6 mg/kg, and the onset of action is typically within 60 seconds with a duration of 2–3 minutes. Succinylcholine is a depolarizing agent, and may result in malignant hyperthermia, and can cause cardiac arrest due to severe hyperkalemia in certain patients, including victims of burns, drowning, spinal cord transaction, and severe crush injury. In such patients, a non-depolarizing agent such as Vecuronium or Rocuronium should be considered; although the onset of action of these agents is slightly slower, their duration of action can persist much longer than with Succinylcholine, which may interfere with future neurologic examinations. If paralytic agents are used, it is important to obtain a very quick neurologic assessment prior to their administration. If 5–10 seconds can be spared, an assistant should ask the awake patient to move his or her arms/legs and briefly assess sensation, and perform a pupillary exam. In the comatose patient, painful stimuli should be applied to the arms/legs to see if any movement is elicited.
Once the patient is properly anesthetized, the preferred definitive airway is orotracheal intubation. It provides a rapid definitive airway, and the materials required to accomplish it are readily available in most health care settings. Preparation is the key in the successful intubation of a trauma patient. The most experienced physician should be utilized, and several well-trained assistants should be used to bag the patient, provide requested supplies, and maintain in-line cervical spine stabilization in addition to cricoid pressure. Equipment should include a laryngoscope with several types and sizes of blades and the light bulb should be checked for function prior to patient arrival. Other equipment includes several sizes of ETT, a stylet, equipment to suction the oropharynx, and a syringe for inflating the cuff. A minimum of three people should be involved in the intubation of the trauma patient, if at all possible. The most experienced person should be located at the head of the bed in position to intubate, the second most experienced should be in position below and to the side of the head of the bed to maintain the cervical spine in neutral position, and a third should be to the side of the bed to apply cricoid pressure if necessary and hand equipment to the person performing the intubation. All extraneous material should be removed from the patient’s head and neck; the anterior portion of the C-collar be removed. The assistant maintaining cervical spine precautions must ensure that the head is maintained in line, and that the head is not extended during intubation.
Once intubation is accomplished, appropriate positioning of the ETT should be confirmed, clinically by observation of chest movements and auscultation, with a carbon dioxide detector, and radiographically. Clinical confirmation of placement is notoriously unreliable, and such markers as equal chest rise, symmetric bilateral breath sounds, and condensation on the ETT cannot be used alone for confirmation.33 Capnography is most reliable for confirmation that the ETT is in the airway; if this is not available, colorimetric carbon dioxide detectors can be used. False-positive color change can occur with gastric intubation, but will generally fade after the first few breaths. False-negative color change can occur in patients in cardiac arrest as carbon dioxide production may be below threshold levels for detection. These instances all make continuous capnography much preferable to colorimetric detectors. Lastly, once the primary survey is completed and the patient is stable or semi-stable, a chest x-ray can confirm placement of the ETT in the trachea. Care should be taken to ensure it is not in one of the mainstem bronchi and that both lungs are equivalently inflated. Once successful tracheal intubation is confirmed, the rigid cervical collar should be reapplied. It is important that all personnel involved in the intubation remember that protection of the cervical spine is necessary at all times. Other devices such as the long backboard, sandbags, and struts with binding tape can also be used to immobilize the cervical spine.
Even after the placement of the ETT has been confirmed and it has been secured in place, care must be taken to repeatedly check that it has not been dislodged or become obstructed. Particular care must be taken to inspect for proper placement of the ETT after the patient has been moved or repositioned.
In some cases, traditional orotracheal intubation can be difficult or impossible; some high-risk situations include the obese patient, patients with substantial oromaxillofacial trauma or blood loss, mucus or emesis in the airway, patients with facial burns or inhalation injury, and patients with trauma to the neck. If available, every effort should be made to involve a clinician with advanced airway training such as the trauma surgeon, anesthesiologist, or otolaryngologist. In high-risk cases, the tools for a surgical airway should be immediately available and consideration should be given to using advanced airway adjuncts. Advanced airway tools include the bougie, Glide scope, fiberoptic intubation, and retrograde intubation (Fig. 21.3).

FIGURE 21.3. Definitive airway devices—ETT, LMA, bougie.
The bougie is a semirigid, long plastic tube with an upward angled tip; it can be passed blindly, or with laryngoscopic guidance, the upward angle preferentially directs it toward the tracheal aperture and away from the esophagus, as does the presence of cricoid pressure. The physician should be able to feel the tip pass the tracheal rings as bumps, then stop advancing when it encounters the carina, and in most cases, turn sharply right following the right mainstem bronchus. The bougie can then be used as a guide for placement of the ETT in a Seldinger-type technique.
Other advanced airway techniques include use of a Glide scope, fiberoptic intubation, and retrograde intubation. The Glide scope is a laryngoscope with a camera located on the end of the laryngoscope blade. The image is sent to an attached video screen, allowing the clinician to more easily visualize the vocal cords, especially in a very anterior airway. It also allows for successful intubation with less risk of hyperextension of the neck in patients with possible cervical spine injury. Fiberoptic intubation is also an option in the potentially challenging airway. However, because fiberoptic intubation requires specialized equipment and training, it is not recommended for emergency airways, rather it is more suited to the semi-elective situation. It is particularly useful in patients that are stable or semi-stable but have injuries that make impending airway loss a high risk, such as burn patients without immediate airway compromise, patients with neck injury with possibility of expanding hematoma, or stable patients with oromaxillofacial trauma. Fiberoptic intubation ideally should take place in the operating room with surgical airway tools available should it fail. Another advanced airway technique is retrograde intubation, which is a hybrid between orotracheal intubation and surgical cricothyroidotomy. The airway is accessed via the cricothyroid membrane as in cricothyroidotomy, a wire is passed through the membrane and retrieved from the oropharynx with Magill forceps, the wire is held taught with clamps on either end and Seldinger technique is used to pass an ETT over the wire into the airway in a blind fashion.–3436
If the airway cannot be secured using the above techniques, or in cases where airway injury is suspected and attempts at intubation risk further injury, the goal should be to obtain a surgical airway immediately. Definitive surgical airways include cricothyroidotomy and tracheostomy. In the case of suspected or known laryngeal injury, a cricothyroidotomy would be above the level of the injury and in this case, emergent tracheostomy is the preferred airway. In all other cases, cricothyroidotomy is the preferred surgical airway. Cricothyroidotomy can be performed with percutaneous or open technique. In the traditional open technique, very few pieces of specialized equipment are necessary; a scalpel, small retractors, a Kelly, and ETT or tracheostomy tube are the only essential items. The patient’s neck is exposed, again, an assistant is used to maintain strict cervical spine immobilization, the cricothyroid membrane is palpated between the thyroid and cricoid cartilages, a vertical midline incision is made in the skin, the membrane is exposed and divided in the transverse direction to avoid injury to the overlying vocal cords, and the ETT or tracheostomy tube is placed into the airway. Clinical exam and capnography are then used to confirm placement into the airway. In the obese patient or the patient with significant soft tissue injury that distorts the traditional landmarks, the cricoid cartilage can be located by placing the smallest finger of the clinician’s right hand into the sternal notch; the index finger is then located immediately above the cricothyroid membrane. Many companies manufacture kits for percutaneous cricothyroidotomy. The kits will generally include a scalpel to create the incision, a large-bore needle for accessing the airway through the membrane, a wire to pass through the needle, a plastic dilator to create a passage, and a small rigid tube similar to a tracheostomy tube for ventilation.
There is some debate as to whether or not cricothyroidotomy tubes need to be replaced with a formal surgical tracheostomy for long-term ventilation. Traditionally, all cricothyroidotomies were converted electively to tracheostomies for fear of subglottic stenosis caused by irritation of the airway. However, recent studies in trauma and ICU populations have demonstrated no increased risk of stenosis compared to tracheostomies.–3740 These studies reveal that the rates of tracheal stenosis up to 60 months following decannulation are lower than previously thought (overall <3%), and are comparable to rates of stenosis following tracheostomy.39 They additionally show equivalent rates of successful decannulation, and some reveal a significantly higher rate of complications associated with conversion to tracheostomy.37,40 Although long-term use of cricothyroidotomy is still an area of controversy, its routine conversion to tracheostomy should be questioned.
In certain patients, the airway may be patent and protected upon initial inspection but may be in danger of rapidly becoming compromised. These high-risk patients benefit from elective placement of a definitive airway in a controlled fashion prior to the development of symptoms or frank airway compromise. Elective intubation to secure a definitive airway is particularly important if the patient will require transport to another location for definitive care, or if prolonged diagnostic studies are planned. Such situations include patients with significant burns, especially if the burn involves the face, or if there is evidence of inhalational injury, patients with substantial oromaxillofacial or neck trauma, where subsequent soft tissue swelling or copious bleeding or secretions may rapidly obstruct the airway, and patients with significant traumatic brain injury where declining or waxing and waning GCS may lead to inability to protect the airway. Finally, agitated and combative patients or those with acute alcohol or drug intoxication may be unable to protect their airway and should be promptly intubated as well.
Pediatric Airway
Intubation of the pediatric trauma victim requires knowledge of the anatomic and physiologic differences in pediatric patients. Children are obligate nasal breathers, so keeping the nasopharynx clear of obstruction, mucus, and blood is of paramount importance. Supplemental oxygen must be directed toward nasal breathing. If definitive airway is indicated, orotracheal intubation is again the preferred route, but it may be more challenging, especially to the inexperienced clinician. In particular, the pediatric airway is more challenging not simply due to smaller size but also because the epiglottis is proportionally larger and more floppy in children than adults and more difficult to maneuver around. Additionally, the airway is higher and more anterior, making visualization during direct laryngoscopy more difficult. Because of these anatomic features, intubation may be easier with the use of a straight or Miller blade, which can be used to directly lift up the epiglottis, allowing visualization of the true vocal cords. Lastly, the airway is proportionally shorter in children, this coupled with their smaller stature overall makes bronchial intubation a much higher risk in children. Outside of the airway itself, children have a more pronounced vagal response and may develop considerable bradycardia, which is also more likely to be severe and rapid in onset in response to hypoxia. Because cardiac output is primarily determined by heart rate in children, bradycardia will result in notable hypotension and hypoperfusion. Therefore, atropine should, at a minimum, be available during any airway maneuver, and prophylactic administration prior to laryngoscopy is widely practiced.
Proper sizing of the ETT can be determined by three general methods. First, the Broselow tape can be used to estimate the patient’s weight and all equipment and drug dosages required for intubation; second, the patient’s small finger is a rough estimate of the external diameter of the ETT; lastly, the modified Cole formula can be used. The (childs age + 4)/4 will give the optimal internal diameter of the ETT. The ETT should be inserted to a depth of three times the internal diameter of the ETT used. Again, care must be taken to confirm appropriate position of the ETT after intubation, keeping in mind the much higher risk of bronchial intubation. Tracheal placement can be confirmed with auscultation of symmetric breath sounds over both lateral lung fields, equivalent chest rise bilaterally, return of carbon dioxide on capnography or colorimetry, and lastly, with radiographic evaluation.
One area of controversy is the use of cuffed versus uncuffed ETTs in the pediatric population. Traditionally, it has been taught that all children <8 years of age should be intubated with an uncuffed ETT, to avoid compression of the tracheal mucosa against the nondistensible cricoid ring, which in children is the narrowest portion of the airway. This was thought to prevent post-extubation stridor and tracheal stenosis. However, there has been little in the literature to support such claims of damage. Additionally, ETTs today are technically advanced over earlier models and the low-pressure, high-volume cuffs much less damaging. Recent changes in pediatric guidelines from the American Heart Association in 2005 and the Resuscitation Council of the United Kingdom in 2005 regarding CPR in pediatric and neonatal patients state that cuffed ETTs may be used in infants and children (except newborns), and that provided proper cuff pressures (<20 cm water) are used, they are as safe as uncuffed ETT.41,42 Additionally, rather than age, the primary determinants for use of cuffed or uncuffed ETT in children should be the underlying reason for intubation and suspected duration of intubation.–4246 In particular, patients with burns or severe pulmonary injuries that are likely to require prolonged intubation with higher levels of ventilatory support will likely benefit from the use of cuffed ETT.44,45 In these patients, the use of cuffed tubes will aid in the delivery of adequate ventilation at higher pressures, and prevent the need for dangerous ETT exchanges due to air leaks, which occur frequently in this population.44,45 Even in the elective surgical population, there is level I evidence that the use of a cuffed ETT decreases the number of re-intubations or ETT exchanges due to sizing or air leak without any increase in unsuccessful extubations or post-extubation stridor in patients younger than 5 years.46 While these studies apply primarily to the in-hospital population, there is a growing body of evidence to support the use of uncuffed ETT in the prehospital setting as well, though further studies are required before this can be recommended.43
If orotracheal intubation is unsuccessful, a surgical airway is indicated as in adults. However, cricothyroidotomy is not recommended for pediatric patients under 12 years of age. Instead, the airway is accessed with percutaneous placement of a large-bore needle into the cricothyroid membrane and jet insufflation is used to temporarily oxygenate the patient. Air is insufflated at high pressures using jet insufflation in order to overcome the high resistance of the long, narrow catheter. Insufflation is performed for 1 second with intervening 4-second intervals to allow passive release of carbon dioxide. Ventilation is necessarily restricted and carbon dioxide levels will predictably rise over time. Conversion to a tracheostomy or repeated attempt at intubation with advanced airway adjuncts or more experienced personnel must be performed within the next 45 minutes once oxygenation is improved to prevent the accumulation of unacceptable levels of carbon dioxide.47
BREATHING
Once the airway has been assessed as patent or a definitive airway has been secured, the primary survey moves on to breathing. Breathing encompasses a brief inspection of the chest and assessment of the adequacy of oxygenation and ventilation. Conditions in this realm that should be diagnosed in the primary survey include tension pneumothorax, open pneumothorax (or sucking chest wound), massive hemothorax, and flail chest.
Assessment begins with visual inspection of the thorax, all clothing must be removed and the anterior and posterior chest and axillae should be inspected for lacerations, ecchymoses, open wounds, air bubbling from wounds, symmetry of chest rise, paradoxical motion of any portion of the chest, and the use of accessory muscle for respiration. Pulse oximetry should be applied as soon as the patient arrives, and continuously reassessed for sufficiency. The chest should be palpated for crepitus, tenderness, and instability of the sternum or ribs. The chest should be auscultated for the presence and symmetry of breath sounds, and dullness of cardiac or breath sounds. Lastly, a chest x-ray should be performed as soon as is feasible to radiographically evaluate the soft tissues, bones, lung parenchyma, and thoracic cavities. Throughout the assessment, high-flow oxygen should be administered to the patient.
Tension pneumothorax is the most rapidly life-threatening of all breathing problems. It occurs when air continuously enters the thoracic cavity from the lung, airway, or atmosphere and cannot escape. The pressure causes collapse of the lungs, preventing oxygenation and ventilation on the ipsilateral side, and eventually causes deviation of the mediastinum away from the tension pneumothorax. This causes compression of the superior and inferior vena cava, decreasing preload to the heart and resulting in hypotension. Tension pneumothorax should be recognized immediately by air hunger, hypoxia, tachypnea, hyperresonance, unilateral absence of breath sounds, deviation of the trachea away from the affected side, distended neck veins, hypotension, and tachycardia. Crepitus may be felt as well, but is nonspecific. The tracheal deviation may be difficult to visualize with a rigid cervical collar in place, and may be prevented from occurring if the patient is intubated as a greater pressure is required to deform the more rigid plastic ETT. Additionally, distended neck veins may not be present if the patient has concomitant hypovolemia. Lastly, tension pneumothorax may be confused with pericardial tamponade as both result in distended neck veins, a feeling of impending doom or restlessness, and hypotension. However, tamponade will result in muffled heart sounds and does not cause tracheal deviation or asymmetrical breath sounds. If tension pneumothorax is suspected, emergent decompression must be performed. ATLS recommends needle decompression with large-bore needles or angiocatheters placed in the second intercostal space in the midclavicular line. If the needle is properly placed, a rush of air should be observed with an immediate improvement in vital signs, as the tension pneumothorax is converted to a simple pneumothorax. This should then be followed by the placement of a chest tube for more permanent decompression of the affected hemithorax, and drainage of any blood that may be associated with the tension pneumothorax.
If no air is noted, the needle may be in the subcutaneous tissue, there may be no pneumothorax, or the wrong side may have been accessed. A second decompression of the contralateral chest should be undertaken; if no rush of air is again noted, tension pneumothorax is unlikely and cardiac tamponade should be considered, and rapid FAST should be performed to assess for pericardial fluid. Occasionally, in the obese patient or in patients with significant soft tissue edema/hematomas, needle decompression may not be possible as the device may not be long enough to reach the thoracic cavity in this situation, or if the clinician is very comfortable with chest tube placement, needle decompression may be skipped in favor of immediate chest tube placement.
Chest tubes in experienced hands can be placed in <60 seconds. The most important step is the entry of the thoracic cavity to allow escape of the air trapped there, which is accomplished even more rapidly and occurs once the thorax has been entered by blunt dissection. The chest tube should be placed in the midaxillary line in the fourth or fifth interspace at the level of the nipple in males, and the inframammary fold in females. A small incision, approximately 1.5–2 cm in length, is made with a scalpel, a clamp is used to bluntly dissect the subcutaneous tissue until the bony rib is felt. The clamp is then used to bluntly enter the thoracic cavity immediately over the top of the rib to avoid injury to the neurovascular bundle located beneath each rib. Significant force may be required to create this entry. A rush of air or blood should be observed upon entry into the pleural cavity, immediately relieving intrathoracic tension and improving the patient’s vital signs. The clamp is then used to bluntly spread the soft tissues, creating an opening in the intercostal tissue to accommodate a 36 French chest tube. Digital manipulation should be used to guide the tube posteriorly and cephalad to drain the thorax. In most adults, insertion of 10–12 cm of the tube should be adequate to ensure the last side port is within the chest cavity. In all cases, further advancement of the tube should be stopped as soon as resistance is felt. The tube is then secured in place with a suture and the insertion site dressed with an occlusive dressing. The end of the tube should then be connected to a closed drainage system. In all trauma patients, this collection system should be prepared sterilely with citrate, an anticoagulant, so that any collected blood can be autotransfused back into the patient if desired.
In cases where the tension pneumothorax has been converted to simple pneumothorax by needle decompression or in cases of simple pneumothorax or simple hemothorax, care should be taken during placement of chest tubes to maintain sterility. A cap, mask, gown, and sterile gloves should be worn by the clinician and a cap and mask should be worn by everyone in the room. Chlorhexidine preparations are preferred over povidone antiseptics as they have a decreased risk of surgical site infections. The site should be properly cleansed and anesthetized and completely draped to avoid contamination of the site, instruments, or chest tube. A single dose of pre-procedure antibiotics with gram-positive coverage has proven as effective as a 24-hour course of periprocedure antibiotic prophylaxis. Antibiotic prophylaxis longer than 24 hours is not effective in preventing infection or empyema and is not recommended.
Massive hemothorax may also present with tension physiology. Hypotension may be a result of decreased preload from tension physiology as well as from massive blood loss. Treatment is immediate placement of a chest tube to the affected side. In contrast to tension pneumothorax, massive hemothorax rarely results in distended neck veins because of associated hypovolemia. Blood loss of >1,500 mL defines a massive hemothorax and is an indication for operative exploration. Additional indications for thoracotomy include massive continuous air leak, which may indicate massive parenchymal lung injury or injury to a major airway, and blood loss of 200 mL an hour for >4 hours. Again, every effort should be made to collect shed blood in a sterile fashion so that it may be autotransfused. Anticoagulation can be accomplished by the addition of citrate, in a 1:7 ratio, to the blood being transfused. After the addition of citrate, the blood can be immediately transfused back into the patient with the use of a standard blood filter and tubing. Many studies have demonstrated the safety of autotransfusion of blood collected from traumatic hemothorax.48,49 Though the character of the autotransfused blood has not been extensively studied, available data would suggest that this blood is inherently depleted of coagulation factors, particularly Factor VIII and fibrinogen, as well as platelets; however, studies of circulating blood after autotransfusion show only mild increases in PT/aPTT, and a moderate decrease in circulating platelets.50,51Consideration should be given to additional transfusion of platelets when massive autotransfusion occurs.
Open pneumothorax, or sucking chest wounds occur when a defect in the chest wall is full thickness and large enough for air to communicate between the thoracic cavity and the environment. During inspiration, negative pressure in the thoracic cavity sucks air into the hemithorax, preferentially over the lungs, resulting in hypoxia. The wound should be grossly decontaminated by removal of metal, dirt, and other visible objects, and an occlusive dressing should be applied and secured on three sides. This prevents air from being sucked into the thoracic cavity, but if intrathoracic pressure builds, it may escape from under the fourth side, preventing tension physiology from developing. A chest tube should be placed to relieve the pneumothorax as soon as possible. When the initial assessment is completed and the patient is stable, the wound should be cleansed, debrided, and closed in the operating room.
A flail chest occurs when three or more contiguous ribs are broken in two places, creating a segment of bone and muscle that can move independently of the thoracic wall (Fig. 21.4). This independent segment will move paradoxically with spontaneous respirations, pulling inward with inspiration secondary to negative intrathoracic pressure. This paradoxical motion can cause significant pain to the patient as the broken ribs grate upon one another, resulting in desire to take rapid shallow breaths, causing atelectasis and hypoxia. Additionally, the force required to create a flail segment is excessive and usually also results in significant underlying pulmonary contusion further increasing hypoxia. Lastly, the flail segment may be associated with a hemothorax or pneumothorax. These are treated with a chest tube as previously described. Treatment of the flail segment varies according to patient presentation. If stable, supplemental oxygen, aggressive pulmonary toilet, and adequate analgesia are suitable. Pain can be controlled with oral medications, intravenous medications, patient-controlled analgesia, local anesthetic with rib blocks, or catheters that deliver a continuous stream of local anesthetic, or with epidural anesthesia. There is evidence that epidural pain control is superior to other methods.52,53 In unstable or semi-stable patients, intubation and positive pressure ventilation are the best treatments. The intubation allows more aggressive pain management and sedation; the positive pressure ventilation can be used to recruit atelectatic lung, and support contused lung to improve oxygenation. Additionally, the positive pressure ventilation splints the flail segment so that the paradoxical motion is halted and the entirety of the thoracic wall can move in synchrony, relieving pain and allowing healing of the soft tissue and bones. The elderly patient is particularly susceptible to deterioration after chest trauma, and pain management and pulmonary toilet should be very aggressive, with a low threshold for intubation. Avoidance of fluid overload in patients with flail chest and large pulmonary contusions is also advisable.
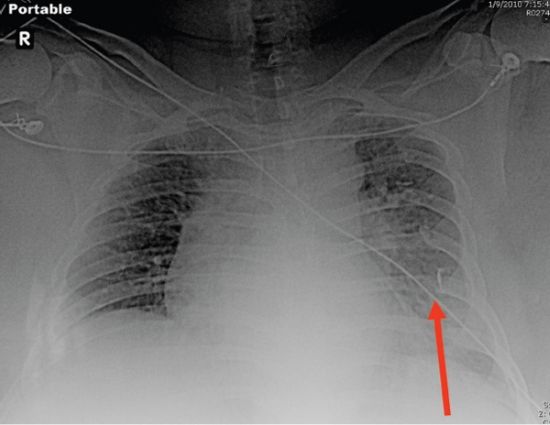
FIGURE 21.4. Chest x-ray showing multiple left-side rib fractures (flail chest).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


