Fig. 36.1
Illustration demonstrating the musculotendinous anatomy of the lateral aspect of the elbow, near the site of the tendon origin on the lateral epicondyle (Reproduced with permission from Philip Peng Educational Series)
Symptoms
The main presenting symptom is stabbing elbow pain (lateral epicondyle), radiating as far as the thumb (Fig. 36.2). Physical examination reveals point tenderness in the region of the lateral epicondyle and pain and weakness exacerbated by resisted wrist extension and supination (Cozen test and third-digit tennis elbow test).
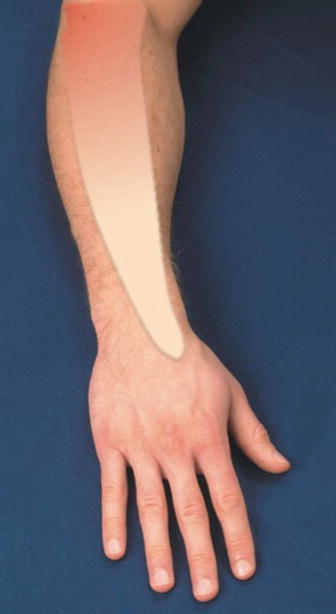
Fig. 36.2
Diagram showing the pain area in a patient with tennis elbow (Reproduced with permission from Philip Peng Educational Series)
Procedure
The patient is usually in sitting position with the elbow 90° in flexion rest comfortably on a pillow over a table. With sterile precaution, a linear high-frequency probe (6–13 MHz) is placed over the lateral elbow region, revealing the lateral epicondyle, capitellum, and head of radius (Fig. 36.3). The target structure CET can be visualized in long-axis view. A 23-G or 25-G needle is inserted in-plane from inferior to superior direction all the way to the epicondylar insertion of CET (Fig. 36.3). Applying light pressure to the plunger of the syringe while withdrawing the needle, the steroid solution is injected in the target point. The practitioner should avoid over-pressurizing the plunger which may cause artificial tissue injury. The total volume is approximately 1 mL with a mixture of local anesthetic and 10 mg of triamcinolone.
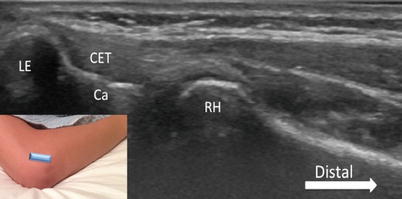
Fig. 36.3
Sonogram of the common extensor tendon (CET) on its long axis. The position of the ultrasound probe is shown in the inset, with the cranial end of the probe placed on the lateral epicondyle (LE). The CET origin is seen as a continuous band of longitudinally oriented fibers. Ca capitellum, RH radial head (Reproduced with permission from Philip Peng Educational Series)
When tendon fenestration is performed, the patient position, scanning procedure, and needle used are the same. The needle repeatedly fenestrate the tendinotic tendon until the tissue is softened, and crepitation is diminished.
Intra-articular Injection of the Elbow Joint
The elbow joint is a compound joint formed by the proximal ends of the ulna and radius and the distal end of the humerus. The ulna (olecranon) and humeral capitellum form a hinge joint (Fig. 36.4). The radial head articulates with the capitellum of the humerus, allowing swivel movement, while it also revolves within the radial notch of the ulna. Both movements from radial head articulations allow axial rotation of the forearm (Fig. 36.5). The joint capsule encloses the entire elbow joint including three fat pads in different fossae: radial, coronoid, and olecranon fossae (Fig. 36.5). The elbow joint is transversed by three nerves, and understanding the anatomy is important to avoid nerve injury to these nerves (Fig. 36.6). At the level just proximal to the elbow joint, the radial nerve is sandwiched between the brachioradialis and brachialis muscles, the ulna lies subcutaneously lateral to the medial head of the triceps muscle in the posterior compartment of the arm, and the median nerve runs besides the brachial artery lateral to the biceps brachii and brachialis muscles.