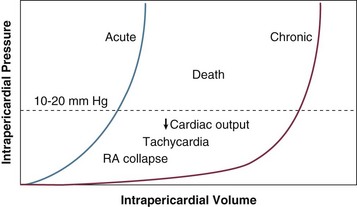
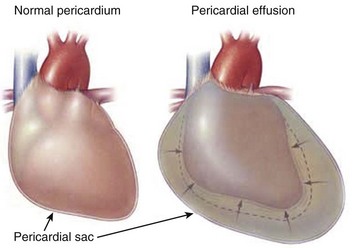
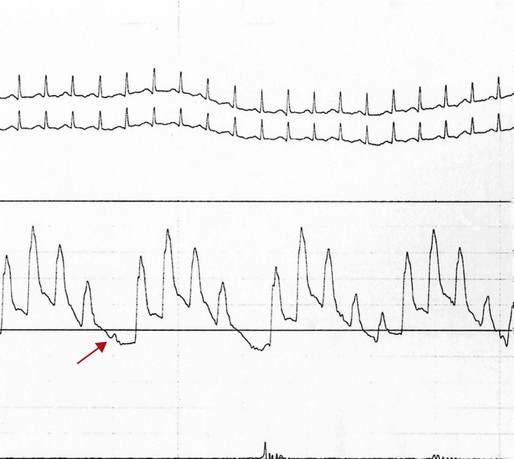
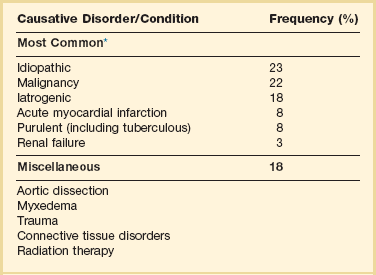
24 Cardiac tamponade is a condition characterized by an increase in pressure external to the heart resulting in impaired filling of the cardiac chambers. In the typical scenario, as fluid in the pericardium accumulates, cardiac output falls. The diagnosis represents a continuum from mild tamponade with subtle diagnostic findings to a critical clinical setting with imminent mortality.1 The variability in presentation, including diagnostic findings and course, and the morbidity and mortality associated with treatment make this a particularly challenging clinical problem in critical care medicine. The pericardium consists of a visceral and a parietal pericardial segment, the former being composed of a single layer of cells that adhere to the cardiac epicardial surface.2,3 The parietal pericardium is the structure responsible for the clinically relevant features of tamponade; it is a relatively noncompliant structure composed of collagen and elastin and normally is less than 2 mm thick. The mechanical properties of the pericardium—in particular, those reflected by its pressure-volume curve (Fig. 24.1)—are responsible for the clinical features seen in cardiac tamponade. The pericardium extends from the lower third of the superior vena cava to the apex of the heart. It is attached to the sternum, the diaphragm, and the great vessels. Because it extends beyond the heart border, trauma to not only the heart but also the great vessels approaching the heart borders can lead to cardiac tamponade.4 Cardiac tamponade is a result of decreased transmural pressure, typically from the accumulation of fluid in the pericardial space (Fig. 24.2). Other causes of “tamponade-like physiology” are related to extrinsic compression of the heart,5 although these pathologic processes should be separated from those causing constriction rather than true tamponade. Differentiating these two distinct physiologic entities, constriction and tamponade, is essential to diagnosis and management. The fluid accumulating in the pericardial space can be blood, serous fluid, purulent material, clot, or rarely gas. As fluid accumulates, the pericardium stretches, until it reaches a point (see Fig. 24.1) at which its degree of compliance is exhausted, so that it has become largely inelastic. At this point, any further increase in intrapericardial fluid is associated with a decrease in intracardiac chamber volume, because the total volume of pericardial fluid, heart muscle, and the cardiac chambers becomes fixed by pericardium no longer able to stretch. This in turn results in decreased filling of the heart and consequently decreased stroke volume. To maintain cardiac output, an early compensatory mechanism is an increase in heart rate. Subsequent adaptations to maintain blood flow to central end organs (heart, brain, kidneys) are venous pressure rise, peripheral vasoconstriction, increase in ejection fraction, and selective shunting of blood to preserve flow to the essential end organs. Venous pressure increase is accomplished by fluid retention and peripheral venoconstriction. In severe tamponade, equalization of right atrial, right ventricular diastolic, pulmonary diastolic, pulmonary artery wedge, and intrapericardial pressures occurs. Both pulmonary and systemic arterial and pulse pressures fall. Tamponade is a continuum, ranging from a primarily echocardiographic finding of right-sided chamber collapse to shock and pulseless electrical activity. The normal parietal pericardium, because of its limited compliance, limits abrupt expansion of the heart as a whole.6 Thus, in the setting of right ventricular infarction, for example, acute dilation of the right ventricle is at the cost of left ventricular volume decrease—a ventricular interdependence phenomenon similar to that illustrated in Figure 24.3. Acute chamber enlargement resulting from other etiologic conditions or disorders, such as abrupt volume loading or sudden onset of severe valvular regurgitation, is impeded by the constraint of pericardium that has reached the limits of its intrinsic elasticity. Because right-sided heart filling occurs preferentially with inspiration, when negative intrathoracic pressures result in increased venous return and higher right-sided chamber volume, left ventricular stroke volume and hence systolic blood pressure tend to fall as left atrial and left ventricular volumes decrease. This exaggerates the normal respiratory variation, and systemic pressure falls with inspiration to a level at which pulsus paradoxus, defined by convention as a greater than 10 mm Hg decrease in systolic pressure, is seen. In addition, decreased intrathoracic pressure has a disproportionate effect on the pulmonary venous circulation, which is not exposed to the high pericardial pressures; hence, a disproportionate fall during inspiration in the pulmonary vein to left atrial gradient further exacerbates the decrease in left atrial filling.7 The fall in systolic pressure is not in fact a paradox but rather an exaggeration of normal respiratory variation of approximately 3%8 with associated inspiratory decrease in left ventricular stroke volume. With severe tamponade, total elimination of pulse pressure can be seen with individual heartbeats, as in the example in Figure 24.4. In contrast with acute tamponade physiology, in which hemodynamic decompensation may occur after only a modest accumulation of fluid, generally in the range of 100 to 200 mL, chronic pericardial effusion results in a gradual increase in distensibility of the pericardium. With increasing compliance, large amounts of fluid can accumulate at low pressure without decreasing transmural pressure or compressing the cardiac chambers (see Fig. 24.1). Even in chronic low pressure–high volume tamponade, a limit of distensibility is eventually reached that results in similar pathophysiology as with acute tamponade, in some cases only after a liter or more of fluid has accumulated. Once the steep portion of the pressure-volume curve is reached, it is important to appreciate that with accumulation of another 50 to 100 mL of pericardial fluid, hemodynamic decompensation can occur rapidly, with similar outcomes as in patients who suffer from acute tamponade, such as is seen with penetrating trauma, coronary artery perforation, aortic dissection, or cardiac rupture. Pericardial effusions generally can be characterized as transudate or exudate, infectious or bloody, with tamponade occurring with variable frequency depending both on the rapidity of fluid accumulation and, to a somewhat lesser degree, on characteristics of the effusion and physiology determined by its etiology. Transudates are characteristic of congestive heart failure, radiation, and uremia; exudates are characteristic of infections, malignancy, and connective tissue disorders. Laboratory testing may help differentiate exudates from transudates; pericardial and serum protein, albumin, lactate dehydrogenase (LDH), cholesterol, and glucose should be obtained,9 although some of the differentiating characteristics applicable to pleural effusions may not be discriminatory in pericardial effusions.10 In addition, pericardial fluid total and differential cell count, Gram stain, aerobic and anaerobic culture, and mycobacterial and fungal evaluation should be performed along with cytology when malignancy is considered. Molecular techniques can be useful in diagnosing otherwise occult infections.11 Amylase is reserved for cases where pancreatic disease or esophageal rupture are part of the differential diagnosis. Conditions predisposing to slow accumulation such as heart failure, myxedema, chronic renal failure, and connective tissue disorders in general are less likely to cause acute tamponade, whereas those associated with rapid development, such as malignancy, infection (including bacterial, fungal, and human immunodeficiency virus related), or particularly hemorrhage, commonly result in abrupt hemodynamic deterioration. The effect of inflammation in decreasing compliance of the pericardium exacerbates the hemodynamic effects of effusions associated with pericarditis.12 The potential etiologic disorders are highly variable, with significant influence of demographics and geography, so that tamponade secondary to tuberculous pericardial effusion in immune-compromised patients is a not uncommon presentation in Africa,13 whereas in industrialized nations malignant effusions are a far more common cause.14 Large and usually benign pericardial effusions are seen frequently after heart transplantation, possibly immune mediated.15 Large pleural effusions can cause sufficient compression of the heart that tamponade physiology occurs.16 The most common etiologic disorders are listed in Table 24.1; more detailed discussion of the various causes is presented later in the chapter, organized by the hospital setting in which presentation typically is seen. Table 24.1 *Frequency of common etiologies of tamponade is based on 119 cases in Barcelona, Spain. Other relatively common causes of effusion include congestive heart failure, hypoalbuminemia, coagulopathy, and postcardiotomy and Dressler’s syndromes. Etiologies of tamponade will be dependent on geography and patient demographics and also will be strongly influenced by the presence of oncology, trauma, or dialysis units. For a comprehensive list of tamponade etiologies based on prior data, see Box 6.1. Data from Sagrista-Sauleda J, Merce J, Permanyer-Miralda G, et al: Clinical clues to the causes of large pericardial effusions. Am J Med 2000;109:95-101. Dyspnea is the most common symptom of tamponade, although its etiology sometimes is unexplained and it usually is not associated with significant concomitant pulmonary vascular congestion. It is likely to be secondary to decreased cardiac output and encroachment on lung volume by the expanding pericardium as well as any simultaneous pleural effusions. The patient may describe a sensation of fullness in the chest or abdomen and dysphagia, associated with venous engorgement and passive congestion, stretching of the richly innervated pericardium, and occasionally vagal stimulation.17 Because most patients with tamponade have comorbid conditions accounting for their effusion, additional signs and symptoms are likely to be related to pericarditis, malignancy, or other concomitant conditions. The hallmarks of cardiac tamponade on physical examination relate to features associated with venous hypertension, low cardiac output, and effects of the layer of fluid between the heart and the chest wall. In patients with tamponade, the general appearance changes substantially during progressive increase in pericardial pressure. Because tamponade represents a continuum, some patients with early tamponade physiology look well, whereas patients with more advanced tamponade show features of a low-output state, with clinical manifestations reflecting the high catecholamine levels required to maintain cardiac output. They become progressively more anxious and agitated and less communicative and may be struggling to breathe. Patients may complain of chest pain associated with pericardial irritation, not infrequently radiating to the neck, jaw, or shoulder18; if venous congestion is acute, patients may experience pain from stretching of Glissen’s capsule around the liver. The physical examination in significant tamponade can include Beck’s triad, described in 1935 by the surgeon C. S. Beck.19 This entity features jugular venous distention, decreased arterial pressure, and a small, quiet heart. As described earlier, pulsus paradoxus is the result of cardiac chamber interdependence and a decrease in left ventricular chamber volume with inspiration. It can be detected at the bedside by auscultation of Korotkoff sounds, identifying the highest and lowest pressures at which sounds are first heard during inspiration and expiration; alternatively, a simpler and more useful technique is to palpate the radial artery pulse with the cuff inflated to the maximum pressure at which the pulse appears and then to lower the cuff pressure in increments of 10 mm Hg to detect the pressure at which pulses are continuously noted throughout the respiratory cycle. In the patient whose systolic pressure is shown in Figure 24.4, simple palpation of the radial pulse would detect the loss of pulse pressure in the beat flagged by the red arrow. It is important to recognize that although pulsus paradoxus is a classic feature of severe tamponade, as a diagnostic feature it is of limited sensitivity and specificity. Various thresholds other than the relatively arbitrary 10 mm Hg threshold have been proposed to increase specificity, including a 10% decrease, rather than a 10 mm Hg fall.20 A drop in systolic pressure greater than 50% of the pulse pressure also has been proposed.1 Use of a 15 or 20 mm Hg fall in pressure by physical examination is a less sensitive but far more specific finding for tamponade but may result in delayed diagnosis. Pulsus paradoxus may be present in other conditions that result in an exaggerated decrease in systolic pressure with inspiration, such as massive pulmonary embolism, severe chronic obstructive pulmonary disease (which also can feature constrictive physiology because of limited expansion of the heart in the setting of hyperexpanded lungs),20 and right ventricular infarction.21 Furthermore, other features of the systemic blood pressure and pulse are important to consider. With a progressive decrease in cardiac filling overall, a decline in systemic pressure (regardless of phase of the respiratory cycle) as well as a decrease in pulse pressure (the difference between systolic and diastolic pressures) occurs, reflecting decreasing stroke volume and decreasing cardiac output. Thus, it may be impossible to palpate radial artery pulsations; with severe tamponade, the patient is likely to feel cool and clammy, a finding consistent with severe peripheral vasoconstriction. Tachycardia is almost invariable, except for comorbid conditions associated with a decrease in heart rate, such as electrical conduction disturbances, severe hypothyroidism, or aggressive β-blockade. Tachycardia is a compensatory mechanism for decreased stroke volume, is also caused by high catecholamine levels, and may result from pericardial irritation of the sinus node that stimulates a higher heart rate. On occasion, acute bradycardia may be seen in tamponade, sometimes the first finding after hemorrhage into the pericardial sac. Although a well-preserved systolic pressure and a wide pulse pressure are uncommon in tamponade, neither a low pressure nor a narrow pulse pressure is completely specific. Further, early in the course of tamponade, acute surge in catecholamine levels may result in hypertension rather than shock; in addition, patients with tamponade in the setting of renal disease and chronic hypertension appear to present more often with elevated systolic pressures.22 The pulsus paradoxus may be absent in conditions in which ventricular interdependence is masked23 (Box 24.1), such as a nonrestrictive atrial septal defect, in which inspiration also increases left atrial filling, or aortic insufficiency, in which left ventricular filling in diastole is increased by regurgitation from a high-pressure source: the aorta. Localized tamponade may have some general tamponade features (such as decreased stroke volume) but may not result in ventricular interdependence—hence, the clinical picture may be that of a sick patient with tamponade but without pulsus paradoxus. Markedly elevated left-sided heart diastolic pressures in severe left ventricular hypertrophy and other disease states may exceed the elevated right atrial and intrapericardial pressures in tamponade, decreasing the effect of inspiration on the interdependence of the right and left sides of the heart. An example in which both pulse pressure and pulsus paradoxus would be insensitive markers of tamponade is aortic dissection that combines aortic insufficiency with tamponade, in which a wide pulse pressure may be seen in some patients with partial compensation, and in which pulsus paradoxus, as discussed, may be masked. By contrast, conditions resulting in impaired right ventricular filling, such as right ventricular hypertrophy in severe pulmonary hypertension, also may result in the absence of a pulsus paradoxus24; furthermore, in settings such as cor pulmonale, the dramatic elevation in right-sided diastolic pressures will delay onset of the otherwise highly sensitive and early finding of right atrial and right ventricular diastolic collapse until tamponade is severe.25 A substantial number of case reports describe physiologic conditions in which the classic findings for tamponade are not seen or are attributable to other etiologic disorders.26 Because impairment of right-sided filling is usually the first manifestation of increasing pericardial pressure, high jugular venous pressure manifested by prominent venous pulsations may be the earliest finding on physical examination, occurring with increasing intrapericardial and right atrial pressures. Jugular venous distention may, however, be simultaneously absent because venoconstriction, a common finding with acute tamponade, makes detection of elevated venous pressures difficult. It also will be masked by low-volume tamponade, including volume-depleted states such as trauma, when, in addition to hemorrhage into the pericardium, significant blood loss has occurred. Other settings in which venous distention may not be observed are post-dialysis in patients with uremic pericardial effusions, and excessive diuresis, sometimes as part of treatment for symptoms of congestive heart failure when the cause of elevated filling pressures has not been appreciated.27
Cardiac Tamponade
Fundamentals of Tamponade
Pericardial Anatomy
Physiology
Pericardial Pressure
Etiology
History and Physical Examination
Pulsus Paradoxus
Venous Pressure
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Cardiac Tamponade