I. INTRODUCTION
Perioperative arrhythmias and conduction disturbances increase morbidity and mortality. New onset arrhythmias affect about 7% of patients following major noncardiothoracic surgery and up to 60% of post–cardiac-surgery patients. Atrial fibrillation (AF) is the most common postoperative arrhythmia.
In this chapter, we review the classification, etiology, and treatment of the arrhythmias most frequently encountered in critical care medicine.
II. CLASSIFICATION AND MANAGEMENT
A. The cardiac conduction system consists of three main parts: the sinus node, the atrioventricular (AV) node, and the His–Purkinje system.
B. There is not just one pacemaker system; instead, there are multiple mechanisms in cardiac pacing. Pathology of the sinus node and atrioventricular conduction system, as well as the right and left atrioventricular rings/right ventricular outflow tract, contribute to arrhythmias in the adult heart.
III. BRADYARRHYTHMIA
A. Pulseless Electrical Activity (PEA)
1. PEA is cardiac arrest with the presence of spontaneous organized cardiac electrical activity in the absence of adequate organ perfusion sufficient to maintain consciousness.
a. Management: Cardiopulmonary resuscitation (CPR) with uninterrupted chest compressions and standard pharmacological interventions provide the basis of the treatment. Primary management involves treating the underlining cause (significant hypoxia, profound acidosis, severe hypovolemia, tension pneumothorax, electrolyte imbalance, drug overdose, sepsis, large myocardial infarction, massive pulmonary embolism, cardiac tamponade, hypoglycemia, hypothermia, etc.). Extracorporeal life support with prolonged failure of return to spontaneous circulation should also be considered.
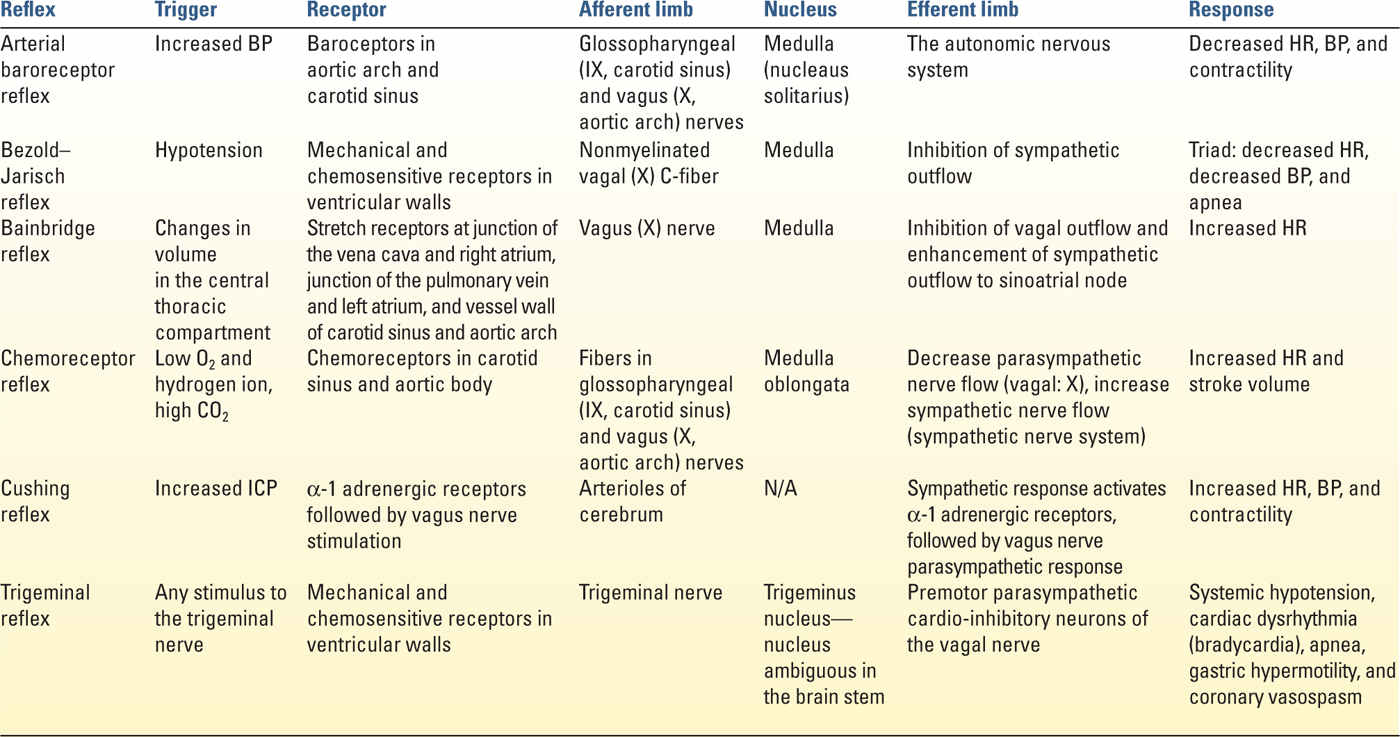
B. Abnormal Sympathetic Tone and the Cardiovascular Reflexes
Arrhythmias secondary to cardiovascular reflexes are commonly seen (Table 17.1).
C. Sinoatrial (SA) Node Abnormality
1. Sick sinus syndrome (SSS): SSS indicates bradyarrhythmias with or without tachyarrhythmias. More than 50 percent of patients with SSS develop tachy–brady syndrome with atrial fibrillation or flutter, leading to an increased risk of embolic stroke. The etiology includes intrinsic dysfunction of the SA node including degenerative fibrosis, an infiltrative process, or inherited dysfunction of ion channels within the SA node. Extrinsic conditions, that is, metabolic, infectious, autonomic, or pharmacologic conditions may also cause SSS (for a review, see Selected Readings).
a. Management: Chronic bradycardia may lead to ventricular electrical remodeling, and symptomatic SSS is a class I indication for a permanent pacemaker.
D. Conduction Delay and Bundle Branch Block (Congenital, Acquired)
1. Conduction delay: First degree A-V block is not an entirely benign condition. Instead, it may indicate worse clinical prognosis, especially among the elderly population. Second- and third-degree A-V block warrants pacemaker implantation.
a. Management: Cardiac pacing/resynchronization therapy for the patients with/without coexisting SSS, but the optimal pacing (as measured using the aortic flow time velocity integral measured on cardiac ultrasound) depends on intrinsic AV interval and desired pacing frequency.
2. Bundle branch block: Bundle branch block occurs secondary to a wide range of cardiac pathology. Compared with right bundle branch block (RBBB), left bundle branch block is considered to have high-diffuse disease, underlying ischemia, and dyssynchrony.
a. Management: Both RBBB and LBBB may benefit from biventricular pacing to restore synchrony of right/left ventricular contraction.
IV. TACHYRRHYTHMIAS
A. Sinus Tachycardia
1. The etiology may include sepsis, hypovolemia, cardiac ischemia/CHF, pain, and endocrine pathology (hyperthyroidism).
B. Atrial Fibrillation
1. Atrial fibrillation (AF) is characterized by a lack of organized P-wave activity and an irregularly irregular ventricular response on the ECG. AF is the most common arrhythmia requiring treatment, affecting around 5 million Americans, with the prevalence expected to double by 2050.
2. Atrial fibrillation is a complex molecular process. Atrial fibrillation may induce rapid atrial rates and promote increased sympathetic nerve activity, which augments β-adrenergic tone. This leads to an increase in protein kinase A–mediated hyperphosphorylation of atrial ryanodine receptors (RyR2). Increased RyR2 phosphorylation promotes sarcoplasmic reticulum calcium release that induces calcium-mediated inhibition of voltage-dependent L-type calcium currents. This leads to shortening of atrial myocyte action potential duration (ADP) and effective refractory periods (ERP). The electric remodeling promotes further AF and increased sympathetic nerve output, myocyte apoptosis, and fibrosis and promotes atrial dilatation and structural remodeling (reviewed by Wickramasinghe and Patel).
3. Management
a. Treatment of stable AF consists of pharmacologic intervention or overdrive pacing. Pharmacological treatment for hemodynamically stable AF includes class I and III medications (Table 17.2).
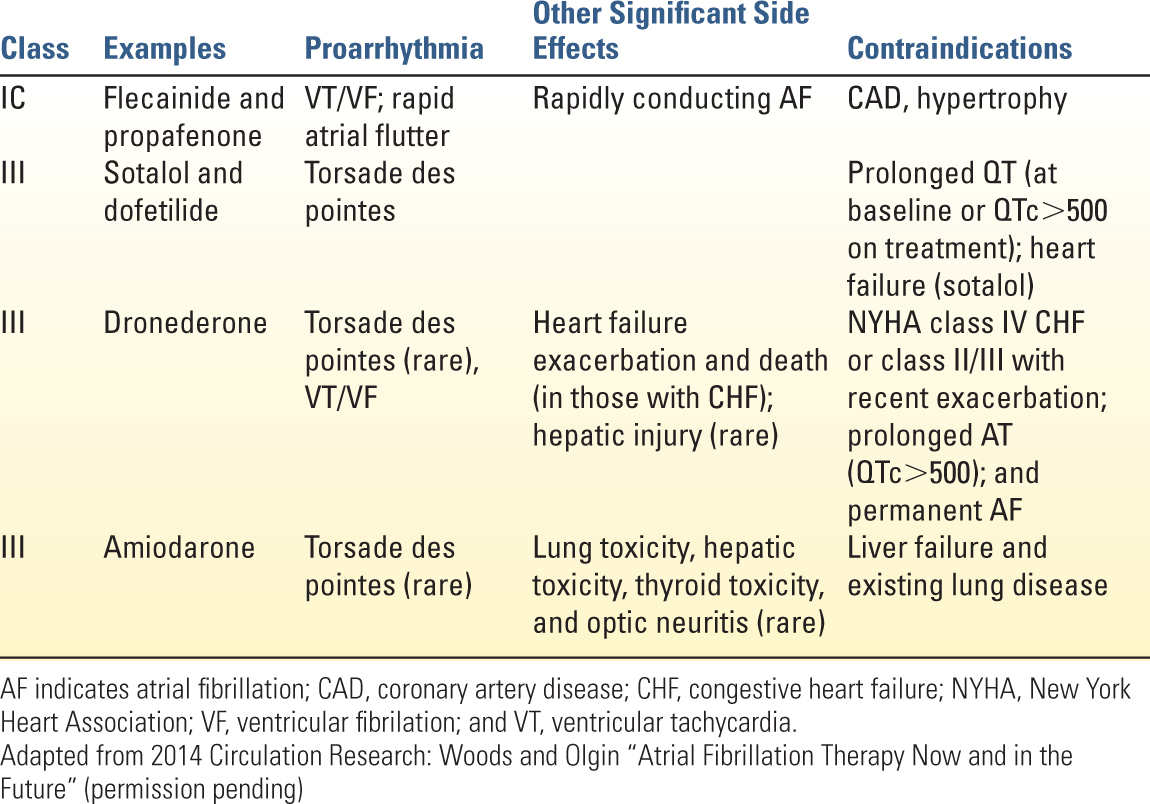
b. Unstable AF (altered mental status, hypotension of systolic <90 mmHg, chest pain, shortness of breath) warrants synchronized cardioversion. For maintaining sinus rhythm after cardioversion, several class IA, IC, and III drugs, as well as class II (β-blockers), are moderately effective in maintaining sinus rhythm after conversion of atrial fibrillation.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


