ERRORS, DEFECTS, AND MISTAKE-PROOFING
In manufacturing, the concept of quality includes the making of a product that performs as expected and has zero defects.1 This concept can be applied to the practice of medicine.2 A defect is a poor-quality result that cannot be undone. Examples of defects in the practice of regional anesthesia are wrong-sided block, wrong-medication injection, seizure due to undetected intravascular injection of local anesthetic, and total spinal anesthesia. Errors are precursors to defects. Examples of errors that might lead to the defects noted above include an incorrect consent form, a mislabeled drug, a needle entering the vascular system, or an epidural needle entering the subarachnoid space. It is critical to quality that errors are either prevented at the source from occurring or detected and corrected immediately before they become defects.1
Thus, three major strategies are used in manufacturing and medicine to prevent errors from becoming defects: physically making it impossible to create the error; checking at the source for error (also known as self-check); and checking for error just prior to the next step in a process (sequential check).1 Examples of these strategies in regional anesthesia include respectively removing a dangerous drug from the hospital formulary, reading the label of a syringe prior to injection, and watching carefully for a change in heart rate while injecting a local anesthetic that contains an epinephrine test dose during a block.
 SOURCE OF ERRORS
SOURCE OF ERRORS
Any human system has a built-in error rate due to the limitations of human performance. Errors include slips, lapses, and mistakes.3,4 A slip is when the action conducted is not what was intended. A lapse is a forgotten or missed action. A mistake is when the planned action was wrong.3 Since we are all human, there is a baseline rate of errors that will occur in any system we create. It is important for any system to not only recognize and accept this, but to build in checks to discover and correct these errors before they become defects.
The practice of regional anesthesia represents the interface of humans, knowledge, and technology. Technology includes the space, lighting, equipment, supplies, and drugs we use. Knowledge includes information about the patient’s history, medical condition, surgical objectives, and our knowledge of techniques and drugs. Traditional medical education focuses on the information and some of the technical aspects predominantly. However, recent efforts to improve safety have turned attention to the human conditions that compromise performance (Box 3-1).4–6 Human factors such as fatigue, interruptions, interpersonal conflict, and distractions have drawn significant attention and must be addressed and eliminated or reduced for best performance.4,7 The culture of medicine can create danger when a hierarchical environment creates fear of speaking up in members of the team.5,6,8 Everyone needs to feel free to ask a question for a clarification about the intention or potential safety issue. Leadership, openness, accountability, and intentional planning are required to change the culture.9,10
BOX 3-1 Sources of Errors in Regional Anesthesia Practice
 Human Factors: fatigue, interruptions, personal conflicts
Human Factors: fatigue, interruptions, personal conflicts
 Fear of speaking up: not identifying a defect for fear of being low on the hierarchy
Fear of speaking up: not identifying a defect for fear of being low on the hierarchy
 Variation: nonstandard approaches to patients undergoing the same operation or multiple versions of epidural anesthesia trays
Variation: nonstandard approaches to patients undergoing the same operation or multiple versions of epidural anesthesia trays
 Individual approaches to the same procedure: rather than a common approach based on guidelines, scientific evidence, or departmental consensus
Individual approaches to the same procedure: rather than a common approach based on guidelines, scientific evidence, or departmental consensus
Production pressure is pressure to perform care delivery in less time. It is present in the modern health care delivery system.11 Unfortunately, this “hurry-up” mentality results too often in cutting corners and speeding up tasks to the point where mistakes and safety risks occur. Later in this chapter, we address the appropriate response to production pressure.
 THE EFFECT OF VARIATION ON QUALITY AND SAFETY
THE EFFECT OF VARIATION ON QUALITY AND SAFETY
Process engineers in industry understand the devastating effect of variation on quality. Eliminating variation for the sake of creating a consistent product is one of the foundational principles of manufacturing.1,12,13 Thus, standards are created for parts and supplies to ensure performance within a predictable and acceptable range. Similarly, standard work is created for each job at the interface between product, machines, supplies, and humans.13 Specific job training was a foundational element that allowed women to take over jobs traditionally performed by men in the United States during World War II.14 Unfortunately, the lack of standard work in medicine has hampered our ability to provide a reliable product for our patients. The cry of “No Anesthesia by Cookbook” is a common phrase.15 However, physicians and nurses should understand that all our work is not the complex “organic” decision-making type.16 Some of our work is routine and easily subjected to standards that drive out variation and risk and improve quality. Large variation in the tools of regional anesthesia, for example, the number and types of needles to perform a single kind of block, results in variations in practice, unfamiliarity with equipment, difficulty in acquisition and stocking, and ultimately more risk of error or failure.
 EVIDENCE-BASED MEDICINE AND THE HUMAN CONDITION
EVIDENCE-BASED MEDICINE AND THE HUMAN CONDITION
Traditional medical training emphasizes the importance of evidence-based medicine. Physicians are expected to use evidence-based medicine in their practice. Still, the Institute of Medicine reported that it can take up to 15 to 20 years before proven practices become routine.17,18 Execution of well-accepted clinical guidelines remains a major challenge. Not following evidence-based guidelines has resulted in external regulatory bodies instituting public reporting and incentive payment strategies. Why is delivering evidence-based medicine so difficult? Is it because the studies are too complex? Or are we practitioners too busy to read? Is there just too much to know? Do we expect too much of ourselves to be able to read, assimilate, and create the pathways that will provide such care? Why is my memory failing me? The level of complexity and speed of modern health care creates a sense of challenge that can be fulfilling but too commonly results in burnout, despair, and self-doubt.19,20 Perhaps we are too self-reliant. Perhaps we expect too much of ourselves.
With this background, the rest of this chapter is devoted to practical examples of system design that will allow mistake-proofing regional anesthesia.
 THE THEMATIC SOLUTION: A CULTURE OF SAFETY WITH FOCUS ON THE PATIENT AND CONTINUOUS IMPROVEMENT
THE THEMATIC SOLUTION: A CULTURE OF SAFETY WITH FOCUS ON THE PATIENT AND CONTINUOUS IMPROVEMENT
The acceptance that we all are fallible and need help is present in a culture of safety. Teamwork and communication is maximized. The expectation that errors do and will occur is critical to fostering the requisite self-check and sequential check to detect errors. The culture of safety allows teammates to question and speak up when they sense or detect an error.4,21 Acquisition of appropriate knowledge of anatomy, pharmacology, techniques, and potential complications prior to applying this knowledge to patients is an appropriate goal. The learner is closely supervised and progressively advanced. Understanding the requisite repetitions to mastery is important in training.22 Dry laboratory and simulation scenarios can help train the novice and help prepare the expert for dealing with the unexpected or the extremely rare event.4,23 The workplace is studied scientifically with measures of cycle time, distances traveled, error rates, and defect rates, all of which in turn are systematically and repetitively improved.2 Patients, families, and providers are involved in the improvement of the workplace and the work flow. Continuous improvement allows successive approximations toward the ultimate goal of perfection.2,13 Carelessness is unacceptable. Avoidable complications should not occur. Knowing and meeting external regulatory requirements ensures corporate integrity and builds confidence in the team, the patients, and the public.
 THE WORKPLACE
THE WORKPLACE
The patient experience is foremost in mind, and their experience is actively managed.2,17 Patients come informed, know what to expect, and arrive on time. The environment is quiet, comforting, and supportive. Waiting is minimized.
Standardization of the workplace drugs and supply system eases the workflow (Box 3-2). A standardized cart with all the supplies needed for a block can be created so that it can be drawn to the bedside. The drawers are labeled and organized in a manner that allows learning where things belong and ease of routine access. The concept of “just-in-time” supply means that the practitioner has what he/she needs, when he/she needs it, in the amount he/she needs.13,24 If not, the waste of time in walking, searching, and returning will prolong the time it takes for the block and ultimately tire the provider toward the end of the day and frustrate the surgeon during the day.2 Accordingly, distances traveled for patients, providers, drugs, supplies, equipment, and information should be minimized as much as possible.2
BOX 3-2 Improving the Regional Anesthesia Workplace
 Optimize the human aspect of work: teamwork, communication, effective, and ongoing training
Optimize the human aspect of work: teamwork, communication, effective, and ongoing training
 Standardize the workplace: drugs, supplies
Standardize the workplace: drugs, supplies
 Optimize workflow: organize supplies, minimize travel distances, send for the patient based on a time predetermined to be adequate for block placement
Optimize workflow: organize supplies, minimize travel distances, send for the patient based on a time predetermined to be adequate for block placement
 Optimize visual systems: patient tracking, clear labeling of drugs and supply sources
Optimize visual systems: patient tracking, clear labeling of drugs and supply sources
 Develop, then periodically reevaluate clinical pathways
Develop, then periodically reevaluate clinical pathways
 Embrace checklists
Embrace checklists
 Optimize external setup—preoperative exams, patient consent, standard block trays
Optimize external setup—preoperative exams, patient consent, standard block trays
 Secure skilled assistance when performing the block
Secure skilled assistance when performing the block
 VISUAL SYSTEMS: REMOVING AMBIGUITY AND MISTAKES
VISUAL SYSTEMS: REMOVING AMBIGUITY AND MISTAKES
One only needs to visit a new environment to appreciate how much ambiguity there is in the activity going on around them. Visual system design is critical to signaling and removing ambiguity.2,13,24 Patient-tracking systems showing where they are in the process is critical to coordination of care and anticipating next steps. Medication errors due to look-alike bottles and labels have had catastrophic results. The safety improvement from clear to consistent labels is obvious. The Institute for Safe Medication Practice has recommended abandoning color-coded labels as practitioners can unintentionally reach for a “color” in a class of drugs and commit a syringe-swap error.25 Black printing on white labels leaves only one way to determine what drug and concentration is in the syringe: read the label. Sterile preprinted labels can be produced to allow consistent, efficient, and easy use every time. An example of sterile preprinted labels in a peel-pack for epidural block is included in Figure 3-1. A standard block tray setup can improve supply and drug recognition and the flow of a block (Fig. 3-2). Everyone should know the agreement about the layout. This can reduce mistakes and needle-stick injuries. The standard layout allows easy finding of supplies and drugs, should a learner need help from a more experienced practitioner.
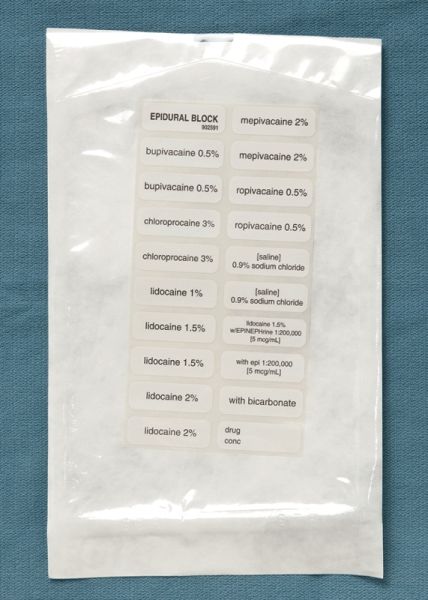
FIGURE 3-1. A preprinted label set in a sterile peel-pack that can be opened onto a sterile epidural block tray field. The labels allow quick labeling of all syringes and basins. Separate label sets for spinal block and peripheral nerve block can be created.



