Introduction
After cardiac arrest occurs, prompt and efficient action can be life saving. It is relatively rare for basic life support (BLS) interventions alone to restore a spontaneous circulation. Advanced life support (ALS) is the term used to describe a more extensive range of interventions, which includes advanced airway management, drugs, manual defibrillation, echocardiography, and identification and treatment of reversible causes of cardiac arrest. ALS interventions are usually provided by a team, for example an in-hospital resuscitation team or paramedic crew. Advanced life support algorithms facilitate team members working together in a structured and efficient manner enabling treatments to be given promptly without prolonged discussion.
ALS algorithm (Figure 5.1)
The first step in the ALS algorithm is to confirm cardiac arrest. The ALS provider is trained to check for breathing and feel for a pulse simultaneously. Cardiac arrest is confirmed by the absence of both a pulse and normal breathing; call the resuscitation team if not already present. Start high-quality, uninterrupted chest compressions and attach the patient to a defibrillator monitor with self-adhesive defibrillation/monitoring pads. Continue CPR by alternating 30 compressions with 2 ventilations until an advanced airway is inserted—this enables ventilation of the lungs without interrupting chest compressions. The underlying heart rhythm is assessed during a coordinated, short pause in CPR; once the rhythm is confirmed, CPR is restarted whilst the next phase of treatment is planned.
The ALS algorithm provides two main treatment arms defined by the underlying heart rhythm (Figure 5.1). The main difference between the treatment arms is the requirement for defibrillation. Heart rhythms requiring defibrillation (ventricular fibrillation (VF) (Figure 5.2) or pulseless ventricular tachycardiac (VT)) are managed using the shockable side of the algorithm. Other rhythms (pulseless electrical activity (PEA) and asystole) are treated according to the non-shockable side of the algorithm.
Figure 5.1 The adult Advanced Life Support Algorithm. Reproduced with the kind permission of the Resuscitation Council (UK).

Figure 5.2 Ventricular Fibrillation (VF). Copyright 2012 Dr Oliver Meyer, Reproduced with permission.

Shockable rhythms (Box 5.1)
Prolonged interruptions in chest compressions before and after a shock are associated with reduced survival. Defibrillation attempts should minimise the peri-shock pauses to no more than a few seconds (see Chapter 6). Attempted defibrillation should be a coordinated sequence of actions (Figure 5.3). Once a shockable rhythm has been identified, restart chest compressions promptly. Charge the defibrillator to the appropriate energy level during chest compressions (150–200 J biphasic for the first shock and 150–360 J biphasic for subsequent shocks). Once the defibrillator is charged, all but the person performing chest compressions should stand clear of the patient. There is uncertainty about the safety of delivering a shock during manual chest compression, so once other members of the team are clear, the person performing chest compressions stops compressions and stands clear while the shock is delivered. Do not delay defibrillation by attempting to re-confirm the underlying rhythm prior to shock delivery. Once the shock is delivered, immediately restart chest compressions. Continue CPR for a further 2 min before pausing to reassess the heart rhythm.
Figure 5.3 Defibrillation sequence. Plan actions; Pause CPR for rhythm analysis; Deliver shock; Restart CPR
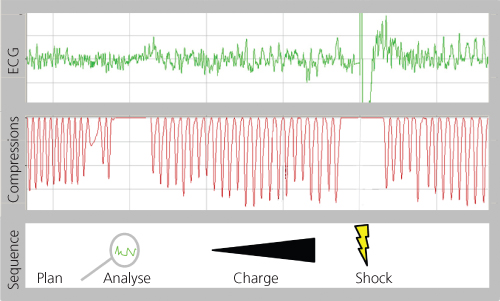
- Plan actions before pausing CPR
- Pause CPR briefly and check rhythm
- Restart CPR
- If VF/VT present, charge defibrillator
- Team stand clear
- Stop compressions and stand clear
- Deliver shock
- Immediately resume CPR
- Continue CPR for 2 min before reassessing rhythm
If a shockable rhythm persists, repeat the shock sequence. Increase the energy level as indicated by the defibrillator manufacturer’s instructions’. If a third shock is necessary, after shock delivery and restarting CPR, give adrenaline 1 mg and amiodarone 300 mg i.v. Further adrenaline 1 mg i.v may be given every 3–5 min thereafter (every other loop of the algorithm).
If during a rhythm check, organised electrical activity compatible with a cardiac output is seen, check for evidence of return of spontaneous circulation (ROSC). Signs of ROSC include a palpable pulse, spontaneous movements and/or a sudden increase in end-tidal carbon dioxide (ETCO2) on waveform capnography. If ROSC has occurred, start post-resuscitation care. If there are no signs of ROSC, or if asystole or an agonal heart rhythm is seen during the rhythm check, continue CPR and switch over to the non-shockable algorithm.
Non-shockable rhythms (Box 5.2)
The non-shockable rhythms are PEA (organised electrical activity in the absence of a palpable pulse) and asystole (the absence of electrical activity). Survival from cardiac arrest with PEA or asystole is dependent on identifying and treating promptly a potentially reversible cause of the arrest.
Treatment for non-shockable rhythms focuses on high-quality, uninterrupted chest compression and identification and treatment of potentially reversible causes of the arrest (Table 5.1). Adrenaline (1 mg) increases the rate of ROSC and should be given as soon as vascular access is available. Give further doses every 3–5 min (every other loop). Whether adrenaline improves long-term survival rates remains unknown.
Table 5.1 Potentially reversible causes of cardiac arrest and their treatment.
| Cause | Indicators/tests | Treatment |
| Hypoxia | History Arterial blood gas analysis | High flow oxygen Secure the airway |
| Hypovolaemia | History Signs of bleeding Echocardiography / ultrasound | Stop haemorrhage Fluid resuscitation |
| Hyperkaleamia and electrolyte disturbances | History Laboratory tests Arterial blood gas analysis 12 lead ECG | Specific treatment targeted at correcting the specific electrolyte disturbance |
| Hypothermia | History Measure temperature | Warm IV fluids Invasive re-warming with cardiopulmonary bypass |
| Tension pneumothorax | Clinical signs Ultrasound | Chest decompression (thoracostomy or needle) Chest drain |
| Tamponade | History (penetrating chest injury, post cardiac surgery) Echocardiography | Pericardiocentesis Thoracotomy |
| Toxin | History | Specific treatment targeted at toxin (e.g. naloxone for opioid) |
| Thrombosis | History Clinical signs e.g. DVT Echocardiography/ultrasound | CPR Thrombolytic therapy |









