Chapter 47
Ventilator Alarm Situations
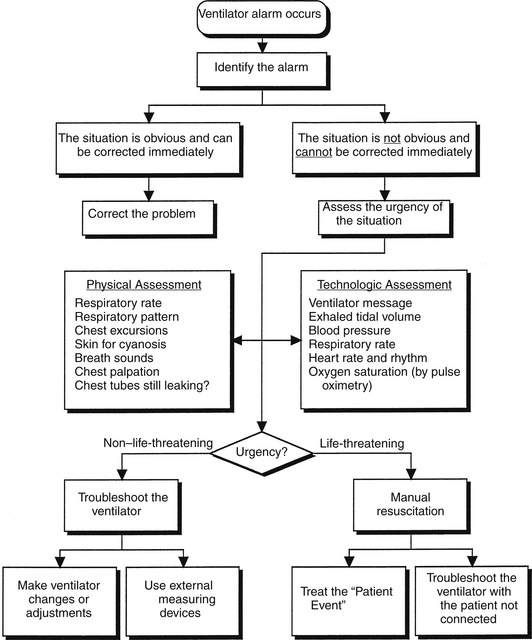
Contemporary microprocessor-based mechanical ventilators provide a wide selection of ventilatory modes that can customize assisted and spontaneous ventilation to individual patients (Chapter 2). These technologically advanced ventilators also incorporate a variety of alarms to alert intensive care unit (ICU) clinicians to numerous potentially dangerous situations. Ventilator alarms are designed to inform, but not dictate, the actions necessary to correct the potential hazard. For this reason, it is imperative that ICU clinicians be familiar with the function of the array of these alarms, how to evaluate ventilator alarm situations, and how to successfully manage those situations (Figure 47.1).
Types of Ventilator Alarms
The types and number of alarms that are functional on a ventilator vary depending on which ventilatory mode is being used. In addition, identical alarms may have different meanings and response times in different modes. Finally, alarms can signify different levels of clinical urgency (Table 47.1).
TABLE 47.1
Level of Urgency of Ventilator Alarms
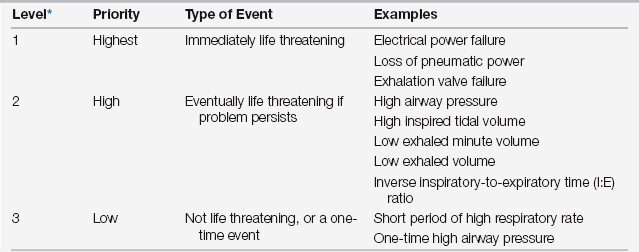
∗Level is indicated by tone, pitch, or volume of the audio alarm, or by information on the ventilator’s visual display, or both.
Patient-related event alarms are synonymous with “monitoring alarms.” They are designed to detect changes in the patient’s underlying physiologic condition. When a simple physiologic monitor alarm (e.g., an electrocardiographic [ECG] monitor) activates, the reason for the alarm arises from a patient-related event and not the functioning of the monitor itself. In contrast, a ventilator with its alarms serves not only as a physiologic monitor but also as a therapeutic intervention whose effects are continuously self-monitored. ICU clinicians often have difficulty recognizing when a problem arises from the patient or from the ventilator and distinguishing patient-ventilator interface problems from those solely attributable to the patient (patient-related events).
Each commonly used ventilator alarm is designed to detect a certain acute abnormality, as indicated by its name. Many alarms, however, overlap in the underlying conditions that they detect, as well as in the clinical consequences that they aim to prevent (Table 47.2). For example, if the patient becomes disconnected from the ventilator, multiple alarms activate. Early-response alarms monitor low inspiratory pressure, low exhaled tidal volume, and low positive end-expiratory pressure (PEEP) (if PEEP had been applied before the disconnection). Later alarms include low expired minute ventilation and apnea. Not only do these ventilator-associated alarms form a redundant safety net, but they also are complemented by nonventilator alarms, such as a pulse oximeter, or ECG lead monitoring. Tables 47.3 to 47.7 list conditions in which alarming is used frequently, with their differential diagnoses, categorized according to site of the problem, and matched with appropriate corrections.
TABLE 47.2
| Name of Alarm | Detects | Designed to Prevent |
| High inspiratory pressure limit | Acute increase in peak airway pressure | Barotrauma |
| Low inspiratory pressure | Large air leak | Delivery of inadequate tidal volume |
| Patient disconnection from ventilator circuit | Hypoventilation, hypoxemia | |
| Insufficient response by the ventilator to the patient’s inspiratory demand | Patient discomfort | |
| Excessive work of breathing | ||
| Low PEEP or CPAP pressure | Small leak in the system | Loss of end-expiratory pressure |
| Decrease in Pao2 | ||
| High end-expiratory pressure | Resistance to exhalation | Partial or complete obstruction of expiratory breathing circuit |
| Low exhaled tidal volume | Air leak | Insufficient ventilatory support |
| Low inspired tidal volume | Decrease in spontaneous tidal volumes | Hypoventilation |
| High exhaled tidal volume High inspired tidal volume Low respiratory rate Low exhaled minute ventilation | Improving lung compliance Increased inspiratory demand Oversedation Diminished respiratory drive Decrease in mechanical or spontaneous volumes | Volutrauma, barotrauma, alveolar hyperinflation, and ventilator-associated lung injury (VALI) Patient/ventilator asynchrony Apnea, hypercapnia Insufficient ventilatory support |
| Decreased lung compliance∗ | Hypoventilation | |
| Onset of respiratory muscle fatigue∗ | Respiratory compromise | |
| High exhaled minute ventilation | Increase in lung compliance∗ Excessive ventilation | Hyperventilation Dynamic hyperinflation† |
| Acute respiratory alkalosis | ||
| High respiratory rate | Respiratory distress, including anxiety, pain | Respiratory compromise Dynamic hyperinflation† |
| Self-cycling ventilator | Patient discomfort | |
| Onset of respiratory muscle fatigue | Hyperventilation Acute respiratory alkalosis | |
| Inverted inspiratory-to-expiratory ratio (I:E) | Self-cycling ventilatorInsufficient expiratory time | Hyperventilation Dynamic hyperinflation† |
| Inadvertent inspiratory pause | ||
| Apnea | Respiratory arrest | Hypoventilation with hypercapnia |
| Hypoxemia | ||
| Low oxygen-air inlet pressure | Disconnection of oxygen or compressed air source | Hypoxemia |
| Fall in oxygen or air pressure to less than minimal level | Insufficient pressure to power the ventilator’s pneumatic system | |
| Power disconnect | Electrical power failure Ventilator unplugged by mistake | Failure of all components of the ventilator that require electrical power to operate |
| Low or high Fio2 | A variance between the set Fio2 and the analyzed Fio2 | Hypoxemia Oxygen toxicity Misinformed clinical decisions based on incorrect Fio2 |
| Ventilator inoperative | Malfunction in the ventilator serious enough to be unsafe for patient use | All potentially harmful effects of the ventilator on the patient Insufficient ventilatory support |
PEEP, positive end-expiratory pressure; CPAP, continuous positive airway pressure.
∗Pertains to pressure control and pressure support modes of ventilation.
†Dynamic hyperinflation results in air trapping and auto-PEEP.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


