TOPICS
3. Implications of Ultrasound in Obstetric Anesthesia
7. Perioperative Cardiac Evaluation and Monitoring
8. Role in Obstetric Anesthesia
INTRODUCTION
Ultrasound has emerged as a valuable tool in anesthesia practice, “unblinding” many of what were once “blind” procedures. Because ultrasound is a radiation-free imaging tool, it has gained popularity for patient management in many areas of medicine. In anesthesia practice, it has become important for line placement1 and provides some distinct advantages in placement of regional anesthesia.2 The educational benefits of ultrasound imaging for teaching regional anesthesia have also been elucidated.3,4
In obstetric anesthesia, central neuraxial blockade analgesia is the most common anesthetic technique. The availability of ultrasound has naturally extended interest in this modality from peripheral nerve blocks to facilitating spinal/epidural techniques in obstetrics. Successful use of spinal ultrasound to aid in the placement of epidural and spinal injection in obstetric anesthesia was first reported in 1984.5 Recently, as ultrasound machines with higher quality images have become more affordable and more commonly available, their popularity has increased further.
Several studies conducted to assess the effectiveness of spinal ultrasound for epidural anesthesia have shown that an ultrasound-guided neuraxial approach can reduce the number of attempts and the procedure time while at the same time increasing the block success rate.6–8 These studies have provided a foundation for National Institute of Clinical Excellence (NICE) guidelines related to ultrasound imaging to facilitate instrumentation of the epidural space.9 The benefits of routine ultrasound imaging for intrathecal anesthetic placement are less clear.
ULTRASOUND TECHNOLOGY
Ultrasound imaging is based on high-frequency sound waves that are transmitted and received by a transducer (1-20 MHz). The transducer detects both the intensity of the echo and the time required to travel back to the source, which enables the calculation of the distance of the reflecting interface. Different layers of tissue produce a separate reflection of the ultrasound signal. At each interface, some of the wave is reflected back and detected by the transducer. The proportion of reflected to transmitted wave depends on acoustic impedance of tissues forming the interface. Bone reflects the majority of the energy, so few structures beyond bone can be visualized. Ultrasound examination of spine is challenging because the area of interest is deep and shielded by a complex, articulated cage of bones. For these reasons, images of the spinal structures are best observed with a low-frequency, curved ultrasound probe (2-5 MHz). Although higher frequency allows higher image resolution, the low frequency ultrasound beam provides deeper penetration, at the expense of image resolution.
Two acoustic windows are effective for lumbar spine sonographic assessment: one seen on the transverse approach and one seen on the longitudinal paramedian approach. The information from these two scanning planes complements each other.
IMPLICATIONS OF ULTRASOUND IN OBSTETRIC ANESTHESIA
Educational Implications
Ultrasound can be an important teaching tool in anesthesia. Sonographic visualization of anatomical structures can help improve understanding of spatial relationships and increase confidence in trainees, potentially reducing complications. In obstetric anesthesia, the learning curve for labor epidural placement has improved significantly with the advent of ultrasound imaging for teaching epidural anesthesia.3 Preprocedure ultrasound examination has reduced the number of attempts and failures10 for placing epidural catheters by anesthesiology trainees. It can be used as a preoperative assessment tool for predicting the feasibility/difficulty of neuraxial blockade.11,12 It appears that resident learning can be improved with the addition of ultrasound imaging.
Clinical Implications
• Neuraxial blockade
• Acute and chronic pain control
• Vascular access
• Cardiac evaluation
NEURAXIAL BLOCK
Ultrasonic assessment of the lumbar spine in assisting neuraxial anesthesia placement has become increasingly used in obstetric anesthesia. The efficacy and safety of ultrasound-guided neuraxial blocks in obstetrics have been evaluated by several studies.3,5–9 The conventional method used to perform neuraxial blocks is based on using palpation to identify bony landmarks. Pregnancy-associated weight gain and presacral edema can obscure anatomic landmarks and render palpation more complex and challenging. This can lead to an increase in the likelihood of block failure or complications, which can also be augmented with obesity, spine abnormalities, and prior back surgery. Ultrasound prepuncture scanning can provide information on the sonoanatomy of the lumbar spine. Studies have shown that the success rate of ultrasound-guided epidural insertions at first attempt was 30% to 60% greater when compared with the conventional epidural palpation technique.13 For intrathecal anesthetic placement, the benefits are less clear.
Advantages of Neuraxial Ultrasound
• More accurate location of midline
• Accurate determination of interspace level
• Suggestion of optimal needle puncture point and the angle of the puncture
• Estimation of depth of the epidural space
• Valuable teaching tool
• Increased in efficacy and decreased in duration of procedure
• May decrease the number of attempts and hence trauma
• Potential reduction in the number of unintentional dural punctures and other complications
• Useful in identifying atypical anatomy, including that associated with obesity, scoliosis, and previous spinal instrumentation
Ultrasound Examination of the Lumbar Spine
A systematic approach to ultrasound imaging of the spine has been described and builds on a detailed knowledge of lumbar spine anatomy. In 2008, The National Institute for Health and Clinical Excellence (NICE) issued guidelines for the use of lumber ultrasound imaging.9 Commonly used approaches to access the acoustical windows of lumbar spines are longitudinal paramedian and the transverse approaches. The pattern of images is described as the “saw sign” in the longitudinal paramedian approach (Figure 7-1) and “flying bat” in the transverse approach (Figure 7-2). In the “saw sign,” the teeth of the “saw” represent the articular processes and the spaces between the teeth represent the interspinous spaces, which consist of the ligamentum flavum/posterior longitudinal ligament and the vertebral body.14 Due to wider acoustic window in longitudinal approach, the ultrasonic images obtained in this plane are superior in quality compared with those obtained in the transverse plane, but the information obtained from each of these views complement each other.
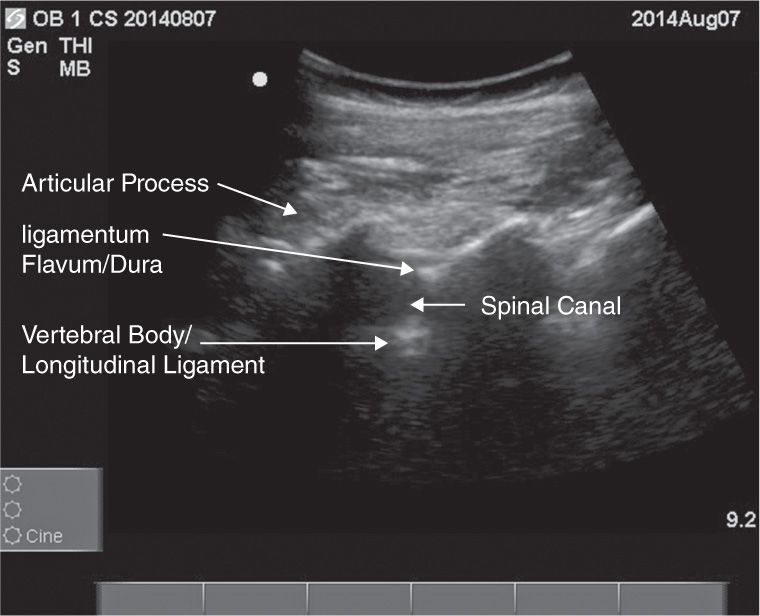
Figure 7-1. “Saw sign” in longitudinal paramedian approach.
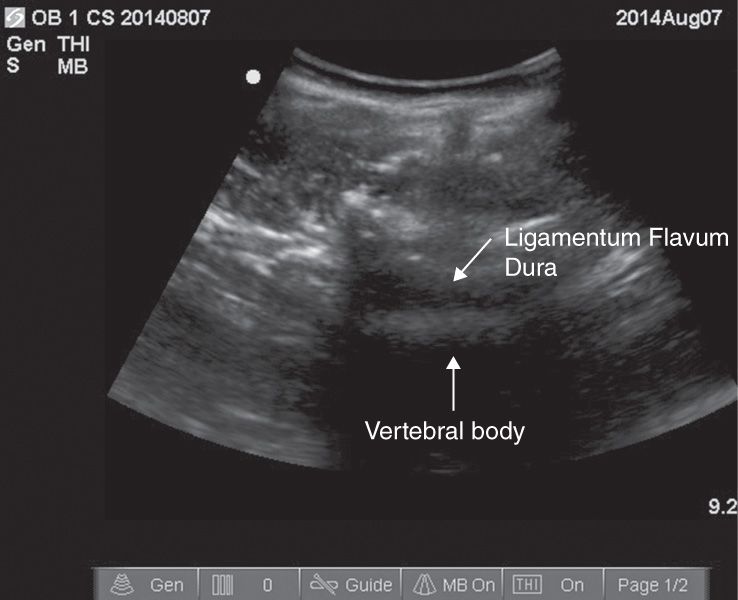
Figure 7-2. “Flying bat sign” in transverse approach.
SONOANATOMICAL LANDMARKS SEEN IN THE LONGITUDINAL PARAMEDIAN APPROACH
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


