Ultrasound-Guided Sciatic Block
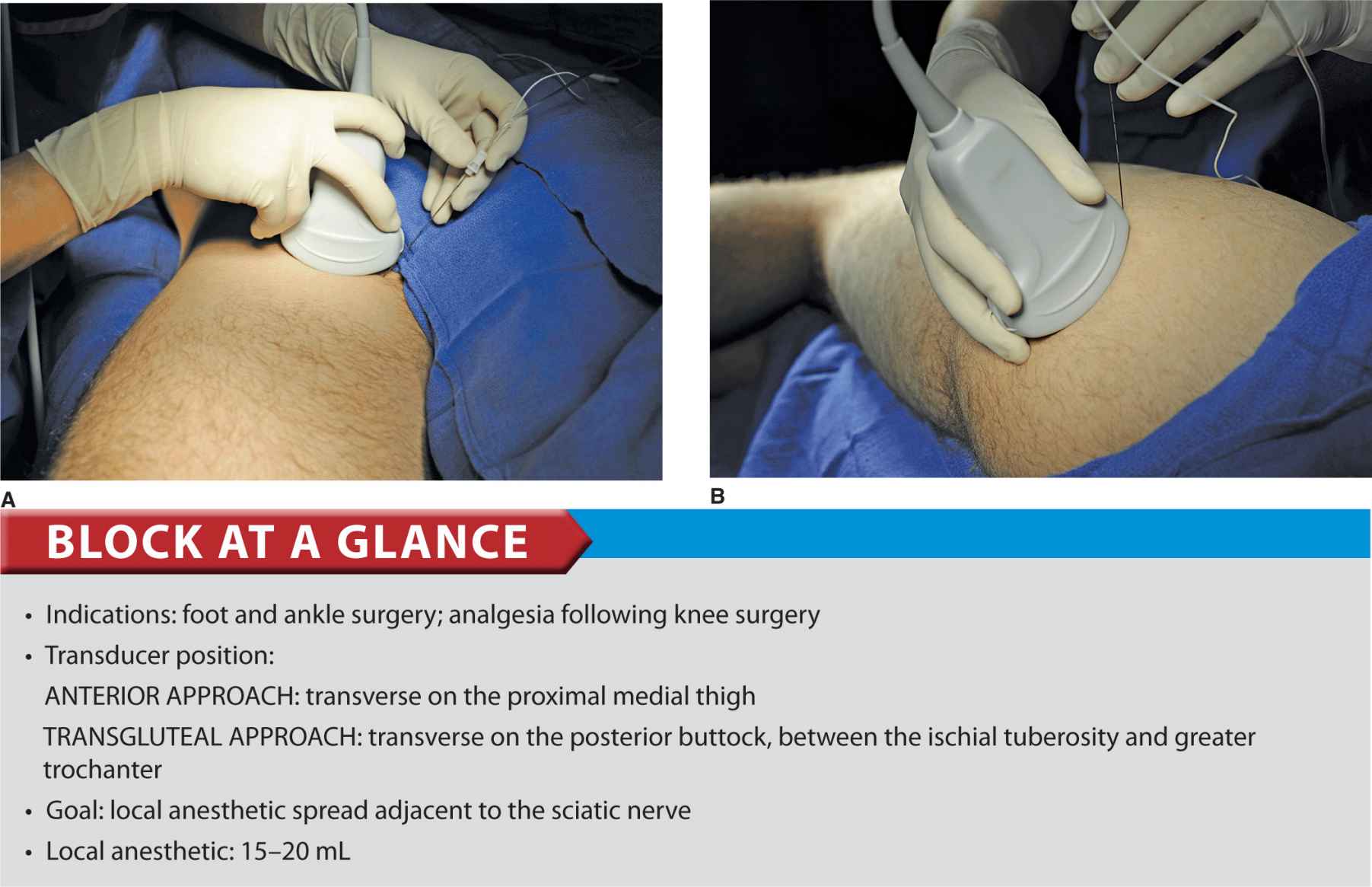
FIGURE 39.1-1. (A) Needle insertion to block the sciatic nerve using an anterior approach. Note that a curved (phased array) lower frequency transducer is used either in-plane (shown) or out-of-plane needle insertion can be used. (B) Transgluteal approach to sciatic block; patient position, transducer (curved) placement and needle insertion.
PART 1: ANTERIOR APPROACH
General Considerations
The anterior approach to sciatic block can be useful in patients who cannot be positioned in the lateral position due to pain, trauma, presence of external fixation devices interfering with positioning, and other issues. It also may be well-suited to patients who require postoperative blocks for analgesia following a total knee arthroplasty. Ultrasonography adds the benefit of no requirement for the palpation of a femoral pulse or the use of geometry for identification of the skin puncture point. In addition, using the ultrasound-guided approach should reduce the risk of puncture of the femoral artery as compared with the landmark-based approach. The actual scanning and needle insertion are performed on the anteromedial aspect of the proximal thigh, rather than the anterior surface, and may require a slight abduction and external rotation of the thigh. This block is not well suited to insertion of catheters because a large needle must traverse several muscles (causing pain and possibly hematomas), an awkward catheter location (medial thigh), and catheter insertion at approximately perpendicular angle to the sciatic nerve is difficult.
Ultrasound Anatomy
The sciatic nerve is imaged approximately at the level of the minor trochanter. At this location, a curved transducer placed over the anteromedial aspect of the thigh will reveal the musculature of all three fascial compartments of the thigh: anterior, medial, and posterior (Figures 39.1-2 and 39.1-3). Beneath the superficial sartorius muscle is the femoral artery, and deep and medial to this vessel is the profunda femoris artery. Both of these can be identified with color Doppler ultrasound for orientation. The femur is easily seen as a hyperechoic rim with the corresponding shadow beneath the vastus intermedius. Medial to the femur is the body of the adductor magnus muscle, separated by the fascial plane(s) of the hamstrings muscles. The sciatic nerve is visualized as a hyperechoic, slightly flattened oval structure sandwiched between these two muscle planes. The nerve is typically visualized at a depth of 6 to 8 cm (Figure 39.1-3).
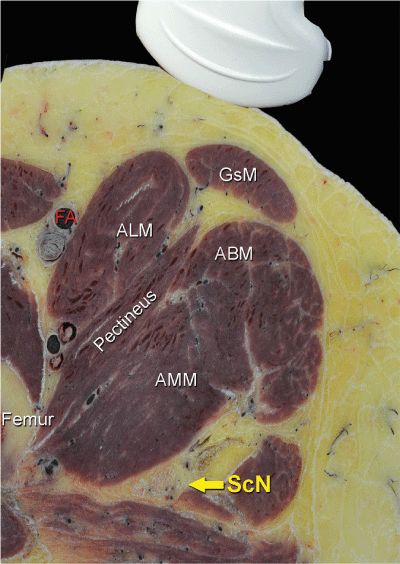
FIGURE 39.1-2. Cross- sectional anatomy of the sciatic nerve (ScN). Shown are femoral artery (FA), adductor longus muscle (ALM), pectineus muscle, adductor magnus muscle (AMM), adductor brevis muscle (ABM), gracilis muscle (GsM), and the femur. The sciatic nerve is seen posterior to the AMM.
FIGURE 39.1-3. Ultrasound anatomy of the sciatic nerve. From superficial to deep; femoral artery (FA) and femur laterally, adductor magnus muscle (AMM) and sciatic nerve (ScN) laterally. The sciatic nerve is typically located at a depth of 6 to 8 cm.
Distribution of Blockade
Sciatic nerve block results in anesthesia of the posterior aspect of the knee, hamstrings muscles, and entire lower limb below the knee, both motor and sensory, with the exception of skin on the medial leg and foot (saphenous nerve). The skin of the posterior aspect of the thigh is supplied by the posterior cutaneous nerve of the thigh, which has its origin from the sciatic nerve more proximal than the anterior approach. It is, therefore, not blocked by the anterior approach. Practically, however, the lack of anesthesia in its distribution is of little clinical consequence. For a more comprehensive review of the sciatic nerve distribution, see Chapter 1.
Equipment
Equipment needed is as follows:
• Ultrasound machine with curved (phased array) transducer (2–8 MHz), sterile sleeve, and gel
• Standard nerve block tray (described in the equipment section)
• One 20-mL syringe containing local anesthetic
• A 100-mm, 21 to 22 gauge short-bevel insulated stimulating needle
• Peripheral nerve stimulator
• Sterile gloves
Landmarks and Patient Positioning
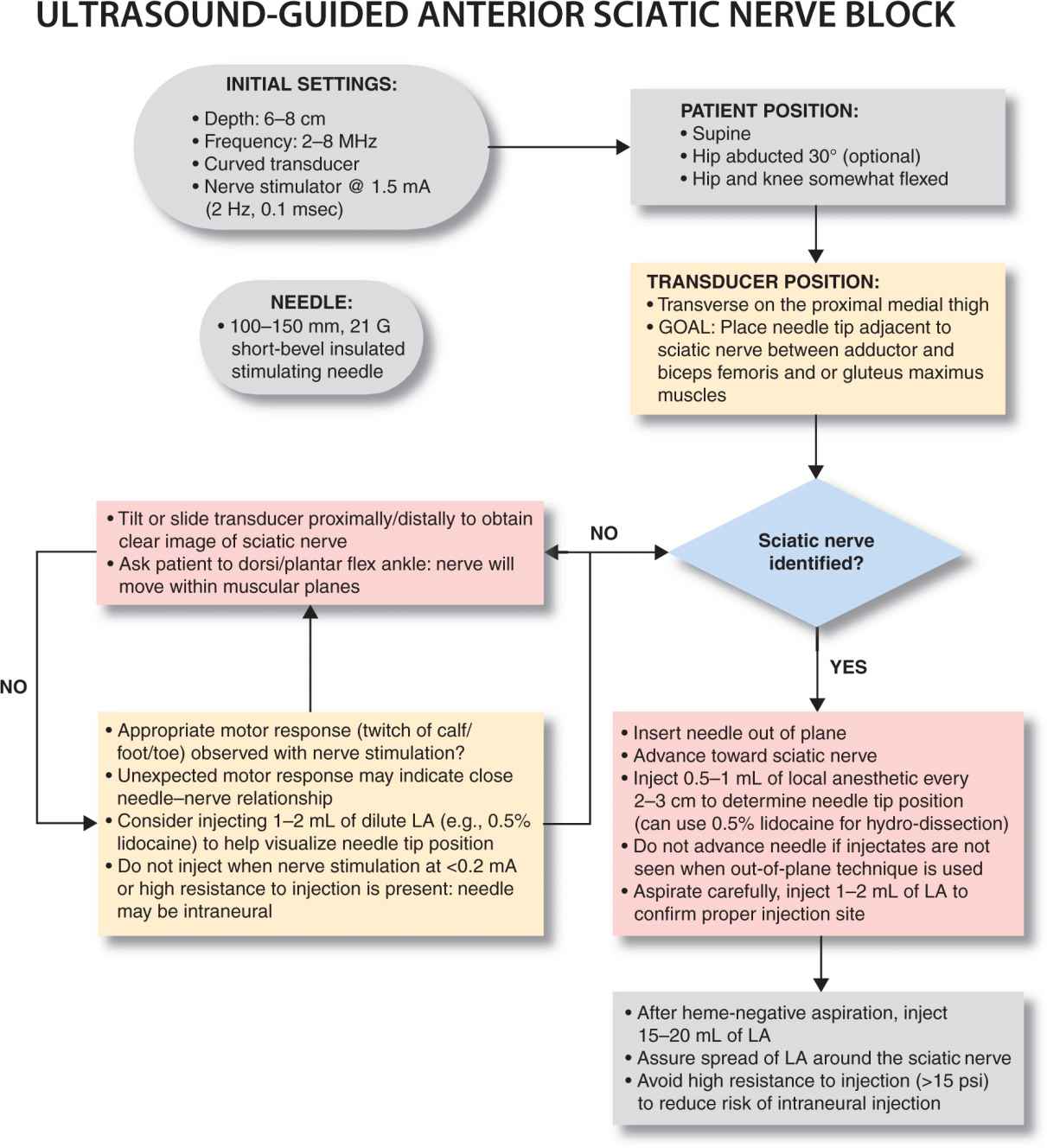
Anterior approach to sciatic nerve block is performed with the patient in the supine position. The hip is abducted to facilitate transducer and needle placement (Figure 39.1-4 and 39.1-5). When feasible, the hip and knee should be somewhat flexed to facilitate exposure. If nerve stimulation is to be used at the same time (recommended), exposure of the calf and foot are required to observe motor responses. In either case, it is useful to expose the entire thigh to appreciate the distance from the groin to knee.

FIGURE 39.1-4. Transducer position to visualize the sciatic nerve through the anterior approach.
FIGURE 39.1-5. A simulated needle path using an out of plane technique to reach the sciatic nerve (ScN) through the anterior approach.
Technique
With the patient in the proper position, the skin is disinfected and the transducer positioned so as to identify the sciatic nerve. If the nerve is not immediately apparent, sliding and tilting the transducer proximally or distally can be useful to improve the contrast and bring the nerve “out” of the background from the musculature. Finally, if the patient is able to dorsiflex and/or plantar flex the ankle, this maneuver often causes the nerve to rotate or otherwise move within the muscular planes, facilitating identification. Once identified, the needle is inserted in-plane or out of plane (more common in our program) from the medial aspect of the thigh and advanced toward the sciatic nerve (Figure 39.1-5). If nerve stimulation is used (1.0 mA, 0.1 msec), the contact of the needle tip with the sciatic nerve is usually associated with a motor response of the calf or foot. Once the needle tip is deemed to be in the proper position, 1 to 2 mL of local anesthetic is injected to confirm the adequate distribution of injectate. Such injection helps delineate the sciatic nerve within its intramuscular tunnel, but it may displace the sciatic nerve away from the needle. Improper spread of the local anesthetic or nerve displacement may require an additional advancement of the needle. When injection of the local anesthetic does not appear to result in a spread around the sciatic nerve, additional needle repositions and injections are necessary.
In an adult patient, 15 to 20 mL of local anesthetic is usually adequate for successful blockade (Figure 39.1-6). Although a single injection of such volume of local anesthetic suffices, it may be beneficial to inject two to three smaller aliquots at different locations to assure the spread of the local anesthetic solution around the sciatic nerve. The block dynamics and perioperative management are similar to those described in the nerve stimulator technique section, Chapter 19.
FIGURE 39.1-6. Simulated needle path using an out-of-plane technique with local anesthetic ![]() and proper distribution of local anesthetic to anesthetize the sciatic nerve (ScN).
and proper distribution of local anesthetic to anesthetize the sciatic nerve (ScN).
SUGGESTED READING
Abbas S, Brull R. Ultrasound-guided sciatic nerve block: description of a new approach at the subgluteal space. Br J Anaesth. 2007;99:445-446.
Barrington MJ, Lai SL, Briggs CA, Ivanusic JJ, Gledhill SR. Ultrasound-guided midthigh sciatic nerve block-a clinical and anatomical study. Reg Anesth Pain Med. 2008;33:369-376.
Bruhn J, Moayeri N, Groen GJ, et al. Soft tissue landmark for ultrasound identification of the sciatic nerve in the infragluteal region: the tendon of the long head of the biceps femoris muscle. Acta Anaesthesiol Scand. 2009; 53: 921-5
Bruhn J, Van Geffen GJ, Gielen MJ, Scheffer GJ. Visualization of the course of the sciatic nerve in adult volunteers by ultrasonography. Acta Anaesthesiol Scand. 2008;52:1298-1302.
Chan VW, Nova H, Abbas S, McCartney CJ, Perlas A, Xu DQ. Ultrasound examination and localization of the sciatic nerve: a volunteer study. Anesthesiology. 2006;104:309-314.
Chantzi C, Saranteas T, Zogogiannis J, Alevizou N, Dimitriou V. Ultrasound examination of the sciatic nerve at the anterior thigh in obese patients. Acta Anaesthesiol Scand. 2007;51:132.
Danelli G, Ghisi D, Fanelli A, et al. The effects of ultrasound guidance and neurostimulation on the minimum effective anesthetic volume of mepivacaine 1.5% required to block the sciatic nerve using the subgluteal approach. Anesth Analg. 2009;109:1674-1678.
Danelli G, Ghisi D, Ortu A. Ultrasound and regional anesthesia technique: are there really ultrasound guidance technical limits in sciatic nerve blocks? Reg Anesth Pain Med. 2008;33:281-282.
Domingo-Triado V, Selfa S, Martinez F, et al. Ultrasound guidance for lateral midfemoral sciatic nerve block: a prospective, comparative, randomized study. Anesth Analg. 2007;104:1270-1274.
Fredrickson MJ, Kilfoyle DH. Neurological complication analysis of 1000 ultrasound guided peripheral nerve blocks for elective orthopaedic surgery: a prospective study. Anaesthesia. 2009;64:836-844.
Gnaho A, Eyrieux S, Gentili M. Cardiac arrest during an ultrasound-guided sciatic nerve block combined with nerve stimulation. Reg Anesth Pain Med. 2009;34:278.
Gray AT, Collins AB, Schafhalter-Zoppoth I. Sciatic nerve block in a child: a sonographic approach. Anesth Analg. 2003;97:1300-1302.
Hamilton PD, Pearce CJ, Pinney SJ, Calder JD. Sciatic nerve blockade: a survey of orthopaedic foot and ankle specialists in North America and the United Kingdom. Foot Ankle Int. 2009;30:1196-1201.
Karmakar MK, Kwok WH, Ho AM, Tsang K, Chui PT, Gin T. Ultrasound-guided sciatic nerve block: description of a new approach at the subgluteal space. Br J Anaesth. 2007;98:390-395.
Latzke D, Marhofer P, Zeitlinger M, et al. Minimal local anaesthetic volumes for sciatic nerve block: evaluation of ED 99 in volunteers. Br J Anaesth. 2010;104:239-244.
Marhofer P, Harrop-Griffiths W, Willschke H, Kirchmair L. Fifteen years of ultrasound guidance in regional anaesthesia: Part 2-recent developments in block techniques. Br J Anaesth. 2010;104:673-683.
Murray JM, Derbyshire S, Shields MO. Lower limb blocks. Anaesthesia. 2010;65(Suppl 1):57-66.
Oberndorfer U, Marhofer P, Bosenberg A, et al. Ultrasonographic guidance for sciatic and femoral nerve blocks in children. Br J Anaesth. 2007;98:797-801.
Ota J, Sakura S, Hara K, Saito Y. Ultrasound-guided anterior approach to sciatic nerve block: a comparison with the posterior approach. Anesth Analg. 2009;108:660-665.
Pham Dang C, Gourand D. Ultrasound imaging of the sciatic nerve in the lateral midfemoral approach. Reg Anesth Pain Med. 2009;34:281-282.
Salinas FV. Ultrasound and review of evidence for lower extremity peripheral nerve blocks. Reg Anesth Pain Med. 2010;35:S16-25.
Saranteas T. Limitations in ultrasound imaging techniques in anesthesia: obesity and muscle atrophy? Anesth Analg. 2009;109:993-994.
Saranteas T, Chantzi C, Paraskeuopoulos T, et al. Imaging in anesthesia: the role of 4 MHz to 7 MHz sector array ultrasound probe in the identification of the sciatic nerve at different anatomic locations. Reg Anesth Pain Med. 2007;32:537-538.
Saranteas T, Chantzi C, Zogogiannis J, et al. Lateral sciatic nerve examination and localization at the mid-femoral level: an imaging study with ultrasound. Acta Anaesthesiol Scand. 2007;51:387-388.
Saranteas T, Kostopanagiotou G, Paraskeuopoulos T, Vamvasakis E, Chantzi C, Anagnostopoulou S. Ultrasound examination of the sciatic nerve at two different locations in the lateral thigh: a new approach of identification validated by anatomic preparation. Acta Anaesthesiol Scand. 2007;51:780-781.
Sites BD, Neal JM, Chan V. Ultrasound in regional anesthesia: where should the “focus” be set? Reg Anesth Pain Med. 2009;34:531-533.
Tran de QH, Munoz L, Russo G, Finlayson RJ. Ultrasonography and stimulating perineural catheters for nerve blocks: a review of the evidence. Can J Anaesth. 2008;55:447-457.
Tsui BC, Dillane D, Pillay J, Ramji AK, Walji AH. Cadaveric ultrasound imaging for training in ultrasound-guided peripheral nerve blocks: lower extremity. Can J Anaesth. 2007;54:475-480.
Tsui BC, Finucane BT. The importance of ultrasound landmarks: a “traceback” approach using the popliteal blood vessels for identification of the sciatic nerve. Reg Anesth Pain Med. 2006;31:481-482.
Tsui BC, Ozelsel TJ. Ultrasound-guided anterior sciatic nerve block using a longitudinal approach: “expanding the view.” Reg Anesth Pain Med. 2008;33:275-276.
van Geffen GJ, Bruhn J, Gielen M. Ultrasound-guided continuous sciatic nerve blocks in two children with venous malformations in the lower limb. Can J Anaesth. 2007;54:952-953.
van Geffen GJ, Gielen M. Ultrasound-guided subgluteal sciatic nerve blocks with stimulating catheters in children: a descriptive study. Anesth Analg. 2006;103:328-333.
PART 2: TRANSGLUTEAL AND SUBGLUTEAL APPROACH
General Considerations
The use of ultrasonographic guidance greatly expanded the options that practitioners have for accomplishing the block of the sciatic nerve because the nerve can be imaged at several convenient levels. With the transgluteal approach, the needle is inserted just distal deep to the gluteus maximus muscle to reach the sciatic nerve. The sciatic nerve at the gluteal crease is readily identified in a predictable anatomic arrangement, between two osseous landmarks (ischial tuberosity and the greater trochanter) and beneath a well-defined muscle plane. The use of ultrasound visualization decreases the need for the geometry and measurements that are required for the classic landmark-based approaches. With the subgluteal approach, the nerve simply reached a few centimeters distally, just below the level of the subgluteal crease where imaging is not interfered by the bones. The preference of one approach over the other is made based on the patient’s anatomic characteristics and personal preference.
Ultrasound Anatomy
At this transgluteal level, the sciatic nerve is visualized in the short axis between the two hyperechoic bony prominences of the ischial tuberosity and the greater trochanter of the femur (Figure 39.2-1 and 39.2-2). The gluteus maximus muscle is seen as the most superficial muscular layer bridging the two osseous structures, typically several centimeters thick. The sciatic nerve is located immediately deep to the gluteus muscles, superficial to the quadratus femoris muscle. Often, it is slightly closer to the ischial tuberosity (medial) aspect than the greater trochanter (lateral). At this location in the thigh, it is seen as an oval or roughly triangular hyperechoic structure. At the subgluteal level, however, the sciatic nerve is positioned deep to the long head of the biceps muscle and the posterior surface of the adductor magnus.
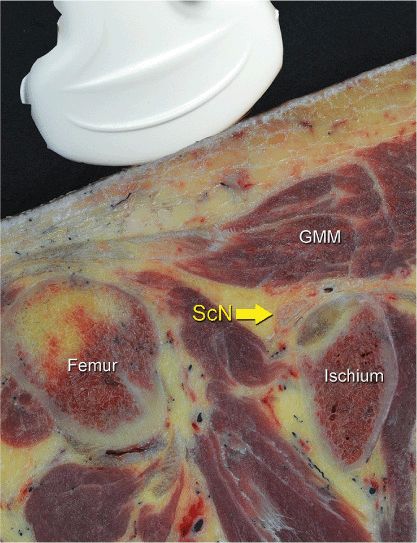
FIGURE 39.2-1. Transsectional anatomy of the sciatic nerve at the transgluteal level. Sciatic nerve (ScN) is seen between the greater trochanter of the femur and the ischium tuberosity, just below the gluteus maximus (GMM) muscle.
FIGURE 39.2-2. An ultrasound image demonstrating the sonoanatomy of the sciatic nerve (ScN). The ScN often assumes an ovoid or triangular shape and it is positioned underneath the gluteus muscle (GMM) between the ischium tuberosity (IT) and femur.
Distribution of Blockade
Sciatic nerve block results in anesthesia of the entire lower limb below the knee, both motor and sensory blockade, with the exception of a variable strip of skin on the medial leg and foot, which is the territory of the saphenous nerve, a branch of the femoral nerve. In addition, both the transgluteal and subgluteal approaches provide motor blockade of the hamstring muscles. The skin of the posterior aspect of the thigh however, is supplied by the posterior cutaneous nerve of the thigh, which has its origin from the sciatic nerve more proximal than the subgluteal approach. It is, therefore, unreliably anesthetized with subgluteal block; however, it is of relatively little clinical importance. For a more comprehensive review of the sciatic nerve distribution, see Chapter 1, Essential Regional Anesthesia Anatomy.
Equipment
Equipment needed is as follows:
• Ultrasound machine with curved (phase array) transducer (2–8 MHz), sterile sleeve, and gel
• Standard nerve block tray (described in the equipment section)
• One 20-mL syringe containing local anesthetic
• A 100-mm, 21 to 22-gauge short-bevel insulated stimulating needle
• Peripheral nerve stimulator
• Sterile gloves
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


