Stroke
Edward C. Jauch
Todd J. Crocco
Health care providers, hospitals, and communities must develop stroke systems to increase the efficiency and effectiveness of stroke care. Emergency medical services (EMS) use is strongly associated with decreased time to initial physician assessment, computed tomography (CT) imaging for stroke, and neurologic evaluation. Once a patient with probable stroke is identified, EMS personnel should transport the patient to the nearest, most appropriate facility. Prearrival notification of the facility is key, decreasing time to examination by a physician, CT imaging, and reperfusion therapy. An ambulance may bypass a hospital that does not have the resources or the institutional commitment to treat patients with a stroke if a more appropriate hospital, preferably a stroke center, is available within a reasonable transport interval.
Minimizing disability from stroke starting with dispatch
Priority transport to an appropriate facility for stroke care
Identification of patients with ischemic stroke for reperfusion therapy
Update of 2007 AHA/ASA ischemic stroke guidelines
Key Points from AHA ASA 2007 Ischemic Stroke Update
EMS activation and transport result in faster hospital arrival and decreased emergency department (ED) evaluation time.
EMS dispatchers can identify 50% of patients with stroke.
Public education programs result in sustained identification and treatment of stroke patients.
Designation of primary stroke centers for emergency stroke care is strongly recommended.
Patients should be transported to the nearest stroke center for evaluation and care if a stroke center is located within a reasonable transport distance and transport time.
Introduction
Each year in the United States over 780,000 people suffer a new or repeat stroke. On average a new stroke occurs every 40 seconds. More than 180,000 of these people will die, making stroke the third leading cause of death in the United States.1 Many advances have been made in stroke prevention, treatment, and rehabilitation.2,3 For example, fibrinolytic therapy can limit the extent of neurologic damage from stroke and improve outcome, but the time available for treatment is limited.3,4
Stroke Facts1
On average, someone in the United States has a stroke every 40 seconds.
On average, someone dies of a stroke every 3 to 4 minutes.
Each year over 780,000 people experience a new or recurrent stroke. About 600,000 of these are first strokes and 180,000 are recurrent strokes.
Men’s stroke incidence rates are greater than women’s at younger ages but not at older ages. Each year approximately 60,000 more women than men have a stroke.
Blacks have almost twice the risk of first-ever stroke compared with whites.
Silent strokes are a common occurrence, increasing in prevalence from 11% for ages 55 to 64 and 43% over age 85.
Approximately 15% of strokes are heralded by transient ischemic attacks (TIAs).
Health care providers, hospitals, and communities must develop systems to increase the efficiency and effectiveness of stroke care. The seven “Ds” of stroke care—detection, dispatch, delivery, door (arrival and urgent triage in the ED), data, decision, and drug administration—highlight the major steps in diagnosis and treatment and the key points at which delays can occur.5,6
This chapter summarizes the management of acute stroke in the adult patient, including out-of-hospital care through the first hours of treatment; this early management focuses on the rapid identification of acute ischemic stroke while allowing evaluation for reperfusion therapy. Highlights from and updates of the 2007 ischemic stroke guidelines are included. For additional information about the management of acute ischemic stroke and these guidelines, see the American Heart Association (AHA)/American Stroke Association (ASA) guidelines for the early management of adults with ischemic stroke.7,8
AHA/ASA Guidelines Update
Activation of the 911 system is strongly supported because it speeds treatment of stroke.
Educational programs to increase public awareness are encouraged because they increase the number of patients evaluated and treated for stroke.
Brief EMS assessment and transport of potential stroke patients to the closest facility providing emergency stroke care are recommended (class I).
Although reperfusion therapy in patients using tissue plasminogen activator (tPA) is presented in the context of early identification and management, other reperfusion methods may be available for selected patients in specialized stroke centers. These include intra-arterial administration of a fibrinolytic agent in carefully selected patients,9,10,11,12,13 angioplasty and stenting,14 mechanical clot distruption,15 and clot extraction.16
The Stroke Chain of Survival
The AHA and ASA have developed a community-oriented “stroke chain of survival” that links specific actions to be taken by patients and family members with recommended actions by out-of-hospital health care responders, ED personnel, and in-hospital specialty services (Fig. 36-1):
Rapid recognition and reaction to stroke warning signs
Rapid start of prehospital care
Rapid EMS transport and hospital prenotification
Rapid diagnosis and treatment in hospital
The 7 D’s of Stroke Survival
In ST-segment elevation myocardial infarction (STEMI), time is muscle. When acute ischemic stroke occurs, time is brain, so the reperfusion concept was expanded to include not only patients with acute coronary syndromes (STEMI) but also highly selected stroke patients.5 Hazinski was the first to describe an analogous series of linked actions to guide advanced cardiac life support (ACLS) stroke care.17 Borrowing from the “door-to-drug” theme of the National Heart Attack Alert Program for fibrinolytic treatment of STEMI,18 the seven “Ds” of ACLS stroke care begin each step with the letter D: detection, dispatch, delivery, door, data, decision, and drug. Table 36-1 lists the seven steps of stroke care plus the major actions in each step. At each step, care must be organized and efficient in order to avoid needless delays.
 Figure 36-1 • The stroke chain of survival. |
Table 36-1 • The 7 “D’s” of Stroke Care in the Reperfusion Era | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Definitions
Acute ischemic stroke (AIS), refers to an abrupt or rapidly developing neurologic impairment lasting >24 hours that is attributable to a focal vascular cause and results in an interruption of the blood supply to a region of the brain. The sudden onset of focal brain dysfunction is the hallmark of stroke.19 Experts and clinicians most often classify strokes as either hemorrhagic or ischemic. Hemorrhagic stroke occurs when a blood vessel within the brain ruptures. Ischemic stroke occurs when a blood vessel becomes blocked, typically by plaque and/or clot, interrupting flow to a region of the brain. If blood flow is interrupted long enough, irreversible infarction of brain tissue often ensues. Although the causes of stroke are numerous, the distinction between ischemic and hemorrhagic types is important, since therapy differs significantly based on stroke type (Fig. 36-2).
Ischemic Stroke
Definition and Categories of Ischemic Stroke
In an ischemic stroke (87% of all strokes1), interruption in the blood supply is caused by occlusion of an artery to a region of the brain. Ischemic strokes can be defined on the basis of etiology and duration of symptoms. With the more widespread use of modern brain imaging, many patients with symptoms lasting ≤24 hours are found to have an infarction. The most recent definition of stroke for clinical trials has required either symptoms lasting >24 hours or imaging of an acute, clinically relevant brain lesion in patients with rapidly vanishing symptoms.
Ischemic stroke is classified into categories based upon the presumed mechanism of stroke and the type and localization of the vascular lesion.20 Strokes are generally subdivided into the following categories:20
Thrombotic stroke (large artery atherosclerotic stroke): An acute thrombus that occludes an artery is superimposed on chronic arterial narrowing, acutely altered endothelial lining, or both. This pathophysiology parallels that for acute coronary syndromes (ACS), where a ruptured or eroded plaque is the proximate cause of most episodes of ACS. The artery may be extracranial or intracranial.
Embolic stroke: Intravascular material, most often a blood clot, separates from a proximal source and flows through an artery until it occludes a distal site. Many of these events are cardioembolic—originating from the heart—in patients with atrial fibrillation, valvular heart disease, acute MI, or rarely endocarditi
Cardiogenic cerebral embolism is responsible for about 20% of ischemic strokes. There is a history of nonvalvular atrial fibrillation (AF) in about half of these patients, valvular heart disease in one fourth, and left ventricular (LV) thrombus in almost one third.21
Other causes: These include small-vessel disease and other causes such as sickle cell disease, hypercoagulable states, and arterial dissection, resulting in a more global pattern of brain infarction. This is typically due to periods of significant systemic hypotension and inadequate cerebral perfusion that cannot support the metabolic demands of the brain tissue. Hypoperfusion stroke often occurs in patients who recover cardiac function after sudden cardiac arrest.
Undetermined
 Figure 36-2 • Type of stroke. Some 87% of strokes are ischemic and potentially eligible for fibrinolytic therapy if patients otherwise qualify; 13% of strokes are hemorrhagic, and the majority of these are intracerebral. Men have 1.25 times the number of strokes as women, and blacks have almost twice the risk of first-ever stroke compared with whites.11 |
Transient Ischemic Attack
By conventional clinical definitions, if the neurologic symptoms continue for 24 hours, a person is diagnosed with stroke; otherwise a focal neurologic deficit lasting ≤24 hours is defined as a TIA. However, approximately one third of all TIAs would be classified as stroke based on diffusion-weighted magnetic resonance imaging,22 and new diagnostic techniques have shown that up to 60% of patients with a TIA have definite radiographic evidence of brain infarction.23 A proposed new definition of TIA is a “brief episode of neurologic dysfunction caused by a focal disturbance of brain or retinal ischemia, with clinical symptoms typically lasting <1 hour, and without evidence of infarction.”24
The distinction between TIA and ischemic stroke has become less important in recent years because many of the preventive approaches are applicable to both groups. TIA and stroke share pathogenetic mechanisms; prognosis may vary, depending on their severity and cause; and definitions are dependent on the timing and degree of the diagnostic evaluation.
TIAs, however, are an important determinant of stroke, with 90-day risks of stroke reported as high as 10.5% and the greatest stroke risk apparent in the first week.25,26 Risk scores have been developed and validated to allow risk stratification of patients with TIA, including duration of symptoms.25,27,28,29
Classification by Vascular Supply
Strokes are also classified by vascular supply and anatomic location:
Anterior circulation (carotid artery territory) stroke: Stroke that results from occlusion of branches of the carotid artery. Such strokes usually involve the cerebral hemispheres.
Posterior circulation (vertebrobasilar artery territory) stroke: Stroke that follows occlusion of branches of the vertebral or basilar arteries. These strokes usually involve the brainstem or cerebellum.
Hemorrhagic Stroke
Hemorrhagic strokes (13% of all strokes) occur when a blood vessel in the brain suddenly ruptures, with hemorrhage into the surrounding tissue. Damage typically results from direct trauma to brain cells; expanding hematoma effects leading to elevated intracranial pressure; release of damaging neurotoxic mediators; local vascular spasm; and loss of blood supply to brain tissue downstream from the ruptured vessel.
There are two types of hemorrhagic stroke, based on the location of the arterial rupture:30
Intracerebral hemorrhagic stroke (10%): Occurs when blood ruptures directly into the brain parenchyma, usually from small intracerebral arterioles pathologically altered by chronic hypertension.
Hypertension is the most common cause of intracerebral hemorrhage.31
Among the elderly, amyloid angiopathy appears to play a major role in intracerebral hemorrhage.
Subarachnoid hemorrhagic stroke (3%): Occurs when blood leaks from a cerebral vessel into the subarachnoid space. If the rupture occurs in a cerebral artery, the blood is released at systemic arterial pressure, causing sudden, painful, and dramatic neurologic symptoms.
Aneurysms cause most subarachnoid hemorrhages.
Arteriovenous malformations cause approximately 5% of subarachnoid hemorrhages.
Pathophysiology
Concept of the Evolving “Ruptured Plaque”
The “ruptured plaque” pathophysiologic concept of ACS is also applicable to many ischemic strokes (see Chapter 1, Figures 1-1 and 1-5).32,33,34 An ulcerated ruptured plaque is the key mechanism of most thrombotic and embolic strokes in patients without valvular heart disease or atrial fibrillation. In thrombotic stroke, complete occlusion typically develops at an atherosclerotic plaque.35,36 In embolic stroke, the developing thrombus breaks off and floats downstream, ultimately lodging in and obstructing a smaller arterial vessel. A thrombotically active carotid plaque associated with high inflammatory infiltrate was observed in about 75% of patients with ipsilateral major stroke. In addition, ruptured plaques of these patients affected by stroke were characterized by the presence of a more severe inflammatory infiltrate—comprising monocytes, macrophages, and T lymphocytes—compared with those observed in the TIA and asymptomatic groups.37 Ruptured plaques may occur not only in the intracranial branches of the carotid and vertebrobasilar arteries but also in the extracranial portions of the carotid arteries and in the aorta.
Vessel occlusion results from the interaction between blood vessels, activated coagulation components of blood, inflammatory cells, and chemical mediators of inflammation. The pathology of recently symptomatic carotid plaques is similar to that of culprit coronary plaques, with strong correlations between macrophage infiltration and plaque instability.34
The most common cause of acute ischemic stroke is atherosclerosis of the carotid or vertebrobasilar artery.
Varying degrees of inflammation in vulnerable atherosclerotic plaques predispose these arteries to endothelial erosion, plaque rupture, and platelet activation as well as aggregation.
The ensuing development of a thrombus—composed of platelets, fibrin, and other elements of coagulation—can completely occlude an artery already narrowed by atherosclerosis. This occlusion of blood flow first leads to ischemia and ultimately to infarction of downstream brain tissue, producing a thrombotic stroke.
The thrombus, either before or immediately after it becomes completely occlusive, may dislodge and travel to more distal cerebral arteries, producing an embolic stroke (Fig. 36-3).
 Figure 36-3 • Occlusion in a artery due to cerebral embolism at the arterial bifurcation. A. Area of infarction surrounding immediate site and distal portion of brain tissue after occlusion. B. Area of ischemic penumbra [ischemic but not yet infarcted (dead) brain tissue] surrounding areas of infarction. This ischemic penumbra tissue is alive but dysfunctional because of altered membrane potentials. The dysfunction is potentially reversible. Current stroke treatment attempts to keep the area of permanent brain infarction as small as possible by preventing the areas of reversible brain ischemia in the penumbra from transforming into larger areas of irreversible brain infarction. [Reprinted with permission of Genentech, Inc, from the Internet Stroke Center (www.strokecenter.org). Copyright Genentech, Inc.] |
Postocclusion Dynamics
Downstream from the thrombotic or embolic obstruction, brain cells begin to die and necrosis occurs. With persistent occlusion, an area of irreversible brain damage (infarction or necrosis) develops.
Surrounding the central area of necrosis or infarction is an area of ischemia called the ischemic penumbra.
“Time Is Brain”
The recently coined term “brain attack” and the phrase “time is brain” convey the sense of urgency in stroke care. Once restriction of blood flow occurs as a result of occlusion, an ever-increasing amount of brain tissue becomes irreversibly injured over time. There is only a limited amount of time available to recognize and treat reversible brain ischemia.41,42,43
Other Pathophysiologic Processes
Atrial Fibrillation
Atrial fibrillation remains the most frequent cause of cardioembolic stroke.44
The noncontracting walls of the fibrillating left atrium and left atrial appendage serve as both a stimulus and a reservoir for small emboli.
Hypertension
Hypertension causes a thickening of the walls of small cerebral arteries, leading to reduced flow and a predisposition to thrombosis.
Lacunar infarcts exemplify the type of thrombotic stroke caused by chronic hypertension. They are thought to result from occlusion of a small perforating artery to the subcortical areas of the brain.
The major cerebrovascular burden imposed by chronic hypertension is hemorrhagic stroke.
Stroke Risk Factors
Risk factors can be identified in most stroke patients.48 Primary and secondary stroke prevention requires identification of a patient’s risk factors, followed by elimination, control, or treatment of as many factors as possible:
Elimination (e.g., smoking)
Control (e.g., hypertension, diabetes mellitus)
Treatment (e.g., antiplatelet therapy, carotid endarterectomy when indicated)
Table 36-2 lists the major modifiable stroke risk factors.
Table 36-2 • Stroke Risk: Factors That Can Be Modified | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
Physical Activity Reduces the Risk of Stroke
A meta-analysis of reports of 31 observational studies conducted mainly in the United States and Europe found that moderate and high levels of leisure-time and occupational physical activity protected against total stroke, hemorrhagic stroke, and ischemic stroke.23
Stroke Management
Stroke treatment begins with the recognition of the symptoms of stroke. An important component in this initial step is education—of the patient, family, community, 911 dispatcher, prehospital care provider, and health care provider. Once recognition of potential stroke symptoms occurs, management involves expeditious transfer of the patient to an appropriate facility for further assessment and care. Stroke centers are important because they focus on the integration of multidisciplinary care helping ensure appropriate hemodynamic management, optimal glucose control, prevention of aspiration, and rehabilitation. Figure 36-4 is the suspected stroke algorithm, which identifies treatment goals for these patients.
Signs and Symptoms of Ischemic Stroke
The warning signs of an ischemic stroke or TIA may be varied, subtle, and transient, but they represent a potentially life-threatening neurologic illness (Fig. 36-4, Box 1). Like the symptoms of an ACS, symptoms of ischemic stroke can be misinterpreted and denied by patients. Emergency health care providers should recognize the importance of these symptoms and respond quickly with effective interventions in stroke management. The signs and symptoms of a stroke may be subtle and include:
Sudden numbness or weakness of the face, arm, or leg, especially on one side of the body
Sudden confusion, trouble speaking or understanding speech
Sudden trouble seeing in one or both eyes
Sudden trouble walking, dizziness, loss of balance or coordination
Sudden severe headache with no known cause
Out-of-Hospital Management: The Important Role of the Community EMS System in Stroke Care (Fig. 36-4, Box 2)
Three of the four links in the stroke chain of survival and the first three of the seven Ds of stroke care (detection, dispatch, and delivery) require effective operation of the EMS system. For this reason the 2005 AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care and the 2007 AHA/ASA guidelines for the early management of adults with ischemic stroke strongly emphasize the important role of these personnel and services.8 Recent data show that 29% to 65% of patients with signs and symptoms of stroke contact local EMS, but only 14% to 32% of them arrive within 2 hours of symptom onset.52,53 EMS use is strongly associated with decreased time to initial physician assessment, computed tomography (CT) imaging for stroke, and neurologic evaluation.54,55
Time to Stroke Treatment
EMS use is strongly associated with decreased time to
Initial physician assessment
CT imaging for stroke
Neurologic evaluation
[check mark] Detection: Early Recognition of Stroke Signs and Symptoms
Early treatment of stroke depends on the patient, family members, or other bystanders recognizing the event. Patients often ignore the initial signs and symptoms of a stroke and delay access to care for several hours after the onset of symptoms. Because of these time delays, many patients with ischemic stroke may not benefit from time-dependent therapies such as intravenous fibrinolytic treatment, which must be started within 3 hours of symptom onset.
In one study of 100 stroke patients, only 8% had received information about the signs of stroke, yet nearly half had previously had a prior TIA or stroke.48 Unlike many acute myocardial infarctions in which chest pain can be a dramatic and unrelenting symptom, a stroke may have a subtle presentation with only mild facial paralysis or speech difficulty. Mild signs or symptoms may go unnoticed or be denied by the patient or bystander. Strokes that occur while the patient is asleep or when he or she is alone further hamper prompt recognition and action.
[check mark] Dispatch: Call 911 and Priority EMS Dispatch
Stroke patients and their families must understand the need to call 911 and activate the EMS system as soon as they suspect stroke signs or symptoms. The EMS system provides the safest and most efficient method for transporting the patient to the hospital.56
EMS Assessments and Actions
EMS assessments and actions for patients with suspected stroke include the following steps:
Rapid identification of patients with signs and symptoms of acute stroke (through the performance of a prehospital stroke assessment tool)
Support of vital functions
Prearrival notification of the receiving facility
Rapid transport of the patient to the most appropriate receiving facility (often a primary stroke center)
Whenever possible, EMS should bring a witness with the patient to the receiving facility.
Emergency medical dispatchers play a critical role in the timely treatment of potential stroke patients. Data show that dispatchers correctly identify stroke symptoms on the basis
of just the initial phone description in more than half of all stroke cases.52,57 Dispatchers can triage emergencies over the telephone and prioritize calls to ensure a rapid response by the EMS system. Specific dispatch educational efforts about stroke are encouraged, and stroke dispatch should be given a priority, like that for acute myocardial infarction and trauma.
of just the initial phone description in more than half of all stroke cases.52,57 Dispatchers can triage emergencies over the telephone and prioritize calls to ensure a rapid response by the EMS system. Specific dispatch educational efforts about stroke are encouraged, and stroke dispatch should be given a priority, like that for acute myocardial infarction and trauma.
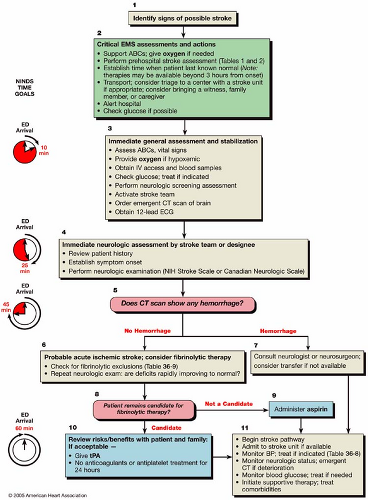 Figure 36-4 • Algorithm for suspected stroke. |
Table 36-3 • Key Components of a Focused Stroke Patient History | |||
|---|---|---|---|
| |||
[check mark] Delivery: Prompt Transport and Prearrival Notification to Hospital
Leaders in EMS and emergency medicine must develop training programs and patient care protocols to guide the actions of prehospital care providers. After the basic life support (BLS) primary and ACLS secondary surveys and appropriate actions have been performed for airway, breathing, and circulation, EMS providers should immediately obtain a focused history and patient assessment (Table 36-3).
A key component of the patient’s history is the time of symptom onset or when the patient was last known to be normal. The history must include this information. The provider may need to obtain this and other details of the patient’s history from family or the appropriate bystander. Preferably this person should be transported with the patient. Prehospital providers can help establish the precise time of stroke onset or the last time the patient was noted to be neurologically normal. This time point is viewed as “time zero,” a starting point that is critical for time-dependent treatments.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


