Circulatory Adjuncts to Improve Coronary Perfusion Pressure
Karl B. Kern
Standard cardiopulmonary resuscitation (CPR) alone often fails to produce enough coronary perfusion pressure for successful resuscitation. The difficulty of achieving optimal coronary perfusion pressure and the early onset of rescuer fatigue with standard manual CPR has been a strong motivation for the development of numerous circulatory adjuncts in hope of achieving greater coronary perfusion pressures.
Rescuer fatigue and implications for successful resuscitation outcome
Circulatory adjuncts and CPR alternatives as methods and strategies to optimize coronary perfusion pressure (CPP) during prolonged CPR
Any interruption in effective chest compression decreases the chance for survival; pauses and interruptions in chest compressions should be minimized, e.g., time for defibrillation, rhythm, and pulse checks.
Improving Coronary Perfusion Pressure: Use of Circulatory Adjuncts
CPP correlates with myocardial blood flow and myocardial blood flow correlates with resuscitation success; hence the greater the CPP, the more likely a successful outcome. However, standard CPR alone often fails to produce enough CPP for successful resuscitation. Increasing the force of manual chest compressions to produce greater CPP is not without potential problems (Fig. 10-1). The use of excessive force in chest compressions may result in severe and even life-threatening injury. In an animal model (without coronary lesions) of cardiac arrest, a myocardial perfusion pressure of 30 mm Hg appears to be ideal for ensuring long-term survival without a high degree of CPR injury. More forceful chest compressions to increase perfusion pressure above 30 mm Hg resulted in CPR-induced trauma and a reduced rate of 24-hour survival.1 In this series, animals that died from CPR-induced injury had a mean perfusion pressure of 39 mm Hg, whereas those that survived for 24 hours had a mean perfusion pressure of 29 mm Hg. These results suggest that CPP measured during CPR may not only be useful as a guide to predict successful defibrillation and return of spontaneous circulation but can also be used to avoid unnecessary injury when optimal levels have already been achieved.
Although effective or good CPR is associated with a better outcome, the ability to perform such CPR appears to be time-dependent, i.e., the longer CPR is performed, the less likely it is that compressions will remain effective in terms of sternal displacement or rate per minute. This phenomenon has been demonstrated in a number of CPR manikins, where recordings of the chest compression rate and depth are obtained.2,3,4,5 A study by Ochoa et al. perhaps demonstrates this time effect most dramatically.3 These authors evaluated the influence of rescuer fatigue on the quality of chest compressions and the influence of gender, age, weight, and height on the reduction of quality CPR. Thirty-eight health care professionals performed chest compressions on a recording manikin for 5 consecutive minutes. A marked decline in depth of sternal displacement was observed as early as the second minute of the trial, and the mean time to fatigue, as verbalized by the participants, was just over 3 minutes.
The difficulty of achieving optimal CPP and the early onset of rescuer fatigue with standard manual CPR has been a strong motivation for the development of numerous circulatory adjuncts in the hope of achieving greater CPPs and thereby improved outcome with resuscitation efforts.
Interposed Abdominal Compression CPR
Interposed abdominal compression CPR (IAC-CPR) is a method of manual basic life support where abdominal
pressure is applied over the midabdomen (midway between the xiphoid process and the umbilicus) with two hands from a second rescuer during the relaxation phase of chest compressions (Fig. 10-2). Investigators at Purdue University reported the hemodynamic advantages of intermittent abdominal compression during CPR.6 Follow-up studies at Purdue verified improvement in CPP with the use of interposed abdominal compression CPR.7 Two other reports examined the use of this form of CPR in experimental models, one of which did not find improvement8 and one of which did.9 Three clinical reports have been published concerning the use of IAC-CPR in human subjects where coronary perfusion was measured. One patient reportedly had an increase in CPP.10 In a separate series, 6 patients had no significant increase11 and, in the largest series of 14 patients, IAC had inconsistent effects on the CPP.12 Despite these hemodynamic inconsistencies, four clinical trials13 comparing IAC-CPR and standard CPR demonstrated greater rates of initial successful resuscitation and a trend toward an increased survival rate to hospital discharge in the IAC-CPR group, including two in-hospital randomized trials.14,15 The first found statistically greater rates of return of spontaneous circulation (ROSC), 24-hour survival, and survival to discharge in 48 of 103 patients randomized to IAC-CPR compared with standard CPR.14 The other trial (from the same investigators and institution) found significantly more ROSC and 24-hour survival with IAC-CPR compared with standard CPR in patients with initial rhythms of asystole or pulseless electrical activity during their in-hospital cardiac arrests.15 Pooled data from these two separate randomized trials showed a 24-hour survival benefit for IAC-CPR (33% vs. 13%). One pediatric case report16 described intra-abdominal trauma, but none of the adult trials have found an increased incidence of CPR-induced trauma. Per the recommendations from International Liaison Committee on Resuscitation (ILCOR), IAC-CPR may be considered for in-hospital resuscitations when sufficient trained personnel are available (class IIb), but there is no convincing evidence that it is superior for out-of-hospital resuscitation; it is therefore not recommended for in that setting.
pressure is applied over the midabdomen (midway between the xiphoid process and the umbilicus) with two hands from a second rescuer during the relaxation phase of chest compressions (Fig. 10-2). Investigators at Purdue University reported the hemodynamic advantages of intermittent abdominal compression during CPR.6 Follow-up studies at Purdue verified improvement in CPP with the use of interposed abdominal compression CPR.7 Two other reports examined the use of this form of CPR in experimental models, one of which did not find improvement8 and one of which did.9 Three clinical reports have been published concerning the use of IAC-CPR in human subjects where coronary perfusion was measured. One patient reportedly had an increase in CPP.10 In a separate series, 6 patients had no significant increase11 and, in the largest series of 14 patients, IAC had inconsistent effects on the CPP.12 Despite these hemodynamic inconsistencies, four clinical trials13 comparing IAC-CPR and standard CPR demonstrated greater rates of initial successful resuscitation and a trend toward an increased survival rate to hospital discharge in the IAC-CPR group, including two in-hospital randomized trials.14,15 The first found statistically greater rates of return of spontaneous circulation (ROSC), 24-hour survival, and survival to discharge in 48 of 103 patients randomized to IAC-CPR compared with standard CPR.14 The other trial (from the same investigators and institution) found significantly more ROSC and 24-hour survival with IAC-CPR compared with standard CPR in patients with initial rhythms of asystole or pulseless electrical activity during their in-hospital cardiac arrests.15 Pooled data from these two separate randomized trials showed a 24-hour survival benefit for IAC-CPR (33% vs. 13%). One pediatric case report16 described intra-abdominal trauma, but none of the adult trials have found an increased incidence of CPR-induced trauma. Per the recommendations from International Liaison Committee on Resuscitation (ILCOR), IAC-CPR may be considered for in-hospital resuscitations when sufficient trained personnel are available (class IIb), but there is no convincing evidence that it is superior for out-of-hospital resuscitation; it is therefore not recommended for in that setting.
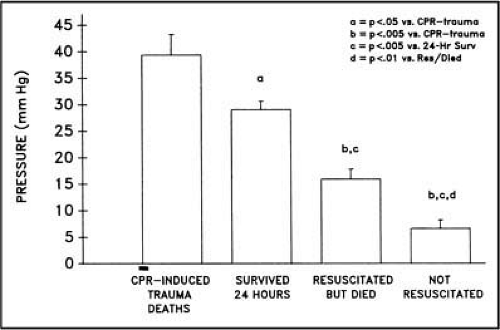 Figure 10-1 • Mean coronary perfusion pressure during CPR for those not resuscitated, resuscitated but not surviving, 24-hour survivors, and those suffering CPR-induced traumatic deaths. Note that the highest CPPs were among those suffering the traumatic injuries. (From Kern KB, Ewy GA, Voorhees WD, et al. Resuscitation 1988;16:246, with permission. © Elsevier 1988.) |
 Figure 10-2 • Multirescuer performance of interposed abdominal compression (IAC) CPR. |
High-Frequency (Rapid Compression Rate) CPR
Whether done manually or mechanically, rapid chest compressions (>100/min) can improve CPP and other measures of resuscitation hemodynamics.17,18,19 However, no clinical studies have shown improved outcome with this technique. Currently this alternative CPR method is given a class indeterminate rating by ILCOR.
Mechanical Piston Devices
Mechanical piston devices typically compress the sternum by a gas-powered piston, the prototype being the Thumper (Fig. 10-3). Experimental studies examining resuscitation hemodynamics achieved with such mechanical piston devices have found mixed results.20,21 One prospective randomized clinical trial and two crossover-design clinical trials have found increased end-tidal carbon dioxide or mean arterial pressure compared to standard manual CPR.20,22,23 The recognized advantage of such devices is in sustaining resuscitation efforts where manual chest compressions may not
be feasible, i.e., during transport, etc. (the ILCOR recommendation for such an indication is IIb). No long-term survival benefit had yet been shown.
be feasible, i.e., during transport, etc. (the ILCOR recommendation for such an indication is IIb). No long-term survival benefit had yet been shown.
 Figure 10-3 • Mechanical piston (Thumper) CPR. |
LUCAS CPR
Another mechanical piston variation, the Lund University Cardiopulmonary Assist System (LUCAS), is also currently being evaluated. This device incorporates a gas-driven piston combined with active decompression (Fig. 10-4). LUCAS CPR produces greater perfusion pressures and resuscitation rates in experimental animals than a standard, commercially available pneumatic piston device.24 Numerous case reports suggest that this device can support adequate circulation during cardiac arrest for substantial periods.25,26 Like the load distributing board (LDB), LUCAS CPR has not been evaluated by ILCOR to date.
 Figure 10-4 • LUCAS mechanical CPR device (Jolife AB; distributed by Medtronic). |
Simultaneous Ventilation– Compression CPR
Based on the theory of the thoracic pump generating blood flow during resuscitation efforts, this technique was found to provide increased peak aortic pressures (“systolic”) and carotid blood flows.27 It is performed using an altered Thumper mechanical compressor and ventilator, where each time the piston compresses the chest, a simultaneous ventilation is also administered. Experimental evidence was mixed,27,28 and in an out-of-hospital study in Dade County, Florida, SVC-CPR failed to improve outcome; indeed, outcome was worse than with standard CPR (hospital discharge: 49 of 337 or 14.5% in the control group and 28 of 365 or 7.7% in the SVC-CPR group; P <0.001).29 This alternative form of CPR is not currently recommended.
Active Compression–Decompression CPR
Active compression–decompression CPR (ACD-CPR) uses a handheld “suction cup” device applied to the anterior sternum. ACD-CPR pulls the anterior chest outward during the relaxation or release phase of chest compressions (Fig. 10-5). In contrast, standard CPR allows passive thoracic recoil
between compressions. The active “diastolic” component of ACD-CPR generates an increased negative intrathoracic pressure resulting in a lower diastolic right atrial pressure and a greater CPP.30 Several reports in experimental models have shown improved diastolic or relaxation-phase CPP with the use of active compression–decompression CPR when compared to standard CPR.31 Clinical trials with this device have shown conflicting results regarding outcome benefits when compared with standard CPR. The most positive results were seen in Paris, where 1-year survival rates were significantly better with ACD-CPR (17 of 373, or 5%) than with standard CPR (7 of 377, or 2%).32 Another clinical trial, in Canada,33 did not show such a benefit. A meta-analysis of 12 clinical trials (n = 4,165 out-of-hospital patients and n = 826 in-hospital patients) failed to show any survival benefit for ACD-CPR.34 Rigorous training and frequent changing of rescuers when performing ACD-CPR are important factors in achieving good results with this alternative resuscitation technique. Some studies have shown an increase in rib fractures with this technique. ILCOR has given this alternative technique the same IIb recommendation as that given to IAC-CPR.
between compressions. The active “diastolic” component of ACD-CPR generates an increased negative intrathoracic pressure resulting in a lower diastolic right atrial pressure and a greater CPP.30 Several reports in experimental models have shown improved diastolic or relaxation-phase CPP with the use of active compression–decompression CPR when compared to standard CPR.31 Clinical trials with this device have shown conflicting results regarding outcome benefits when compared with standard CPR. The most positive results were seen in Paris, where 1-year survival rates were significantly better with ACD-CPR (17 of 373, or 5%) than with standard CPR (7 of 377, or 2%).32 Another clinical trial, in Canada,33 did not show such a benefit. A meta-analysis of 12 clinical trials (n = 4,165 out-of-hospital patients and n = 826 in-hospital patients) failed to show any survival benefit for ACD-CPR.34 Rigorous training and frequent changing of rescuers when performing ACD-CPR are important factors in achieving good results with this alternative resuscitation technique. Some studies have shown an increase in rib fractures with this technique. ILCOR has given this alternative technique the same IIb recommendation as that given to IAC-CPR.
Related posts:
 Emergency Department Management of Acute Coronary Syndromes
Emergency Department Management of Acute Coronary Syndromes
 Heart Failure and Acute Pulmonary Edema in the Emergency Department
Heart Failure and Acute Pulmonary Edema in the Emergency Department
 Restoring Life: The Story of Human Defibrillation and Modern CPR
Restoring Life: The Story of Human Defibrillation and Modern CPR
 Oxygen Administration and Supraglottic Airways
Oxygen Administration and Supraglottic Airways
 Life-Threatening Arrhythmias: Evaluation, Identification, and Assessment
Life-Threatening Arrhythmias: Evaluation, Identification, and Assessment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


