Heart Failure and Acute Pulmonary Edema in the Emergency Department
W. Frank Peacock
HF is a syndrome, and no single test defines the diagnosis. At initial presentation, it may be difficult to accurately diagnose HF, and integration of clinical and laboratory parameters may be necessary to refine diagnosis and prognosis. In one primary care study, the initial diagnosis was falsely positive in over 50%. When symptoms attributed to heart failure develop and are mild to moderate, annual mortality is 5% to 10%; if symptoms are severe, annual mortality increases to 30% to 40%.
Diagnostic considerations in acute heart failure
Initial differential diagnosis using B-type natriuretic peptide (BNP) and N-terminal proBNP (NTproBNP)
Therapy considerations for diuretic therapy, vasodilator therapy, and noninvasive positive pressure ventilation
Risk stratification for discharge and short-stay management
Introduction
The United States is currently experiencing a heart failure (HF) epidemic. With 4.7 million cases and approximately 550,000 new patients each year,1 HF represents the single greatest expense for the Centers of Medicare and Medicaid Studies (CMS). Although HF can occur at any age, it is primarily a disease of the aged. While less than 1% of Americans <50 years of age carry a HF diagnosis, the prevalence doubles each decade until, by the age of 80 years, nearly 10% carry the diagnosis. Among those >65 years, HF is the most common cause of hospitalization,1 accounting for nearly 1 million annual hospitalizations. Furthermore, HF is a disease of recidivism, with up to 60% of patients discharged with HF being rehospitalized within 6 months due to recurrent decompensation.2 As demographic trends predict, the population over age 65 will double in the next 30 years; therefore, the impact of HF is expected to increase significantly as well. Estimated to exceed $27 billion dollars, the current annual U.S. costs for HF care approximately double that of any cancer diagnoses.2
Prognosis
The diagnosis of HF is associated with a very poor long-term prognosis. Once diagnosed with HF, the annual death rate is 18.7%.2 After the development of symptoms, 2-year mortality approximates 35%; over the following 6 years, this increases to 80% for men and 65% for women.1 Outcome is predicted by symptom severity. When symptoms attributed to heart failure develop and are rated as mild to moderate, annual mortality is 5% to 10%. However, if symptoms are considered severe, annual mortality increases to 30% to 40%. Finally, after an episode of pulmonary edema, only half survive a year; if diagnosed with cardiogenic shock, as many as 85% die within 7 days.2
The New York Heart Association (NYHA) HF classification is a commonly used prognostic scale and is reported in the majority of published HF studies. Although it is limited by excluding asymptomatic HF and has poor sensitivity and high interobserver variability, it is a strong mortality predictor. Once a
patient is determined to be NYHA class IV, 1-year mortality exceeds 50%. The newer American Heart Association (AHA) scale includes risk factors as an integral part of the rating system, thus recognizing the fact that earlier intervention has the greatest potential for morbidity and mortality reduction (see Table 6-1).3
patient is determined to be NYHA class IV, 1-year mortality exceeds 50%. The newer American Heart Association (AHA) scale includes risk factors as an integral part of the rating system, thus recognizing the fact that earlier intervention has the greatest potential for morbidity and mortality reduction (see Table 6-1).3
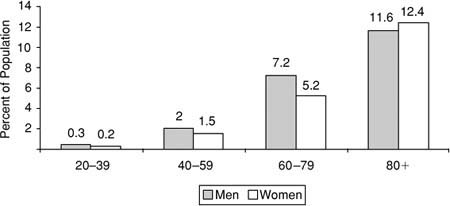
Table 6-1 • Heart Failure Classifications and Stages | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
Pathophysiology
Heart failure may present acutely because of pump dysfunction occurring in the setting of myocardial infarction. In this scenario, loss of a critical amount of functional myocardium results in immediate symptoms. If symptomatic hypotension exists, as a result of inadequate perfusion, cardiogenic shock is diagnosed (see Chapter 7). Heart failure may present precipitously as acute pulmonary edema (APE). Also referred to as acute heart failure syndrome, pulmonary edema is the final manifestation of a reflexively increased systemic vascular resistance (SVR) having the effect of a rapidly decreasing cardiac output (CO) as a compromised myocardium is unable to match the increased workload. By this mechanism, even small elevations of blood pressure (BP) can result in a decreased CO. Decreasing CO triggers further increases in SVR, which worsens the downward spiral. APE can present rapidly with severe symptoms, and if the elevated SVR is not promptly reversed, death or respiratory failure/arrest may result.
Heart failure may also manifest insidiously as the final consequence of pathologic neurohormonal and hemodynamic reflexes initiated by myocardial injury or stress. Threats to CO trigger a neurohormonally mediated cascade that includes activation of the renin-angiotensin-aldosterone system and the sympathetic nervous system. Levels of norepinephrine, vasopressin, endothelin (a potent vasoconstrictor), and tissue necrosis factor are increased. Although not available clinically, the levels of these hormones directly correlate with HF mortality. The clinical consequences of neurohormonal activation are sodium and water retention and increased SVR. These mechanisms may maintain BP and perfusion, but at the cost of increased myocardial workload, wall tension, and myocardial oxygen demand. While some patients are initially asymptomatic, the mechanisms for cardiac remodeling, the final pathologic stage, are in place. “Remodeling” refers to a change in size, shape, and function of the left ventricle (LV) in response to damage or stress. The process is an attempt to compensate for a decline in LV function. Ultimately, the results of remodeling determine future hemodynamics and therapies.
Systolic versus Diastolic Heart Failure
Myocardial wall tension is described by the law of LaPlace as the product of pressure (afterload) and the ventricular radius. Increased tension is believed to be the stimulus for cardiac remodeling. Initially, myocytes hypertrophy or die (apoptosis) and form scar tissue. The dominant response determines HF type. Thus, HF represents the common final pathway of myocardial injury, which may be the result of many different pathologies (Table 6-2).
HF is classified as systolic or diastolic by the measurement of ejection fraction (EF), which is normally 55%–75%. Determining the etiology for diastolic dysfunction is rarely an ED task, but the workup may be initiated in observation or an acute care unit. Systolic dysfunction, defined as an EF <45%, is most commonly from ischemic heart disease, but other etiologies in order of frequency include hypertension, cardiomyopathies, valvular heart disease, and myocarditis.4 Mechanistically, the ventricle has difficulty ejecting blood. Impaired contractility leads to increased intracardiac volumes, with pressure and afterload sensitivity. With circulatory stress (e.g., walking), failure to improve contractility, despite increasing venous return, results in increased cardiac pressures, pulmonary congestion, and edema.
Table 6-2 • Common Causes of Heart Failure and Pulmonary Edema | |
|---|---|
|
In diastolic HF, also referred to as preserved systolic function, contractile function is preserved and the EF is normal or higher. The main pathology is impaired ventricular relaxation, causing an abnormal relation between diastolic pressure and volume. This results in a LV that has difficulty receiving blood. Decreased LV compliance necessitates higher atrial pressures to ensure adequate diastolic LV filling and results in preload sensitivity. The frequency of diastolic dysfunction increases with age, and is more common in elderly women. Chronic hypertension and LV hypertrophy are often responsible for this condition (see Table 6-3). Coronary artery disease also contributes, as diastolic dysfunction is an early event in the ischemic cascade.
As many as 30% to 50% of elderly HF patients have circulatory congestion on the basis of diastolic dysfunction.5 Treatment for volume overload, the most common ED presentation, is the same irrespective of EF. However, because patients with diastolic dysfunction are preload-dependent, excessive diuresis or venodilation may exacerbate the underlying deficit in ventricular filling and cause hypotension. After hemodynamics are stabilized and congestion resolved, treatment of diastolic dysfunction requires consideration of the underlying etiology. Determining HF type is difficult from the history and physical examination; consequently an echocardiogram is usually necessary and recommended as an initial diagnostic step. A combination of diastolic BP ≥105 mm Hg and the absence of jugular venous distention (JVD) has a specificity of 100% but only a 30% sensitivity for indicating preserved LV contractility.6
Table 6-3 • Diastolic HF Etiologiesa | ||
|---|---|---|
|
Some differentiate left- from right-sided HF. Isolated left-sided HF is associated with dyspnea, fatigue, weakness, cough, paroxysmal nocturnal dyspnea, and orthopnea in the absence of peripheral edema, JVD, or hepatojugular reflux. Right-sided HF typically includes peripheral edema, JVD, right-upper-quadrant pain, and hepatojugular reflex without pulmonary symptoms. When abnormal pressure and chamber volumes exist, they will eventually be reflected to the contralateral side. Thus, untreated or poorly controlled left-sided HF will contribute to the genesis of right heart failure and is the most common cause. With isolated right-sided HF (e.g., right ventricular infarct), left-sided HF is less likely but can eventually occur. This traditional distinction of right versus left HF, although often mentioned, does not have great bearing on the ED management, as volume overload is addressed uniformly regardless of the underlying dysfunction. The right-left distinction has greatest applicability when there is suspicion of valvular heart disease or right ventricular infarction.
High-output HF can occur when the normally intact myocardium is unable to meet excess functional demands. These instances are relatively uncommon but include anemia, thyrotoxicosis, large atrioventricular shunts, beriberi, and Paget’s disease of the bone. The appropriate treatment for these conditions is symptomatic while addressing the causative pathology.
Diagnosis
HF is a syndrome, and no single test defines the diagnosis. Thus, at initial presentation, it may be difficult to accurately
diagnose HF. In one primary care study, the initial diagnosis was falsely positive in over 50% of cases. Reasons for misdiagnosis were attributed to obesity, unsuspected cardiac ischemia, and exacerbation of pulmonary disease.7 Gender also contributes to diagnostic errors. Rates of an initially correct HF diagnosis are reported as low as 18% in women and 36% in men.7,8 In the 1,500-patient Breathing Not Properly study, based on history and physical alone, the ED HF diagnosis was correct in 74%.9
diagnose HF. In one primary care study, the initial diagnosis was falsely positive in over 50% of cases. Reasons for misdiagnosis were attributed to obesity, unsuspected cardiac ischemia, and exacerbation of pulmonary disease.7 Gender also contributes to diagnostic errors. Rates of an initially correct HF diagnosis are reported as low as 18% in women and 36% in men.7,8 In the 1,500-patient Breathing Not Properly study, based on history and physical alone, the ED HF diagnosis was correct in 74%.9
Table 6-4 • Framingham Criteria for the Diagnosis of Heart Failure | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Consideration of established criteria may assist in making a diagnosis. The Framingham criteria,10,11 using history and physical findings, require at least one major and two minor criteria for a HF diagnosis (see Table 6-4). The Boston criteria (see Table 6-5) add chest x-ray (CXR) to the history and exam.12 More points give higher probabilities for HF. A score ≥4 correlates with a pulmonary artery occlusion pressure (PaoP) ≥12 mm Hg and has a sensitivity and specificity of 90% and 85%, respectively. These diagnostic criteria are validated but have limited predictive capability when the patient is asymptomatic.
Table 6-5 • Boston Criteria for the Diagnosis of Heart Failure | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
History and Physical Examination
An acute pulmonary edema presentation is typically characterized by severe respiratory distress. Additionally, relative hypertension and cool diaphoretic skin are common. Auscultation will identify rales, which may exist over most of the lung fields. JVD is often marked, but the presence of peripheral edema is variable. The acute HF syndrome can be challenging to diagnose. It occurs in a population of patients at risk for many comorbidities, and errors in diagnosis are further compounded by a lack of more definitive testing available in real time (e.g., echocardiography). In the post-NP assay era, the ED HF misdiagnosis rate is reported as 18%.9 Errors still occur because neither history nor physical examination are completely accurate in diagnosing HF13,14 (Table 6-6).
The physical finding most suggestive of an elevated pulmonary capillary wedge pressure (PCWP) is the S3, which has a specificity of 99%. However, using a stethoscope for detection, its sensitivity is only 20%.13,14 Newer technology utilizing digital microphone detection obtained at the time of ECG performance provides sensitivity and specificity of 40% and 90%, respectively. When detected in patients suspected of having heart failure, the presence of an S3 should raise concern, as outcomes are markedly worsened, including a doubling of 90-day mortality. In similar patients, JVD has a specificity of 94% and a sensitivity of 39% for identifying patients with an elevated PCWP. In other studies, reported confounders impeding a correct HF diagnosis include obesity, deconditioning, and female sex.13
Table 6-6 • Sensitivity of History and Physical Findings for a Diagnosis of Heart Failure | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Chest Radiography
Although the diagnostic “gold standard” for HF is echocardiography,15 the lack of technologic and performance expertise limits its use for this purpose in most EDs (see Chapter 8 Ultrasonography in ED). Thus other measures are required. Chest radiographs (CXR) are easily obtained but are insensitive for evaluating cardiopulmonary status. While a normal CXR does not exclude abnormal LV function, it can help eliminate other diagnoses in the differential (e.g., pneumonia). The radiographic findings of left-side HF are, in descending order of frequency, dilated upper lobe vessels, cardiomegaly, interstitial edema, enlarged pulmonary artery, pleural effusion, alveolar edema, prominent superior vena cava, and Kerley lines.16 Because acute abnormalities lag the clinical appearance by up to 6 hours, CXR should not necessarily delay therapy.
With at least 75% of HF presentations having a prior diagnosis of HF, chronic HF presentations are common in the ED. In this population the CXR signs of congestion have unreliable sensitivity, specificity, and predictive value in identifying patients with high PCWP.17 Radiographic pulmonary congestion is absent in 53% of patients with mild to moderately elevated PCWP (16–29 mm Hg) and in 39% of those with markedly elevated PCWP (>30 mm Hg).17 Cardiomegaly can assist in a diagnosis of HF. However, while a cardiothoracic ratio >60% is associated with increased 5-year mortality, the CXR can be insensitive for this finding owing to intrathoracic cardiac rotation. In fact, in a study of echocardiographically proven cardiomegaly, 22% of patients had a normal cardiothoracic ratio.18
CXR technique affects its performance. Pleural effusions can be missed, especially if obtained with the patient supine. The sensitivity, specificity, and accuracy of the supine CXR were 67%, 70%, and 67%, respectively.19 Although the portable CXR is commonly used in the ED, its sensitivity for HF is poor. When HF symptoms were rated as mild, only the finding of dilated upper lobe vessels was reported in more than 60% of patients.
Despite its limitations, the ED CXR is helpful because it is noninvasive and relatively inexpensive and can be performed rapidly, even at the bedside. The frequency with which the CXR reveals findings of HF increases with HF severity. With severe HF symptoms, the CXR finding consistent with HF occurred in at least two-thirds of patients.16 The radiographic exceptions were Kerley lines and a prominent vena cava, present in only 11% and 44% respectively. The diagnosis of HF is reassuringly less likely in the absence of any CXR findings of HF or significant abnormalities in vital signs and pulse oximetry.
Natriuretic Peptide Assay
Natriuretic peptides (NPs) are the endogenous counterregulatory arm to the pathologic neurohormonal activation that occurs in HF. Four types are recognized: atrial NP, primarily secreted from the atria; B-type NP (BNP), secreted mainly from the cardiac ventricle; CNP, localized in the endothelium; and DNP, possibly of renal origin. NPs result in vasodilation, natriuresis, decreased endothelin, and inhibition of both the renin-angiotensin-aldosterone system and the sympathetic nervous system. BNP is the only NP for which an assay is currently available for clinical use in the ED. Because elevated levels of neurohormones portend a worse prognosis in HF, their attenuation provides the theoretical basis for most therapies proven to delay HF morbidity and mortality. These include treatment with angiotensin converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), aldosterone antagonists, beta-blockers, and nesiritide.
B-type natriuretic peptide (BNP), discovered approximately 20 years ago and available for less than a decade as an assay, has become the one of the most common ED tests for the evaluation of suspected acute decompensated HF (ADHF). BNP measurement offers improved diagnostic accuracy in the setting of suspected HF. Synthesized as pre-proBNP in the myocyte as a response to elevated ventricular pressure or volume stimulus, it is cleaved by the enzyme corin into active BNP and biologically inert N-terminal proBNP (NTproBNP) fragments. BNP is stored in membrane granules.20 Once released, its half-life is approximately 22 minutes. It is cleared by a C receptor, neutral endopeptidases,21 and to some extent by the kidney.22 NTproBNP undergoes predominately renal elimination, and has a half-life of about 2 hours.
Both proteins are available to be measured clinically. They are elevated in relation to NYHA HF class (Fig. 6-1).23
To obtain both good sensitivity and specificity, natriuretic peptide (NP) measurement must be considered in the context of both a low and high cutpoint. Measures beneath the low cutpoint provide excellent sensitivity and may help exclude a HF diagnosis, and levels above the high cutpoint provide strong specificity, such that a HF diagnosis contributing to the clinical presentation should be considered likely. Thus a gray zone between cutpoints remains and constitutes an area of diagnostic uncertainty. Results of NP testing in the gray zone include conditions resulting in non-HF ventricular strain or pressure overload; e.g., primary pulmonary hypertension, pulmonary embolus, myocardial infarction.
To obtain both good sensitivity and specificity, natriuretic peptide (NP) measurement must be considered in the context of both a low and high cutpoint. Measures beneath the low cutpoint provide excellent sensitivity and may help exclude a HF diagnosis, and levels above the high cutpoint provide strong specificity, such that a HF diagnosis contributing to the clinical presentation should be considered likely. Thus a gray zone between cutpoints remains and constitutes an area of diagnostic uncertainty. Results of NP testing in the gray zone include conditions resulting in non-HF ventricular strain or pressure overload; e.g., primary pulmonary hypertension, pulmonary embolus, myocardial infarction.
Addition of a single BNP or NT proBNP measurement can improve the diagnostic accuracy for acute heart failure compared to clinical judgment alone.
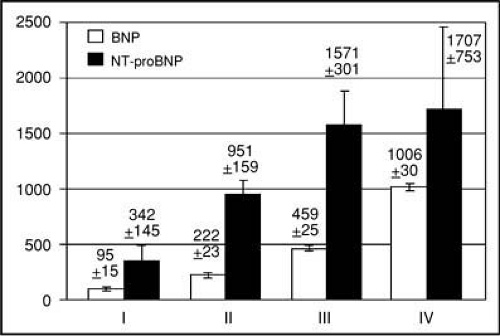 Figure 6-1 • BNP vs. NYHA HF class. (From McCullough PA et al. Rev Cardiovasc Med 2003;4:72–80, with permission.) |
The BNP assay has a range of 0 to 5,000 pg/mL, while the range of the NTproBNP assay is 0 to 35,000 pg/mL. Low and high cutpoints are seen in Table 6-7. If the patient is >75 years of age, per the manufacturer, NTproBNP requires correction. Despite sharing a common synthetic pathway, no consistent relationship between these molecules has been described, so measures of BNP cannot be converted to NTproBNP or vice versa.
NP interpretation requires consideration of the clinical scenario. Besides non-HF conditions known to cause NP elevations into the gray zone, higher levels than clinically predicted are reported in patients with renal failure or insufficiency.24,25 Conversely, BNP levels may be lower than clinically anticipated in two scenarios: (1) despite rapid release, BNP levels may lag by 1 hour or more in the setting of an acute presentation and (2) obesity results in lower BNP concentrations than suggested by the clinical presentation26 (Fig. 6-2).
Table 6-7 • Natriuretic Peptide Cutpoints for Clinical Decision Making | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Finally, patients with chronic HF may have persistently elevated BNP levels, thus requiring consideration of their baseline dry weight BNP to accurately diagnose new symptoms. Although not well studied, in the setting of chronic elevation, changes exceeding 40% to 50% of baseline are considered clinically relevant.
BNP measurement has also demonstrated economic consequence if unavailable in the ED. The Basel trial was a prospective blinded evaluation of BNP in ED patients presenting with dyspnea managed with and without BNP results. BNP testing resulted in a 3.1-day decrease in subsequent length of stay (13.7 vs. 10.6 days) compared with patients in the blinded cohort.27
Beyond diagnosis, several studies describe the prognostic value of ED BNP testing, identifying a population of patients in whom more aggressive therapy or follow-up may be warranted. In the ED, BNP levels >480 pg/mL are associated with a 40% rate of death or HF rehospitalization within the next 6 months versus only 3% if levels were <230 pg/mL.28 In another analysis of hospitalized HF patients, those with an initial BNP >1,740 pg/mL had an acute mortality of 6%, versus only 1.9% if <430 pg/mL29 (Fig. 6-3).
Bioimpedance Measurement
Bioimpedance measurement has been used to aid in the diagnosis and management of patients presenting to the ED with dyspnea and suspected heart failure.30 A noninvasive test that can be performed in the ED, at the bedside, and within minutes of presentation, this technology provides accurate measures of thoracic water content and cardiac output. In a prospective blinded study of patients presenting to the ED with dyspnea, physician knowledge of bioimpedance data resulted in a changed diagnosis in 13% of cases (95% CI 7%–22%), and a change in therapy in 39% (95% CI 29%–50%).
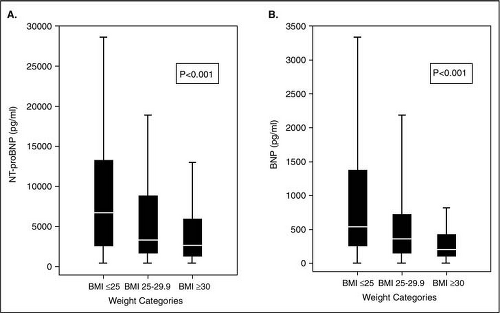 Figure 6-2 • NP levels vs. body mass index. (From Krauser P et al. Am Heart J 2005;149:744–750, with permission). |
Differential Diagnosis
Differentiating HF from other causes of dyspnea is challenging. The differential diagnosis of patients presenting with potential HF (Table 6-8) is confounded by the fact that there are many HF mimics, and these mimics may actually lead to HF or worsen existing HF (Table 6-9). This includes acute myocardial infarction, which must also be considered as a potential cause of a HF exacerbation. A common confounder is coexisting obstructive pulmonary disease. Severe hypertension and peripheral vasoconstriction suggest an acute HF syndrome even in the setting of audible wheezing. Pneumonia and pulmonary embolus can also mimic or exacerbate HF. History and physical examination can help in differentiation, but the CXR and NP assay results may be misleading in the setting of chronic HF. Prior medical records may assist. Edema is seen in HF but is nonspecific, as is noted in hypoproteinemic states, hepatic or renal failure, and vascular diseases.
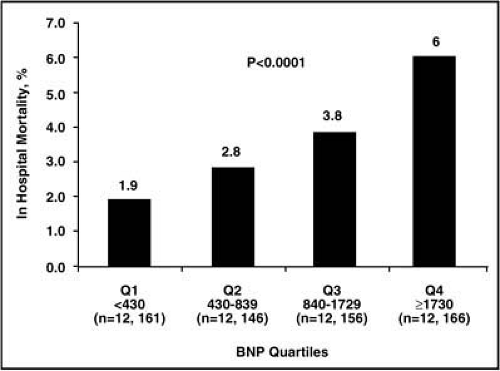 Figure 6-3 • Admission BNP vs. acute mortality in decompensated heart failure. (From Fonarow GC, Peacock WF, Phillips CO, et al for the ADHERE Scientific Advisory Committee and Investigators. J Am Coll Cardiol 2007;49:1943–1950, with permission.) |
Treatment and Stabilization
General Measures
The initial approach is driven by presentation acuity, volume status, and systemic perfusion. If stability is questionable, airway management supersedes all other processes, with therapeutic and diagnostic interventions occurring simultaneously. This is in contrast to the less severely symptomatic patient whose evaluation may be performed in a more stepwise
progression. Initial stabilization is directed at ensuring and maintaining airway control as well as adequate ventilation. Supplemental oxygen use may be guided by pulse oximetry. As the acute risk of hypoxia exceeds that of hypercarbia, O2 should not be withheld for fear of CO2 retention. Arterial blood gas measurements can be helpful in the critically ill and where CO2 retention is a possibility. Endotracheal intubation with mechanical ventilation is indicated if stability is unclear.
progression. Initial stabilization is directed at ensuring and maintaining airway control as well as adequate ventilation. Supplemental oxygen use may be guided by pulse oximetry. As the acute risk of hypoxia exceeds that of hypercarbia, O2 should not be withheld for fear of CO2 retention. Arterial blood gas measurements can be helpful in the critically ill and where CO2 retention is a possibility. Endotracheal intubation with mechanical ventilation is indicated if stability is unclear.
Table 6-8 • Differential Diagnoses for Heart Failure | |
|---|---|
|
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


