Restoring Life: The Story of Human Defibrillation and Modern CPR
Mark E. Silverman
I tried an electric shock directed through the chest to the spine of the back, and not without success; for suddenly it [the bird] rose up and…walked about quietly on its feet.
Efforts to revive the apparent dead with electricity date back over 230 years; however, it is only since the 1960s that defibrillation has become a clinical reality.
The first recorded use of an electrical jolt for resuscitation is a 1774 report by the Royal Humane Society for the Apparently Dead in London in which a limp child was stimulated back to life.
The first portable “defibrillator,” using discharging rods attached to a Leiden jar capacitor, was reported in “An Essay on the Recovery of the Apparently Dead” by Charles Kite in London in 1788.
The need for a universal defibrillator became a research priority in the early twentieth century, when the electrification of homes was accompanied by accidental electrocutions of the public and the company linemen who were up on the poles installing the circuits.
The first successful human defibrillation was performed in 1947 by Claude Beck. Beck was operating on a 14-year-old boy whose heart went into arrest. After cardiac massage and drugs failed, Beck summoned a defibrillator from his experimental laboratory and defibrillated the patient, with a satisfying outcome.
Introduction
The restoration of life to the apparently dead is one of the great stories in medicine. This dream became universally possible with the invention of the defibrillator in the mid-20th century.1,2,3 The story begins in 1672 in Germany, where Otto von Guerike found that a glass globe containing sulfur became charged when rubbed. He had discovered static electricity, which would be harnessed within a glass jar in the next century to deliver powerful shocks. The Leyden jar, invented by Pieter van Musschenbroek in the Netherlands in 1746, provided the first electrical storage device. This corked glass jar, with a central brass rod lined with tinfoil, stored static electricity, which could be released as strong shocks. It soon became popular for scientific, medical, and amusement purposes (Fig. 12-1).
 Figure 12-1 • A Leyden jar capacitor with discharging rods. (Courtesy of the Baaken Library.) |
Early Attempts to Apply Electrical Shocks for Resuscitation
One of the first to experiment with electrical resuscitation was Peter Christian Abildgaard, a Danish physician and veterinarian with a special interest in electricity.4 Abildgaard had observed that animals and men killed by lightning showed little internal damage to explain their death. In 1775, he performed experiments on hens, using shocks from 10 Leyden jars to kill the bird then reviving it from “swooning” with a second shock. He commented: “I tried an electric shock directed through the chest to the spine of the back, and not without success; for suddenly it rose up and…walked about quietly on its feet.”
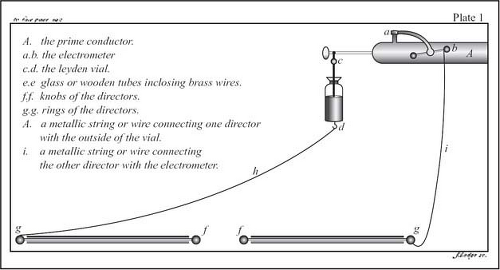 Figure 12-2 • Earliest defibrillator, used by Charles Kite in 1788. The Leyden jar (d) is suspended from the prime conductor (A) and both are connected to directors (f), which are placed on the patient. (Courtesy of the Baaken Library.) |
In the 18th and 19th centuries, sudden death was often due to drowning, asphyxiation, and lightning.2,5 Rescue societies, originating as the Dutch Humane Society in Amsterdam in 1767 and spreading from there to other port cities in Europe, London, and America, organized volunteer resuscitative attempts and reported some early anecdotal success using heat, friction, spirits, smelling salts, fumigation with tobacco smoke instilled in the rectum, and artificial respiration with a bellows. Their enthusiastic efforts were among the first to counteract entrenched concepts about the inevitability of death and to foster important research in this area.1,2
The first recorded use of an electrical jolt for resuscitation is described in a 1774 report by the Royal Humane Society for the Apparently Dead in London, where a limp child was stimulated back to life.5 This success inaugurated the regular application of electricity for such purposes. John Hunter of London, the great comparative anatomist, commented in1776: “Electricity has been known to be of service and should be tried when other methods have failed. It is probably the only method we have of immediately stimulating the heart.”6
The first portable “defibrillator,” using discharging rods attached to a Leyden jar capacitor, was reported in “An Essay on the Recovery of the Apparently Dead” by Charles Kite of London in 1788 (Fig. 12-2). Kite studied records from several hundred cases of drowning and noted that the “recovery of the apparently dead is the length of time that elapses before the proper remedies can be applied.” He also recommended endotracheal intubation.2
In 1809, Allan Burns of Glasgow was recommending the universal application of electricity for sudden death: “Where however, the cessation of vital action is very complete, and continues long, we ought to inflate the lungs, and pass electric shocks through the chest; the practitioner ought never, if the death has been sudden, and the person not very far advanced in life, to despair of success, ’til he has unequivocal signs of real death.”7 Alexandro Volta’s famous dispute with Galvani led to the 1799 invention of the earliest battery, the voltaic pile. This was incorporated into the “reanimation” chair of Richard Reece in about 1820, with the battery attached to the proximal end of a metallic tube inserted into the esophagus of the individual to be revived.2 The
instructions read “In every case of suspended animation, endeavor to restore the functions of the lungs and heart. To accomplish this, extend the patient’s body on the moveable back of the reanimation chair…an assistant should be preparing the Pensile Galvanic Pile…. Having attached the galvanic pile to the top of the chair, one of the wires is to be applied to the tube passing down the gullet, whilst the other is to be successively made to touch different parts of the external surface of the body, particularly about the regions of the heart”2 (Fig. 12-3).
instructions read “In every case of suspended animation, endeavor to restore the functions of the lungs and heart. To accomplish this, extend the patient’s body on the moveable back of the reanimation chair…an assistant should be preparing the Pensile Galvanic Pile…. Having attached the galvanic pile to the top of the chair, one of the wires is to be applied to the tube passing down the gullet, whilst the other is to be successively made to touch different parts of the external surface of the body, particularly about the regions of the heart”2 (Fig. 12-3).
 Figure 12-3 • Reanimation chair of 1820. A metallic tube is inserted into the throat and connected to a voltaic battery hanging above. The dangling wire is touched to the body. (Courtesy of the Baaken Library and Museum, Minneapolis.) |
The Experimental Production and Significance of Ventricular Fibrillation
Ventricular fibrillation was first induced in animals by M. Hoffa and Carl Ludwig in 1850.8 It was not understood as a cause of sudden death in humans until the experiments conducted by John MacWilliam, a professor at Aberdeen, Scotland, in 1885–18879,10,11,12,13,14 (Fig. 12-4). MacWilliam offered experimental proof that “fibrillar contraction” was the cause of sudden death. In 1889, he argued that “sudden cardiac failure does not usually take the form of a simple ventricular standstill in diastole….It assumes, on the contrary, the form of a violent, though irregular and inco-ordinated, manifestation of ventricular energy. Instead of quiescence, there is a tumultuous activity, irregular in its character and wholly ineffective as regards its results.”13 He explained that a variety of pathologic conditions could predispose to ventricular fibrillation, including “degenerative changes of a fatty or fibroid nature in the muscular walls” and “diseased conditions…of the coronary arteries.” MacWilliam also used cardiac compression, artificial resuscitation, and drugs to resuscitate the hearts.
In 1899, Jean Louis Prevost and Frederic Battelli, physiologists in Geneva, Switzerland, induced ventricular fibrillation by passing a weak (40 volt) current through an exposed dog heart or through the chest.15 This was reversed with a repeat, stronger (240–4800 volt) alternating and direct current “countershock.” Their important work, mostly overlooked until 1930, would eventually become crucial to the development of the modern defibrillator by Kouwenhoven.1,2,9 Prevost and Battelli also learned that internal cardiac massage was required to preserve the heart if the second shock was delayed.
 Figure 12-4 • John MacWilliam. (Courtesy of Mr. A. Adam, Honorary Librarian, The Royal Infirmary, Foresterhill, Aberdeen, Scotland.) |
Related posts:
 Emergency Department Management of Acute Coronary Syndromes
Emergency Department Management of Acute Coronary Syndromes
 Heart Failure and Acute Pulmonary Edema in the Emergency Department
Heart Failure and Acute Pulmonary Edema in the Emergency Department
 Circulatory Adjuncts to Improve Coronary Perfusion Pressure
Circulatory Adjuncts to Improve Coronary Perfusion Pressure
 Oxygen Administration and Supraglottic Airways
Oxygen Administration and Supraglottic Airways
 Life-Threatening Arrhythmias: Evaluation, Identification, and Assessment
Life-Threatening Arrhythmias: Evaluation, Identification, and Assessment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


