Seizure Disorders
Henry Cohen MS, PharmD
Salah M. Mesad MD
Seizures are the clinical manifestations of excessive and hypersynchronous, usually self-limiting, abnormal activity of neurons in the cerebral cortex. The behavioral features of a seizure reflect the cerebral cortical areas where the abnormal neuronal activity originates and spreads (Engel, 1989). A convulsion implies a violent, involuntary contraction or series of contractions of voluntary muscles. Epilepsy is a chronic condition characterized by two or more unprovoked recurrent seizures. Epilepsy implies a periodic recurrence of seizures with or without convulsions (Engel, 1989).
ANATOMY, PHYSIOLOGY, AND PATHOLOGY
The excitability of the neuronal cell membrane depends on the maintenance of an electrical charge, or potential difference, between the intracellular and extracellular environments, analogous to the cardiac cell. This is achieved through the maintenance of different concentrations of negatively charged ions on either side of the membrane in the resting state, with the outside having a net positive charge relative to the inside.
The membrane is thus polarized in its resting state, usually with a membrane potential of −60 to at least −80 millivolts. During depolarization, the permeability of the membrane changes to allow positive ions to flow in, eliminating the potential difference. The membrane is subsequently repolarized when the ions that flowed in are pumped back out. The movement of ions during these phases is extremely complex and involves many different channels that are governed by various influences and are operative at different phases of the process (Engel, 1989).
Excitatory postsynaptic potentials generally are caused by excitatory neurotransmitters, which include the excitatory amino acids glutamate and aspartate, acetylcholine, and the less potent histamine and corticotropin-releasing factor (Engel, 1989; Meldrum, 1992). These substances modify Na+, K+, or Ca++ channels to reduce the potential difference across the membrane and facilitate rapid depolarization (Fig. 57-1). Inhibitory postsynaptic potentials are caused by inhibitory neurotransmitters, primarily gamma-aminobutyric acid (GABA) and glycine, and the less potent dopamine, norepinephrine, and serotonin. These substances move K+ out of the cell or Cl− into the cell, increasing the relative intracellular negativity and hyperpolarizing the membrane, making rapid depolarization less likely.
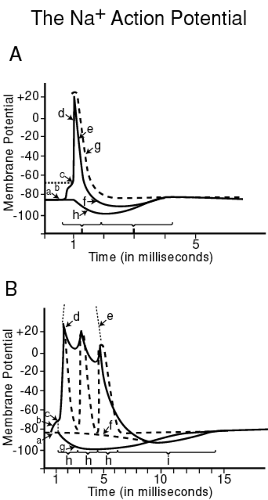 FIGURE 57-1 This graph shows the phases of the Na+ action potential as afterhyperpolarization as recorded at the neuronal cell body (soma). “a” shows the resting membrane potential of approximately −85 mV; “b” shows the phase of graded Na+-mediated depolarization, during which a slow moderate inward flow of Na+ ions begins to reduce the membrane potential; “c” indicates the level of the threshold (approximately −65 mV) at which “explosive” or rapid depolarization “d” occurs; this is also known as the rising phase of the all-or-none regenerative spike. “e” is the repolarization phase, during which the Na+ current “g” and voltage-dependent K+ current “h” reestablish the resting membrane potential; in fact, the potential transiently becomes greater than the resting potential, in the phase known as afterhyperpolarization “f”. “i” indicates the absolute refractory period, and “j” indicates the relative refractory period, during which an appropriate change in the electrophysiologic environment can induce a depolarization to occur prematurely. |
Any imbalance in excitatory or inhibitory influence may lead to hypersynchronous neuronal firing. The action potential spreads to neighboring cells, causing them to fire at the same time and to have concurrent refractory periods. All the neurons emerge from refractoriness simultaneously and are susceptible to firing simultaneously again; the process is thus repeated and perpetuated (Engel, 1989). This coordinated firing spreads until a critical mass is reached and a seizure ensues. The term “seizure threshold” corresponds to the limit beyond which the patient can be made to seize, when subjected to a sufficient number of epileptogenic factors.
During a generalized tonic-clonic seizure, there is a 300% increase in cerebral oxygen consumption and a 900% increase in cerebral blood flow. The increased brain blood flow is necessary to supply neurons with oxygen, glucose, and other necessary nutrients while removing the enormous amounts of carbon dioxide and metabolic waste products. Unfortunately, the brain has a limited capacity to increase brain blood flow, and a state of sequential neuronal hypoxia, anoxia, ischemia, and impending necrosis develops. Hypoxia-induced lactate synthesis causes the production of free radicals (eg, superoxides, peroxides), damaging and destroying the neuronal cells. In patients with status epilepticus (a convulsive seizure or series of seizures lasting longer than 10 to 15 minutes), cardiac collapse and rhabdomyolysis may occur with renal failure as a consequence of prolonged ictal activity (Dodson et al, 1993; DeLorenzo et al, 1992).
EPIDEMIOLOGY
Epilepsy and seizures are among the most common neurologic disturbances. The prevalence of epilepsy ranges from 4 to 8 per 1000. By age 20, about 1% of the population in the United States will have epilepsy, and this cumulative incidence increases to 3% to 4% by 80 years of age (DeLorenzo et al, 1992; Hauser & Annegers, 1992). The annual incidence of epilepsy in the U.S. population is about 50 per 100,000 people (DeLorenzo et al, 1992; Hauser & Annegers, 1992; Hauser et al, 1991). The prevalence of epilepsy increases to 65 per 100,000 people per year if single unprovoked seizures are included, and up to 85 per 100,000 people per year if nonfebrile reactive seizures are added. Of those afflicted, 75% experience their first seizure before the third decade of life (Department of Health, Education & Welfare, 1978).
HISTORY AND PHYSICAL EXAM
The diagnosis of epilepsy is clinical and is based on a detailed description of events experienced by the patient before, during, and after a seizure and, more importantly, on an eyewitness account. Three questions need to be answered when the provider is evaluating a patient with possible epileptic seizures:
Is it epilepsy?
What type of epilepsy?
What is the etiology?
DIAGNOSTIC TESTS
The electroencephalogram (EEG) provides supportive evidence for the clinical diagnosis of epilepsy by demonstrating epilepiform discharges; however, normal studies do not exclude seizures. The EEG aids in the classification of seizures, the selection of appropriate antiepileptic drugs (AEDs), and the analysis of the patient’s response to therapy.
Magnetic resonance imaging (MRI) and computed tomography (CT) of the brain can complement electrophysiologic studies by identifying structural brain lesions that may be causally related to the development of epilepsy. MRI is more sensitive than CT in detecting cerebral lesions related to epilepsy, such as cortical heterotopias or mesial temporal sclerosis, and hamartomas. Some abnormalities, such as calcified or bony abnormalities, may be easier to interpret on CT than MRI. Positron emission tomography and single photon emission computed tomography are less readily obtainable. These techniques can identify areas of cerebral hypometabolism interictally in patients with partial epilepsy, even when MRI and CT have been normal (Engel, 1989).
DIFFERENTIAL DIAGNOSIS
Differentiating epileptic seizures from other paroxysmal nonepileptic events is a common problem. Not all paroxysmal behaviors that include shaking, stiffening, or staring are epileptic seizures. Paroxysmal behavioral changes can result from many different medical, neurologic, and psychiatric disorders. In some cases, these disorders coexist, further confounding the diagnosis and therapy.
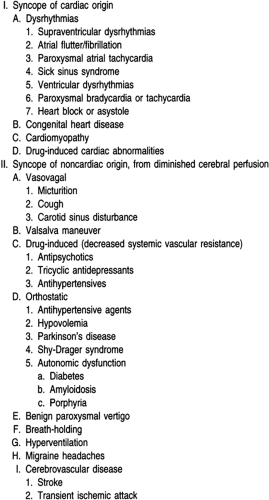
Nonepileptic seizures are common and are reported to occur in approximately 5% to 20% of epileptic outpatients (Commission, 1989; Gates et al, 1991). Patients whose nonepileptic episodes are mistaken for epilepsy face a variety of potential iatrogenic hazards. Patients with undiagnosed nonepileptic seizures usually receive AEDs, whose behavioral toxicity may actually exacerbate nonepileptic seizures (Gates et al, 1991). Physiologic nonepileptic seizures such as syncope are commonly misdiagnosed as seizures (Table 57-1).
 |
Syncope is defined as a sudden transient loss of consciousness resulting from a reduction of cerebral blood flow. It is associated with a loss of postural tone and spontaneous recovery. The diagnosis of syncope is supported if episodes:
Are precipitated by anxiety or pain (eg, venipuncture) or assumption of the upright position
Exclusively occur while standing or sitting
Are associated with pallor and diaphoresis
Are not associated with sustained tonic or clonic movements, bladder incontinence, or tongue or cheek bites
Are not followed by postepisode confusion, lethargy, muscle soreness, and headache.
Although incontinence strongly suggests an epileptic seizure, if the bladder is overdistended when syncope occurs, there also may be incontinence. Prodromal symptoms such as abdominal sensations (eg, “butterflies” or nausea), flushing and warmth, dizziness and lightheadedness, bilateral paresthesia, and a feeling of fear and unreality occur with both syncope and epileptic seizures. Symptoms such as formed visual or auditory hallucinations, olfactory hallucinations, dèjá vu, or focal sensory or motor phenomena strongly suggest partial seizures.
A prodrome lasting several seconds, followed by loss of consciousness for 15 to 60 seconds, followed by a rapid return to a normal level of attentiveness, is typical of syncope. The greatest source of error in distinguishing seizures from syncope is failure to recognize that brief tonic or clonic movements often occur in syncope (convulsive syncope), especially when the patient is maintained in the upright or sitting position (Ziegler et al, 1978; Pacia et al, 1994).
The physical exam in patients with possible syncope includes a brief survey of general medical and neurologic systems, specifically palpation of the pulse and measurement of orthostatic heart rate and blood pressure. An electrocardiogram may help detect abnormalities such as arrhythmias, conduction blocks, and prolonged Q–T syndrome (Pacia et al, 1994).
Classification of Seizures
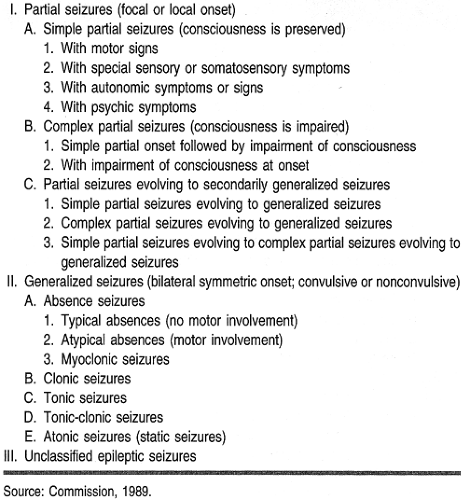
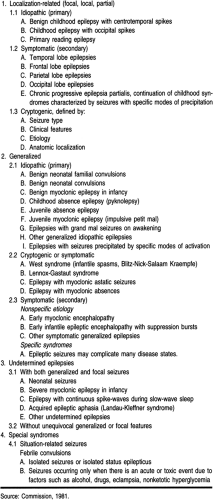
A seizure is not a diagnosis; it is a series of signs and symptoms. Similar seizures can result from multiple underlying cerebral processes. In some cases, seizures are the sole manifestation of the disorder; in others, they are only one of several signs and symptoms present. Certain seizures affect patients of a select age group and produce a characteristic clinical and EEG profile but are idiopathic. The International League Against Epilepsy classifies epileptic seizures based on clinical symptoms and EEG features (Tables 57-2 and 57-3) (Commission, 1989 & 1981). This classification subdivides epileptic seizures into two major categories: partial and generalized. Defining the seizure type and epilepsy syndrome helps determine whether medication is necessary, the likelihood of complete response to AED treatment, and the potential duration of treatment.
 |
 |
Partial seizures have clinical or EEG evidence of a focal onset from one or more areas of the cerebral cortex. Generalized seizures begin in both sides of the brain simultaneously and may arise in subcortical pacemaker regions (eg, thalamus). Partial seizures are subdivided into simple partial seizures (without impairment of consciousness) and complex partial seizures (with impairment of consciousness). A simple partial seizure may evolve into a complex partial seizure, and both types may evolve into a secondarily generalized tonic-clonic (grand mal) seizure. Auras are simple partial seizures.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


